Gabapentin can be given in neuropathic pain
Reading File
Finding Sources
Searching PubMed
gabapentin neuropathic pain
Reading File
Reading File
Reading File
Absolutely correct. Here is a detailed breakdown:
Gabapentin in Neuropathic Pain
Mechanism of Action
Gabapentin binds to the alpha-2-delta (α2-δ) subunit of voltage-dependent calcium channels in the dorsal horn of the spinal cord. This reduces the release of excitatory neurotransmitters - particularly glutamate and substance P - thereby dampening central sensitization and hyperalgesia.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2462
Place in Therapy - First-Line Agent
Gabapentin is a recommended first-line co-analgesic for a variety of neuropathic pain conditions, particularly in:
-
Medically ill patients
-
Elderly patients (favorable safety profile, few drug-drug interactions)
-
Bradley and Daroff's Neurology in Clinical Practice, p. 2462
-
Cummings Otolaryngology, p. 598
Evidence-Based Indications
| Condition | Evidence |
|---|---|
| Diabetic peripheral neuropathy | RCT (Backonja et al., 1998) |
| Postherpetic neuralgia | RCT (Rowbotham et al., 1998) |
| Cancer neuropathic pain | Used alongside opioids |
| Chronic pelvic pain / CPPS | Some benefit reported |
| Trigeminal neuralgia | Used as adjunct |
| General nonmalignant neuropathic pain | Multiple trials |
Gabapentin also shows synergism with morphine in neuropathic pain - the combination is more effective than either drug alone.
- Campbell-Walsh Urology, p. 1622
- Harrison's Principles of Internal Medicine 22E, p. 3130
Dosing
- Start: 100-300 mg at bedtime (titrate slowly)
- Therapeutic range: up to 3600 mg/day in divided doses (if tolerated)
- Important: Nonlinear pharmacokinetics - bioavailability decreases as dose increases (saturable intestinal absorption via amino acid transporters)
Common Adverse Effects
- Drowsiness / somnolence
- Dizziness
- Unsteadiness / ataxia
- Peripheral edema at higher doses
Gabapentin vs. Pregabalin
Both are gabapentinoids with the same α2-δ mechanism. Pregabalin has:
- Linear pharmacokinetics (more predictable absorption)
- FDA approval specifically for diabetic neuropathy, postherpetic neuralgia, and fibromyalgia
- NNT of ~2.2 for diabetic neuropathy
- Possibly greater efficacy than gabapentin for neuropathic pain overall
A recent 2024 systematic review and meta-analysis (PMID 39839199) directly comparing the two confirmed both are effective for neuropathic pain, with pregabalin showing some edge in certain conditions.
Key Points
- Gabapentin is not an opioid but is increasingly regulated due to misuse potential
- It does not require hepatic metabolism - renally excreted unchanged, so dose adjustment required in renal impairment
- FDA warning for all anticonvulsants: monitor for mood changes, worsening depression, and suicidal ideation (especially in adolescents and young adults)
- For neuropathic pain, the NNT for any drug ranges from 3-7, meaning trials of 3-4 weeks with alternate drugs or combinations are often necessary
Compare gabapentin vs pregabalin vs duloxetine and also symptoms of neuropathic pain
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
gabapentin pregabalin duloxetine neuropathic pain comparison
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a thorough breakdown covering both topics.
Symptoms of Neuropathic Pain
Neuropathic pain arises from injury or disease affecting the somatosensory nervous system (peripheral or central). The hallmark is a mix of positive and negative sensory phenomena:
Positive Symptoms (exaggerated or spontaneous sensations)
| Symptom | Description |
|---|---|
| Burning pain | Constant deep burning/gnawing sensation - most classic |
| Lancinating/shooting pain | Brief, electric shock-like, shooting quality |
| Allodynia | Pain from a normally non-painful stimulus (e.g., light touch, clothing) |
| Hyperalgesia | Exaggerated pain from a painful stimulus |
| Hyperpathia | Explosive over-reaction to stimuli, often with aftersensation |
| Paresthesias | Tingling, prickling, "pins and needles" |
| Dysesthesias | Unpleasant abnormal sensations (spontaneous or evoked) |
Negative Symptoms (sensory loss)
- Numbness, hypoesthesia, loss of temperature/pain sensation (especially in small-fiber neuropathy)
Other features
-
Worse at night
-
Associated local autonomic dysfunction (skin color, temperature, sweating changes)
-
Often coexists with a sensory deficit in the same territory
-
Adams and Victor's Principles of Neurology, p. 1345
-
Miller's Anesthesia 10e, p. 6835
Drug Comparison: Gabapentin vs Pregabalin vs Duloxetine
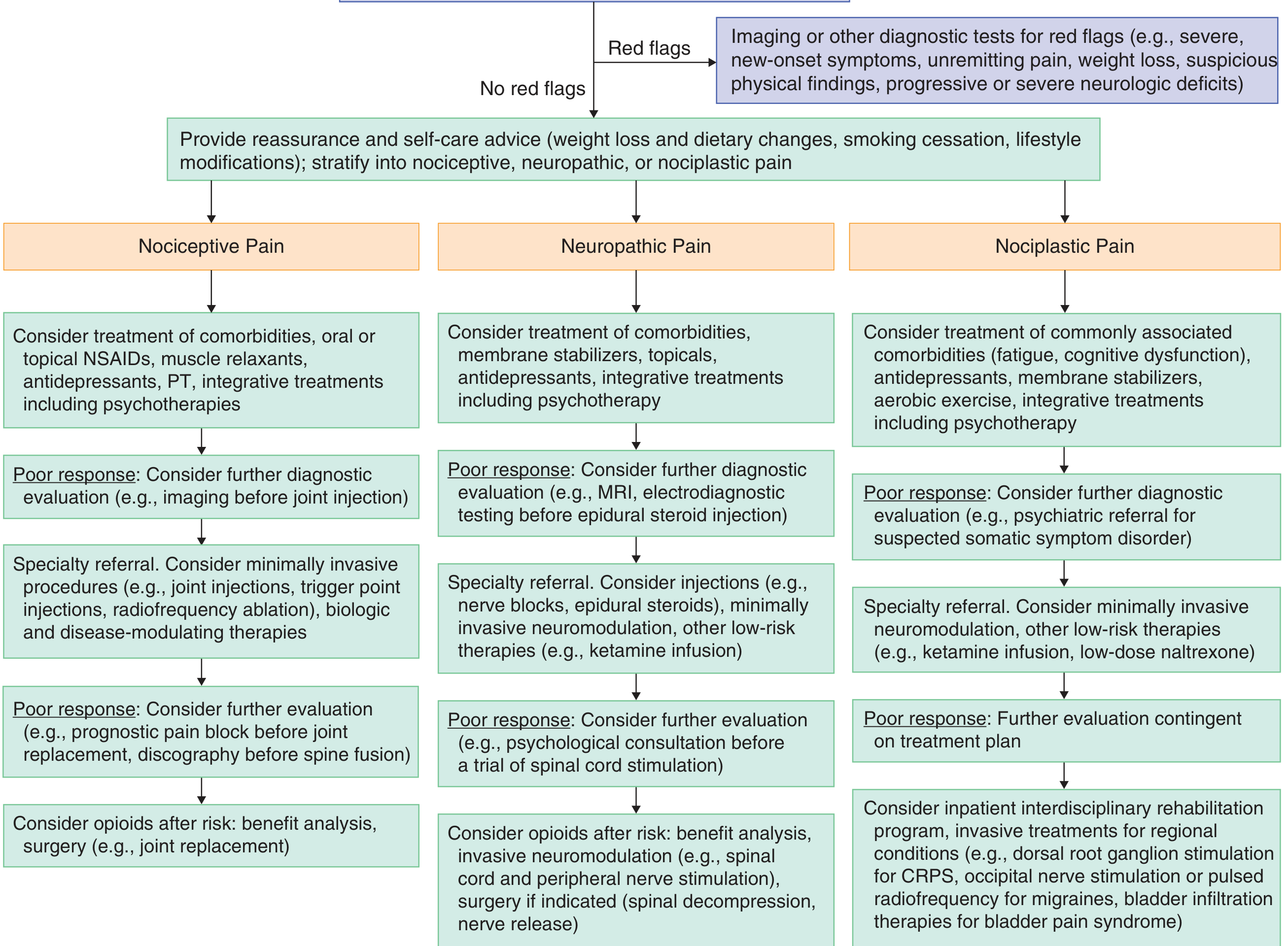
Chronic Pain Approach Flowchart
Side-by-Side Comparison Table
| Feature | Gabapentin | Pregabalin | Duloxetine |
|---|---|---|---|
| Drug class | Gabapentinoid (anticonvulsant) | Gabapentinoid (anticonvulsant) | SNRI antidepressant |
| Mechanism | Binds α2-δ subunit of voltage-gated Ca²⁺ channels → ↓ glutamate, substance P release | Same as gabapentin (α2-δ subunit) | Inhibits presynaptic reuptake of serotonin + norepinephrine; modulates descending inhibitory pain pathways |
| Pharmacokinetics | Nonlinear - bioavailability DECREASES as dose increases (saturable intestinal transporter) | Linear - predictable absorption; food does not significantly affect it | Linear; hepatic metabolism (CYP1A2, CYP2D6) |
| Protein binding | Not protein bound | Not protein bound | ~96% protein bound |
| Half-life | ~5-7 hours | ~6 hours | ~12 hours |
| Elimination | Renal (unchanged) | Renal, 95% unchanged | Hepatic |
| FDA approvals (pain) | Postherpetic neuralgia | Diabetic peripheral neuropathy, postherpetic neuralgia, fibromyalgia, spinal cord injury neuropathic pain | Diabetic peripheral neuropathy, fibromyalgia, chronic musculoskeletal pain |
| Starting dose | 100-300 mg at bedtime | 150 mg/day in 2-3 divided doses | 30 mg/day (can start 20-30 mg) |
| Therapeutic dose | Up to 3600 mg/day | 150-600 mg/day | 60-120 mg/day |
| NNT (diabetic neuropathy) | ~4-6 | ~2.2 (better efficacy) | ~5-6 |
| Best for | General neuropathic pain; elderly; medically ill (few DDIs) | Lancinating/shooting neuropathic pain; also anxiolytic | Diabetic neuropathy; also useful when comorbid depression/anxiety present |
| Renal dose adjustment | YES - required | YES - required | Not renally eliminated; avoid in severe renal failure |
| Hepatic dose adjustment | Not needed | Not needed | YES - contraindicated in hepatic insufficiency |
| Common adverse effects | Drowsiness, dizziness, unsteadiness | Dizziness, sedation, peripheral edema, dry mouth, weight gain | Nausea, dry mouth, dizziness, constipation, increased BP, sweating |
| Drug-drug interactions | Very few | Very few | CYP2D6 interactions; avoid MAOIs (serotonin syndrome) |
| Additional uses | Epilepsy, anxiety | Epilepsy, generalized anxiety disorder | Depression, generalized anxiety disorder, stress urinary incontinence (EU) |
| Abuse potential | Yes (Schedule V in some states) | Higher than gabapentin (Schedule V) | No scheduled substance |
| Discontinuation syndrome | Mild | Mild | Yes - taper gradually to avoid discontinuation syndrome |
| Special warnings | Suicidal ideation (all anticonvulsants); respiratory depression with opioids/CNS depressants | Same as gabapentin; neuropsychiatric effects (mood, agitation) | Avoid in alcohol users (hepatotoxic); may raise blood sugar/HbA1c; avoid in narrow-angle glaucoma; BP elevation |
- Bradley and Daroff's Neurology, p. 2462-2464
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 3041-3043
- Goldman-Cecil Medicine, p. 2088
Key Clinical Pearls
-
Gabapentinoids vs. antidepressants: Gabapentin and pregabalin may be better than antidepressants for lancinating-type (shooting, electric) neuropathic pain. Antidepressants (TCAs, SNRIs) have proven benefit across a broader range of pain conditions. They also act additively when combined.
-
Pregabalin > gabapentin in efficacy: Pregabalin's linear pharmacokinetics make it more predictable and it shows slightly better NNT figures. However, gabapentin is preferred in elderly and medically complex patients because it has fewer DDIs and is less expensive.
-
Duloxetine is the drug of choice when neuropathic pain co-occurs with depression or anxiety - it treats both simultaneously. It is also first-line for diabetic peripheral neuropathy per IASP NeuPSIG and European Federation of Neurological Sciences guidelines.
-
Combination therapy is often more effective: Opioids + gabapentin or opioids + nortriptyline show synergistic benefit over monotherapy (Harrison's Principles, 22E, p. 3130).
-
All three require a 3-4 week trial to assess efficacy, as NNT ranges from 3-7 for all neuropathic pain drugs.
This is a shared conversation. Sign in to Orris to start your own chat.