Therapy of arrhythmias
Reading File
Finding Sources
Finding Sources
Searching PubMed
"antiarrhythmic" AND "therapy"
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive information to provide a thorough answer. Let me compile everything:
Therapy of Arrhythmias
Physiological Basis
Arrhythmias arise from two main mechanisms:
-
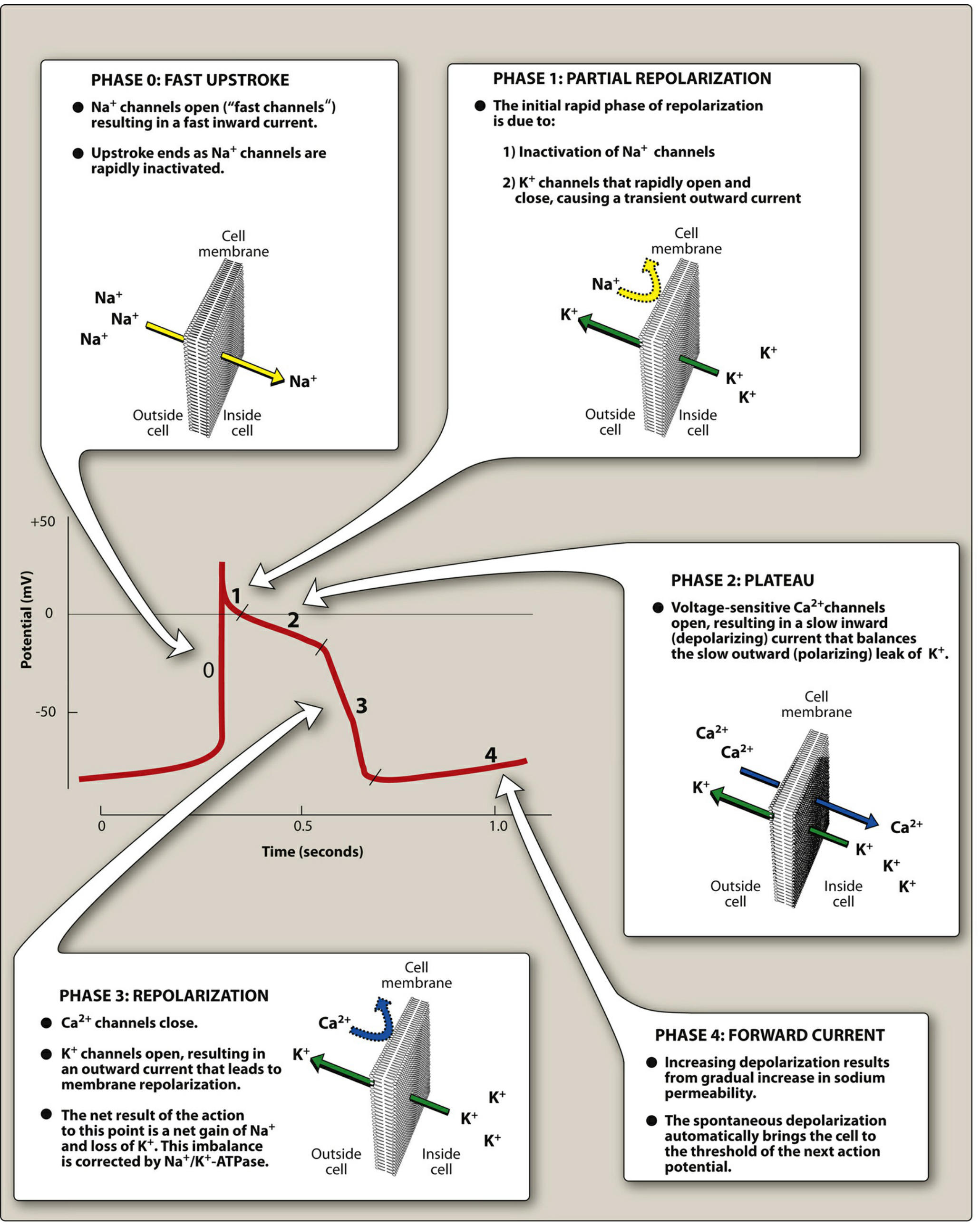
Abnormal automaticity - ectopic pacemaker sites outside the SA node fire due to enhanced phase 4 depolarization. Most antiarrhythmic agents suppress this by blocking Na+ or Ca2+ channels, reducing the ratio of these ions to K+ and flattening the slope of phase 4 depolarization.
-
Reentry - a unidirectional block (from ischemia, scarring, or prolonged refractoriness) creates a circular conduction loop. This is the most common mechanism underlying arrhythmias including atrial flutter, AVNRT, and ventricular tachycardia.
The cardiac action potential has 5 phases targeted by drugs:
Vaughan-Williams Classification of Antiarrhythmic Drugs
Class I - Sodium Channel Blockers
These drugs show use-dependence (state-dependence): they preferentially block cells discharging at high frequency, leaving normal rhythm largely intact. Their use has declined due to proarrhythmic risk, especially in patients with reduced LV function.
| Subclass | Mechanism | Drugs | Key Uses | Major Toxicities |
|---|---|---|---|---|
| IA | Na+ block (intermediate kinetics) + K+ block; slows phase 0, widens AP | Quinidine, Procainamide, Disopyramide | Atrial & ventricular tachyarrhythmias, pre-excited atrial arrhythmias | QT prolongation, torsades de pointes; Quinidine: cinchonism, hemolytic anemia; Procainamide: lupus-like syndrome; Disopyramide: negative inotrope, anticholinergic |
| IB | Na+ block (fast kinetics); shortens phase 3, may shorten AP duration | Lidocaine, Mexiletine | Ventricular tachycardias (acute); prevention of VF post-cardioversion | Neurologic: dizziness, tremor, seizures (lidocaine IV); Mexiletine: nausea/dyspepsia |
| IC | Na+ block (slow kinetics); no change in AP duration | Flecainide, Propafenone | Supraventricular arrhythmias in structurally normal heart | Proarrhythmic - contraindicated post-MI and in structural heart disease (CAST trial) |
- Goodman & Gilman's, Katzung Pharmacology
Class II - Beta-Blockers
Block sympathetic input, slow SA node automaticity and AV nodal conduction velocity.
- Drugs: Metoprolol, Esmolol (IV, short-acting - for acute/peri-operative arrhythmias), propranolol
- Uses: Atrial flutter, atrial fibrillation (rate control), AVNRT, SVT, ventricular rate control
- Toxicity: Bradycardia, hypotension, bronchospasm, fatigue, sexual dysfunction
Class III - Potassium Channel Blockers (Prolong AP and QT)
| Drug | Key Features | Uses | Toxicity |
|---|---|---|---|
| Amiodarone | Blocks IKr, INa, ICa-L, and β-receptors (all 4 classes!) | Serious ventricular arrhythmias (VT/VF), AF, SVT | Pulmonary toxicity, hepatotoxicity, thyroid dysfunction (hypo/hyper), corneal microdeposits, photosensitivity, bradycardia; many drug interactions (CYP metabolism) |
| Sotalol | K+ block + β-blockade | VT, AF maintenance | Torsades de pointes, bradycardia |
| Dofetilide | Pure IKr block | AF cardioversion/maintenance | Torsades (must initiate inpatient with ECG monitoring); renal dose adjustment |
| Ibutilide | K+ channel block + activates inward current (IV only) | Cardioversion of AF/atrial flutter (acute) | Torsades |
| Dronedarone | Amiodarone derivative, multichannel | AF (not permanent AF) - reduces cardiovascular mortality | Less effective than amiodarone; avoid in heart failure |
Class IV - Calcium Channel Blockers (Non-dihydropyridines)
Block L-type Ca2+ channels in the SA and AV nodes.
- Verapamil: Slows SA automaticity and AV conduction; reduces contractility. Uses: SVT, AF/flutter rate control, AVNRT. Oral and IV.
- Diltiazem: Similar to verapamil. IV form used for acute rate control.
- Toxicity: Bradycardia, AV block, hypotension, negative inotropy. Do NOT combine with beta-blockers IV (risk of fatal AV block).
Miscellaneous (Unclassified) Agents
| Drug | Mechanism | Use | Notes |
|---|---|---|---|
| Adenosine | Activates inward K+ rectifier (IK), causing brief complete AV block | Drug of choice for acute PSVT (AVNRT/AVRT) | IV bolus only; duration 10-15 seconds; side effects: flushing, chest tightness, transient dyspnea. Blocked by theophylline; enhanced by dipyridamole |
| Digoxin | Na+/K+-ATPase inhibitor; indirect vagotonic effect on AV node | AF/flutter rate control, SVT | Narrow therapeutic index; toxicity: AV block, bradycardia, GI symptoms, visual disturbances (yellow-green halos); levels elevated by quinidine, amiodarone |
| Magnesium sulfate | Multiple ion channel effects | Torsades de pointes (first-line), digoxin toxicity arrhythmias | IV infusion |
| Atropine | Muscarinic antagonist | Symptomatic bradycardia, AV block | Increases SA node rate |
| Epinephrine | α/β-adrenergic agonist | VF not responding to defibrillation (ACLS) | Used in cardiac arrest |
Drug Therapy by Arrhythmia Type
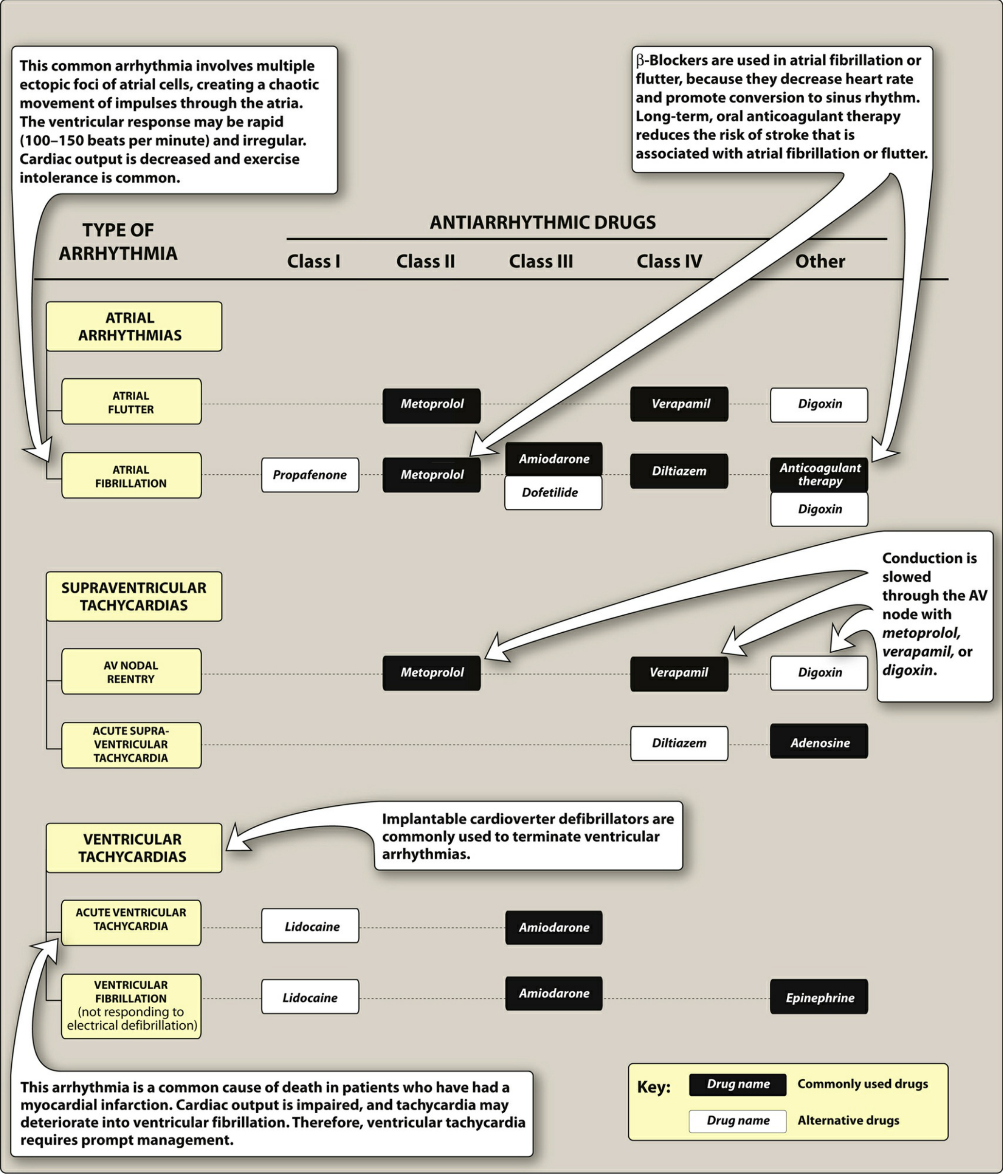
Atrial Fibrillation / Flutter
- Rate control: Beta-blockers (metoprolol), CCBs (verapamil, diltiazem), or digoxin
- Rhythm control / cardioversion: Amiodarone, dofetilide, flecainide/propafenone (only if no structural heart disease), ibutilide (IV, acute)
- Anticoagulation: Long-term oral anticoagulant therapy (warfarin or DOACs) is mandatory to reduce stroke risk
Supraventricular Tachycardias (AVNRT, AVRT)
- Acute: Vagal maneuvers first; then IV adenosine (drug of choice for acute termination); IV verapamil or diltiazem as alternatives
- Chronic prevention: Beta-blockers, verapamil, or catheter ablation (preferred for recurrent cases)
Ventricular Tachycardia (acute)
- Hemodynamically unstable: Immediate DC cardioversion
- Hemodynamically stable: IV amiodarone (preferred) or IV lidocaine
Ventricular Fibrillation
- Electrical defibrillation is first-line and most important
- IV amiodarone or lidocaine if refractory to defibrillation
- Epinephrine during ACLS
Torsades de Pointes
- IV magnesium sulfate (first-line)
- Correct electrolyte abnormalities (K+, Mg2+)
- Stop any QT-prolonging drug
- Overdrive pacing if refractory
Bradyarrhythmias / AV Block
- Acute: IV atropine, temporary pacing
- Definitive: Permanent pacemaker implantation
Non-Pharmacological Therapy
| Modality | Description | Indications |
|---|---|---|
| Electrical cardioversion (DC) | Synchronized shock timed to QRS | Hemodynamically unstable AF/flutter, VT with pulse |
| Defibrillation | Unsynchronized shock | VF, pulseless VT |
| Catheter ablation (RFA/cryoablation) | Destroys arrhythmia focus or pathway via catheter | AVNRT, AVRT (WPW), AF (pulmonary vein isolation), typical atrial flutter (CTI), VT |
| Implantable Cardioverter-Defibrillator (ICD) | Detects VT/VF and delivers a shock | Secondary prevention after VT/VF arrest; primary prevention in HF (EF ≤35%) |
| Permanent pacemaker | Electrical pacing of bradycardia | SSS, high-degree AV block, chronotropic incompetence |
| Vagal maneuvers | Carotid massage, Valsalva | Acute SVT (first-line before adenosine) |
Proarrhythmic Risk - Important Principles
All antiarrhythmic drugs carry the risk of causing arrhythmias (proarrhythmia):
- Class IA, III drugs prolong QT and can precipitate torsades de pointes
- Class IC drugs are strongly contraindicated in ischemic heart disease (CAST study showed increased mortality)
- Amiodarone has the lowest risk of torsades despite QT prolongation
- Hypokalemia, hypomagnesemia, and bradycardia potentiate drug-induced torsades
As a result, antiarrhythmic drug prescribing requires:
- Confirming a definitive arrhythmia diagnosis
- Excluding or correcting precipitating factors
- Establishing that benefit outweighs proarrhythmic risk
- Monitoring ECG (QT interval, PR, QRS width)
- Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung Basic & Clinical Pharmacology, 16th ed.; Lippincott Illustrated Reviews: Pharmacology; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.