Explain thoracic divy from bdc
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Thoracic duct
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Thoracic Duct
Overview
The thoracic duct is the largest and principal lymphatic vessel in the body, measuring 38-45 cm long and 2-5 mm in diameter. It serves as the common drainage channel for lymph from the entire body except the right upper extremity, right breast, right lung, and right half of the head and neck (those drain via the right lymphatic duct).
Course and Relations
Here is a detailed diagram showing the thoracic duct's course through the thorax:
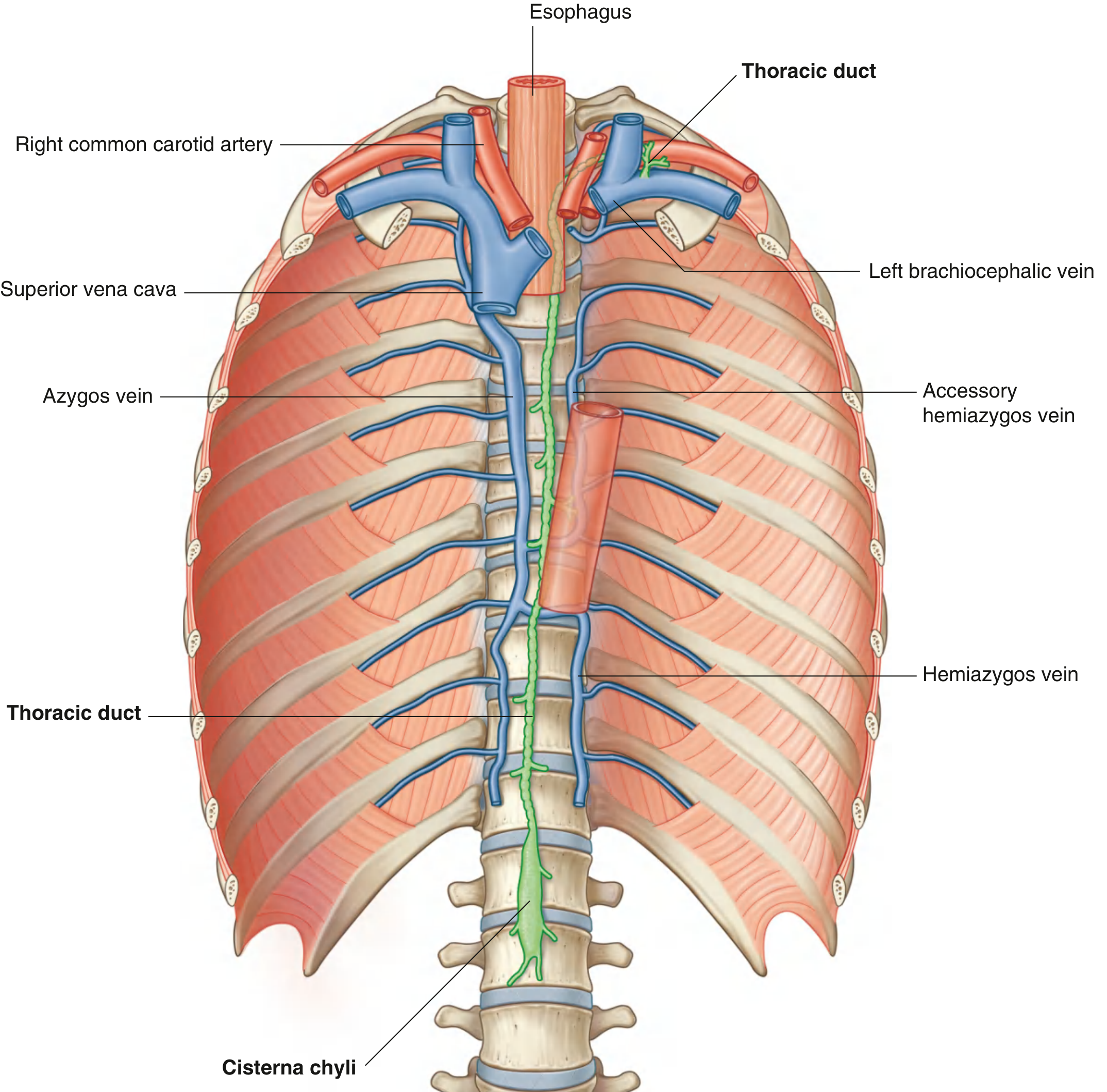
1. Origin - Cisterna Chyli
- Begins at L1-L2 as a saccular dilation called the cisterna chyli (chyle cistern) in the retrocrural abdomen
- The cisterna receives drainage from: abdominal viscera, abdominal walls, pelvis, perineum, and lower limbs
2. Entry into Thorax
- Enters the chest through the aortic hiatus of the diaphragm at T12
- In the posterior mediastinum, it runs to the right of midline between:
- Thoracic aorta on the left
- Azygos vein on the right
- Esophagus anteriorly
- Vertebral bodies posteriorly
3. Crossing the Midline
- At vertebral level T4-T5, the duct crosses to the left and enters the superior mediastinum
- In the superior mediastinum it runs posterior to the arch of the aorta and the initial portion of the left subclavian artery, between the esophagus and the left mediastinal pleura
4. Entry into the Neck
- Arches laterally in the root of the neck, passing posterior to the carotid sheath
- Turns inferiorly in front of the thyrocervical trunk, phrenic nerve, and vertebral artery
5. Termination
- Empties into the junction of the left internal jugular vein and left subclavian vein (left venous angle)
- Just before termination it is joined by:
- Left jugular trunk (drains left side of head and neck)
- Left subclavian trunk (drains left upper limb)
- Occasionally the left bronchomediastinal trunk (drains left thoracic structures)
Tributaries / What it Drains
| Source | Notes |
|---|---|
| Cisterna chyli | Abdomen, pelvis, lower limbs |
| Lower 6-7 intercostal spaces (both sides) | Via descending thoracic lymph trunks |
| Upper left 5-6 intercostal spaces | Via upper intercostal trunks |
| Posterior mediastinal nodes | Direct ducts |
| Posterior diaphragmatic nodes | Direct ducts |
Right Lymphatic Duct (for comparison)
On the right side, three trunks drain independently (or combine into a short right lymphatic duct) into the right venous angle (right internal jugular + right subclavian junction):
- Right jugular trunk (right head and neck)
- Right subclavian trunk (right upper limb)
- Right bronchomediastinal trunk (right thorax + right upper intercostal spaces)
Development (Embryology)
The thoracic duct is formed from:
- The caudal part of the right thoracic duct
- The anastomosis between left and right thoracic ducts
- The cranial part of the left thoracic duct
This embryological origin explains the many anatomical variations seen in the origin, course, and termination of the thoracic duct. The right lymphatic duct is derived from the cranial part of the right thoracic duct.
Clinical Points
- Chylothorax: Injury to the thoracic duct (e.g., during esophagectomy, neck dissection, or aortic surgery) causes chyle to leak into the pleural cavity. Triglycerides >110 mg/dL in pleural fluid is pathognomonic.
- Vulnerability at T4-T5: The crossover point is the most clinically significant level - injuries below T5 typically cause right-sided chylothorax; injuries above T5 cause left-sided chylothorax.
- Surgical ligation: Mass ligation of the thoracic duct at the aortic hiatus (T12) is used prophylactically during transthoracic esophagectomy.
Sources: Gray's Anatomy for Students; Fischer's Mastery of Surgery, 8th ed; The Developing Human - Clinically Oriented Embryology
This is a shared conversation. Sign in to Orris to start your own chat.