Topic : NCV - 15 marks MPT level answer
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the information needed for a complete 15-mark answer. Here it is:
Nerve Conduction Velocity (NCV) Studies
15-Mark MPT-Level Answer (PG Entrance Standard)
1. Definition
Nerve Conduction Velocity (NCV) is the speed at which an electrical impulse travels along a nerve, expressed in meters per second (m/s). NCV studies (also called Nerve Conduction Studies - NCS) are electrophysiological tests that record compound action potentials evoked by transcutaneous electrical stimulation of peripheral nerves.
2. Principle
A supramaximal electrical stimulus is applied to a nerve through skin surface electrodes. This depolarizes all available axons. The resulting action potential is recorded either:
- Over the muscle distally (motor fibers) - compound muscle action potential (CMAP)
- Over the nerve more distally (sensory fibers) - sensory nerve action potential (SNAP)
- Over a mixed nerve proximally - mixed nerve action potential (MNAP)
NCS assesses only medium to large diameter myelinated fibers (motor fibers + sensory fibers carrying vibration and proprioception). Small unmyelinated C fibers (pain, temperature) are NOT assessed.
3. Types of NCS
| Type | Stimulus Site | Recording Site | Potential |
|---|---|---|---|
| Motor NCS | Mixed/motor nerve | Muscle belly | CMAP |
| Sensory NCS (antidromic) | Nerve trunk | Distal digital nerve | SNAP |
| Sensory NCS (orthodromic) | Digital nerve | Nerve trunk | SNAP |
| Mixed NCS | Peripheral nerve | Proximal nerve | MNAP |
| F-wave | Motor nerve (distal) | Muscle | Late response (proximal conduction) |
| H-reflex | Tibial nerve | Soleus | Monosynaptic reflex arc |
Antidromic SNAP recording is used most often clinically because it has technical advantages over orthodromic techniques.
4. Technique and Parameters Measured
Setup
- Cathode (negative electrode) placed closer to recording site; cathode causes depolarization, anode causes hyperpolarization
- Supramaximal stimulation: intensity increased until CMAP/SNAP no longer grows, then current increased an additional 20-30%
Key Parameters
A. Amplitude
- CMAP amplitude: in millivolts (mV); reflects the number of functioning motor axons and innervated muscle volume
- SNAP amplitude: in microvolts (uV); reflects number of sensory axons
B. Distal Latency
- Time (ms) from stimulus to onset of CMAP/SNAP at the distal recording site
- Includes neuromuscular junction delay + muscle depolarization time (in motor studies)
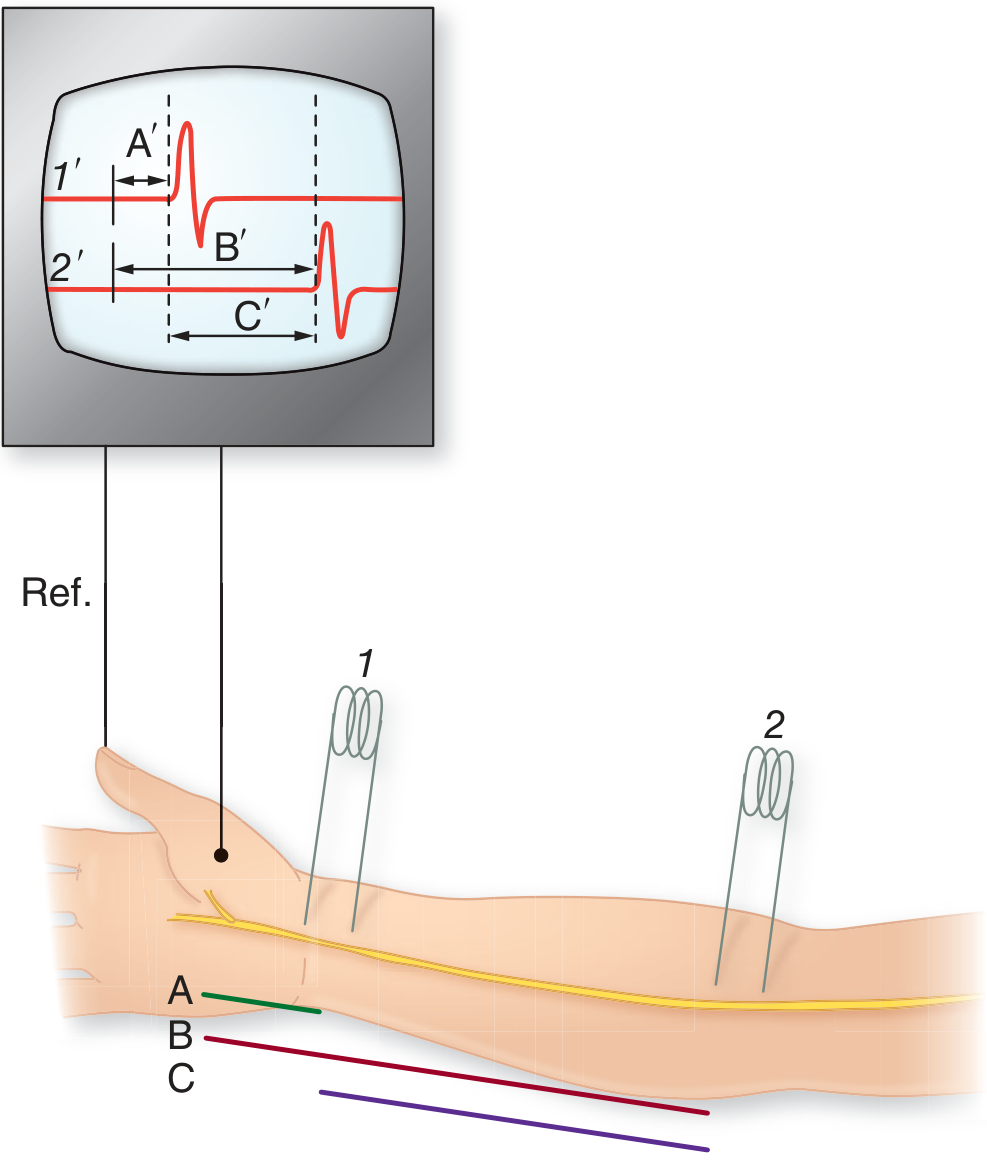
C. Conduction Velocity (CV)
- Calculated by stimulating at two sites and measuring the difference in latencies:
CV (m/s) = Distance between two stimulation points (mm) / Difference in latencies (ms)
This formula eliminates the NMJ delay and muscle depolarization time, giving the true nerve segment velocity.
D. Waveform morphology / Duration / Area
5. Normal Values
| Nerve | Motor CV | Sensory CV | Distal Latency (motor) |
|---|---|---|---|
| Median (upper limb) | 50-65 m/s | 50-65 m/s | < 4.5 ms |
| Ulnar (upper limb) | 50-65 m/s | 50-65 m/s | < 3.5 ms |
| Peroneal (lower limb) | 40-55 m/s | - | < 6 ms |
| Sural | - | 40-55 m/s | - |
General rule: Upper limb NCV = 50-70 m/s; Lower limb NCV = 40-55 m/s (lower limb is 7-10 m/s slower due to longer axons, lower temperature, and shorter internodal distances distally)
6. Factors Affecting NCV
| Factor | Effect |
|---|---|
| Temperature | Each 1°C drop below 38°C slows NCV by ~2.4 m/s (~5%). Cold limbs falsely slow NCV and increase CMAP/SNAP amplitude. Warm to skin temperature > 33°C before testing. |
| Age | NCV is half adult value at birth (incomplete myelination). Reaches adult values by age 3-5 years. Declines ~10% by age 60. |
| Height | Taller individuals have longer nerves with slightly slower NCV (inverse relationship). |
| Nerve segment | Proximal segments conduct faster than distal segments. |
| Gender | Females have slightly higher sensory NCV than males. |
7. Pathological Patterns - Axonal vs. Demyelinating
This is the most important and high-yield concept in NCV interpretation:
| Parameter | Axonal Degeneration | Segmental Demyelination |
|---|---|---|
| CMAP amplitude | Decreased | Normal (unless conduction block) |
| SNAP amplitude | Decreased | Normal or decreased |
| Distal latency | Normal | Prolonged (> 130% ULN) |
| Conduction velocity | Normal or mildly reduced | Markedly slow (< 70% LLN) |
| Conduction block | Absent | Present |
| Temporal dispersion | Absent | Present |
| F wave | Normal or absent | Prolonged or absent |
| Fibrillations on EMG | Present | Absent |
| Motor unit morphology | Reinnervation (large, polyphasic) | Normal |
Key rule: Conduction velocity slows significantly only in demyelination. In axonal loss, velocity is preserved (or only mildly reduced if >50% axons lost).
8. Late Responses
F-Wave
- Antidromic activation travels up to the anterior horn cell; a proportion of motor neurons "backfire" and send an orthodromic impulse back down to muscle
- Records the total round-trip time through the entire motor pathway (including proximal nerve and spinal cord)
- Clinical use: Detects proximal nerve lesions (Guillain-Barre Syndrome early, thoracic outlet syndrome, radiculopathy)
- Normal F-wave latency: ~25-32 ms for upper limb, ~45-56 ms for lower limb
H-Reflex
- Electrical analog of the ankle jerk reflex (monosynaptic)
- Tibial nerve stimulated at popliteal fossa; response recorded from soleus
- Absent H-reflex: S1 radiculopathy, peripheral neuropathy
- Normal latency: 25-35 ms
9. NCV Findings in Specific Diseases
Guillain-Barre Syndrome (GBS) - Acquired Demyelination
- Markedly slowed CV, prolonged distal latencies, conduction block, temporal dispersion
- Nonuniform slowing across segments (distinguishes from hereditary CMT where slowing is uniform)
- Absent F-waves early (proximal conduction block)
- SNAP amplitudes relatively preserved early
Charcot-Marie-Tooth Disease (CMT Type 1) - Hereditary Demyelination
- Uniform, symmetrical slowing of CV (often < 38 m/s in upper limb)
- No conduction block, no temporal dispersion (hereditary vs. acquired distinction)
- Normal CMAP amplitudes early
Diabetic Neuropathy - Axonal (length-dependent)
- Reduced CMAP and SNAP amplitudes, worse in lower limbs
- Normal or mildly slowed CV
- Absent sural SNAP often the earliest finding
- Later stages: absent responses in lower limb nerves
Carpal Tunnel Syndrome (Median nerve entrapment)
- Prolonged distal motor latency (> 4.5 ms) at the wrist
- Slowed or absent median SNAP across the wrist
- Normal conduction across forearm segment
- Classic: "focal" demyelination at carpal tunnel
CIDP (Chronic Inflammatory Demyelinating Polyneuropathy)
- Similar to GBS but chronic: multifocal demyelination, conduction blocks, temporal dispersion
- Acquired pattern = nonuniform slowing
10. NCV in Nerve Injury (Seddon / Sunderland Classification)
| Injury Type | NCV Proximal | NCV Distal (0-10 days) | NCV Distal (> 10 days) | Prognosis |
|---|---|---|---|---|
| Neuropraxia | No response across lesion | Normal | Normal | Good - physiological block only |
| Axonotmesis | No response across lesion | Normal initially | Absent (Wallerian degeneration) | Moderate |
| Neurotmesis | No response | Normal initially | Absent | Poor without surgery |
Key point: Immediately after injury, distal conduction is normal even in axonotmesis/neurotmesis. Wallerian degeneration takes 5-10 days to progress distally - so NCV must be repeated at 10-14 days post-injury to differentiate neuropraxia from axonal injury.
11. NCV vs. EMG - Complementary Tests
| Feature | NCV | Needle EMG |
|---|---|---|
| Assesses | Peripheral nerve | Motor unit / muscle |
| Fiber type | Large myelinated | Motor units |
| Demyelination | Best test | Not specific |
| Axonal loss | Amplitude reduction | Fibrillations, fasciculations |
| NMJ disorders | Limited | SFEMG, repetitive stimulation |
| Myopathy | Normal | Characteristic MUP changes |
12. Clinical Applications / Indications
- Peripheral neuropathy (diabetic, uremic, toxic, hereditary)
- Entrapment neuropathies (carpal tunnel, cubital tunnel, tarsal tunnel)
- GBS and CIDP
- Radiculopathy (with EMG)
- Plexopathy (brachial, lumbosacral)
- Mononeuritis multiplex
- Motor neuron disease
- NMJ disorders (with repetitive nerve stimulation)
- Traumatic nerve injuries (prognosis and timing of surgery)
Summary Mnemonics
CADS - parameters measured: Conduction velocity, Amplitude, Distal latency, Shape (waveform)
"Slow = Demyelination, Small = Axonal"
- Slowed CV + prolonged latency = demyelinating
- Small (reduced) amplitude = axonal loss
Sources: Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology 12th Ed; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E; Campbell's Operative Orthopaedics 15th Ed
Explain in simple language easy to memorize in exam
NCV Studies - Simple & Exam-Ready 🧠
What is NCV? (The Big Idea)
Think of a nerve like a wire. NCV measures how fast electricity travels through that wire.
Normal speed = 50-70 m/s (arms), 40-55 m/s (legs) Legs are slower because the wires are longer and colder.
What Does NCV Measure? → CADS
| Letter | Parameter | Think of it as... |
|---|---|---|
| C | Conduction Velocity | Speed of the car on the highway |
| A | Amplitude | How many cars are on the road |
| D | Distal Latency | Time to reach the first toll booth |
| S | Shape/waveform | What the traffic looks like |
Motor vs Sensory NCS
| Motor NCS | Sensory NCS | |
|---|---|---|
| What you record | CMAP (muscle response) | SNAP (nerve response) |
| Units | millivolts (mV) | microvolts (uV) |
| Direction | Nerve → Muscle | Nerve → Nerve |
Memory trick: CMAP = Car goes to Muscle. SNAP = Sensory Nerve Action Potential
The #1 Most Important Concept
⚡ "SLOW = Myelin problem. SMALL = Axon problem."
DEMYELINATION AXONAL LOSS
(myelin sheath gone) (wire itself lost)
CV is SLOW ✓ CV is NORMAL
Latency is LONG ✓ Latency is NORMAL
Amplitude = normal Amplitude is SMALL ✓
Conduction BLOCK ✓ No conduction block
Temporal DISPERSION ✓ No dispersion
No fibrillations FIBRILLATIONS on EMG ✓
One-line Memory Hook:
"Demyelination = Delay. Axonal = Absent (amplitude)."
Factors That Slow NCV (Exam Traps)
| Factor | Effect | Number to Remember |
|---|---|---|
| Cold | Slows NCV | 2.4 m/s per °C drop |
| Old age | Slows NCV | Reaches adult values by age 3-5; declines after 50 |
| Tall patient | Slightly slower | Long nerves = slower |
| Legs vs arms | Legs slower | 7-10 m/s slower |
Cold trap in exams: A cold limb gives falsely prolonged latency and falsely high amplitude - looks like demyelination but isn't! Always warm limb to >33°C before testing.
Normal Values to Remember
Upper limb nerves: 50 - 70 m/s
Lower limb nerves: 40 - 55 m/s
Median distal latency: < 4.5 ms (carpal tunnel if prolonged)
Late Responses - Simple Version
F-Wave = "The Bouncer"
- Impulse goes UP to spinal cord, bounces back DOWN
- Tests proximal nerve (you can't stimulate there directly)
- Absent/prolonged in: GBS (early sign), radiculopathy
H-Reflex = "Electric Ankle Jerk"
- Electrical version of tapping the Achilles
- Tests S1 nerve root
- Absent in: S1 radiculopathy, peripheral neuropathy
Memory: H = Heel reflex (S1). F = Far away (proximal conduction).
Disease Patterns - The Big 5
1. Carpal Tunnel Syndrome
- Prolonged distal latency of median nerve at wrist (> 4.5 ms)
- Slow SNAP across wrist
- Everything normal above the wrist
- Think: "Traffic jam at the toll booth (wrist)"
2. Diabetic Neuropathy
- Reduced SNAP amplitude (axonal, length-dependent)
- Legs worse than arms
- Sural SNAP - earliest to disappear
- CV normal or mildly slow
- Think: "Wires dying from the tips upward"
3. GBS (Guillain-Barre Syndrome)
- Acquired demyelination - patchy and non-uniform
- Slowed CV + conduction block + temporal dispersion
- F-waves absent early
- Think: "Random potholes on the highway (non-uniform)"
4. CMT Type 1 (Hereditary)
- Uniform demyelination - symmetric slowing
- CV often < 38 m/s
- NO conduction block (this is the key difference from GBS)
- Think: "Evenly bad road (uniform)"
5. Nerve Injury - Neuropraxia vs Axonotmesis
Both injuries:
- Immediately after: Distal conduction = NORMAL
- Wait 10 days!
After 10 days:
Neuropraxia: Distal conduction still NORMAL (just a block)
Axonotmesis: Distal conduction GONE (Wallerian degeneration)
Exam pearl: Never judge axonal injury in the first week. Repeat NCV at 10-14 days.
GBS vs CMT - The Classic Comparison
| Feature | GBS (Acquired) | CMT Type 1 (Hereditary) |
|---|---|---|
| CV slowing | Non-uniform, patchy | Uniform, symmetric |
| Conduction block | YES | NO |
| Temporal dispersion | YES | NO |
| Onset | Acute | Lifelong, slow |
One-liner: "GBS = Patchy road with roadblocks. CMT = Uniformly bad road, no roadblocks."
NCV vs EMG - Two-Second Version
| NCV | EMG (Needle) |
|---|---|
| Tests the wire (nerve) | Tests the motor unit (nerve + muscle) |
| Demyelination: best test | Axonal loss: fibrillations |
| Amplitude = axon count | MUP changes = muscle/nerve disease |
Rule: Do BOTH. NCV and EMG are partners, not alternatives.
Master Flowchart for Any Neuropathy
Neuropathy on NCV?
|
_____|_____
| |
SLOW CV NORMAL CV
| |
Demyelinating Axonal
| |
Uniform? Amplitude reduced?
| |
YES = CMT YES = diabetes, toxins,
NO = GBS/CIDP uremia, B12 deficiency
Quick Revision Table - Exam Day
| Condition | CV | Amplitude | Latency | Block |
|---|---|---|---|---|
| Normal | 50-70 | Normal | Normal | No |
| Axonal neuropathy | Normal | LOW | Normal | No |
| Demyelinating (GBS) | SLOW | Normal | LONG | Yes |
| Carpal tunnel | Normal (forearm) | Normal | LONG at wrist | Focal |
| CMT type 1 | Uniformly SLOW | Normal | LONG | No |
The 5 Things an Examiner Always Asks
- NCV formula? → Distance ÷ Difference in latencies
- What does NCV NOT test? → Small fibers (pain & temperature - C fibers, A-delta)
- Why repeat NCV after 10 days in trauma? → Wallerian degeneration takes 5-10 days
- Cold limb effect? → Slows NCV, mimics demyelination
- GBS vs CMT distinction? → Conduction block + non-uniform slowing = GBS/acquired
Golden Rule for the exam: "Slow and Blocked = Demyelination (GBS/CIDP/CTS) Small and Gone = Axonal (DM/toxin/trauma)"
This is a shared conversation. Sign in to Orris to start your own chat.