Explain me about the right kidney, it’s topography and organs present posteriorly, anteriorly and muscle involved
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the information needed for a thorough answer. Let me also fetch the retroperitoneal position diagram for completeness.
Here is a complete, well-structured explanation of the right kidney - its topography, and all anterior, posterior, and muscle relations.
The Right Kidney - Topography and Relations
1. General Position and Topography
The right kidney is a retroperitoneal organ situated in the posterior abdominal region, immediately lateral to the vertebral column. Key topographic points:
- Vertebral levels: Extends from approximately vertebra T12 superiorly to L3 inferiorly (slightly lower than the left kidney due to the overlying liver)
- Why lower than left: The liver pushes the right kidney a few centimeters inferiorly compared to the left
- Axis: The longitudinal axis parallels the lateral edge of the psoas major muscle, angled about 30 degrees from vertical, with lower poles more lateral than upper poles
- Tilt: Also tilted ~30 degrees off the frontal plane, with lower poles anterior to upper poles
- Rotation: Each kidney is rotated ~30 degrees posteriorly from the renal hilum, making the lateral aspect posterior to the medial aspect - this places upper pole calyces more medial and superficial (dorsal) relative to lower pole calyces
- Rib relations: The superior pole of the right kidney lies anterior to rib XII (the left kidney lies anterior to ribs XI and XII)
- Coverings: Enclosed in perinephric fat (perirenal fat) immediately outside the renal capsule, which in turn is enclosed in the renal fascia (Gerota's fascia)
2. Anterior Relations
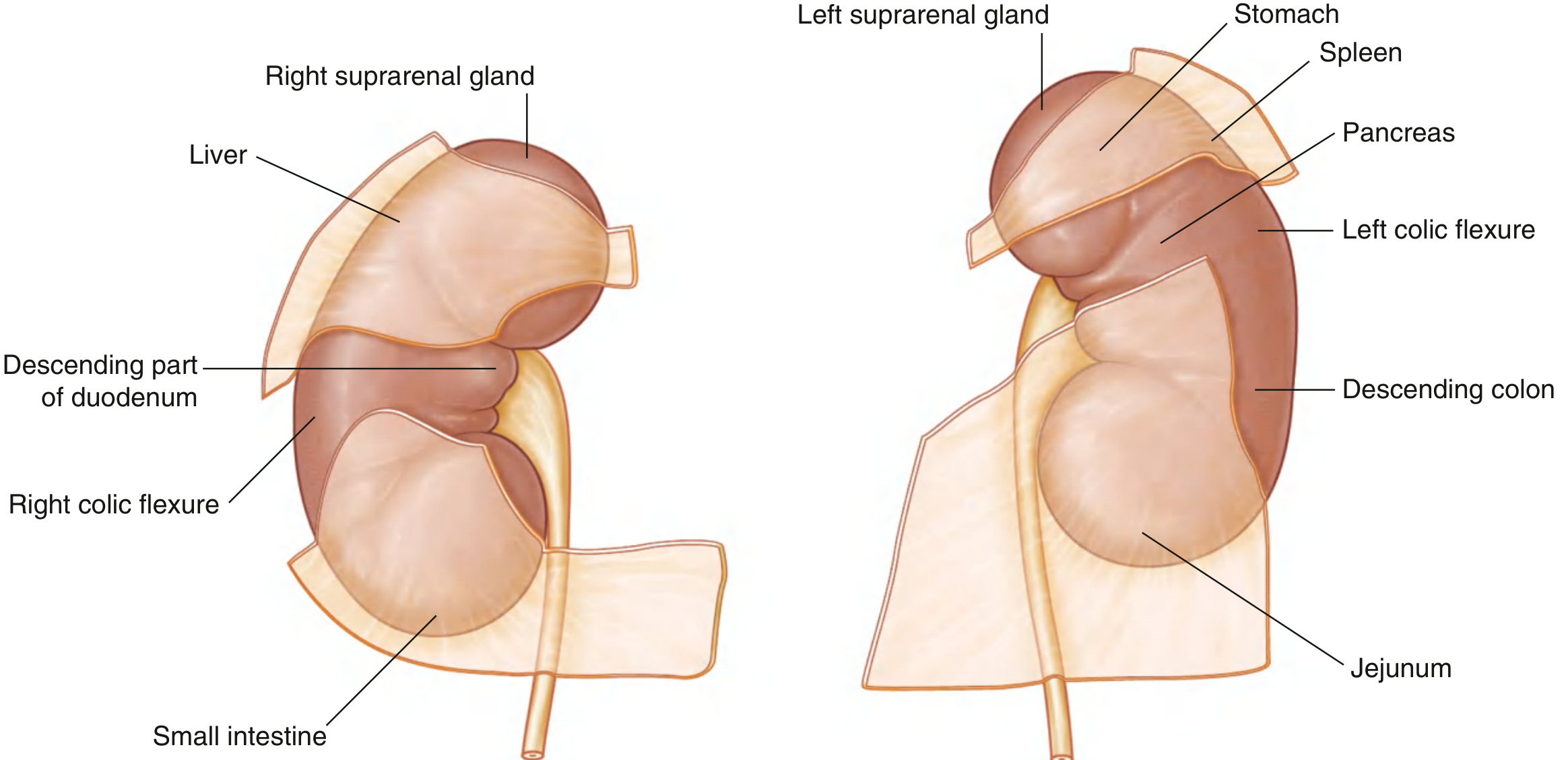
Fig. 4.153 - Structures Related to the Anterior Surface of Each Kidney (Gray's Anatomy for Students)
From superior to inferior, the anterior surface of the right kidney is related to:
| Structure | Contact Type | Location on Kidney |
|---|---|---|
| Right suprarenal (adrenal) gland | Direct contact | Small area, superior pole (medial side) |
| Liver | Separated by peritoneum (hepatorenal recess) | Large area, upper anterior surface |
| Descending (2nd) part of duodenum | Direct contact (retroperitoneal) | Medial aspect, middle of kidney |
| Right colic flexure (hepatic flexure) | Direct contact | Inferior pole, lateral side |
| Small intestine (jejunum/loops) | Separated by peritoneum | Inferior pole, medial side |
Key point: The duodenum and liver do NOT have peritoneum interposed - they contact the right kidney directly. The liver is separated by a layer of peritoneum (hepatorenal pouch of Morison). The right colic flexure contacts the lower lateral pole directly.
3. Posterior Relations
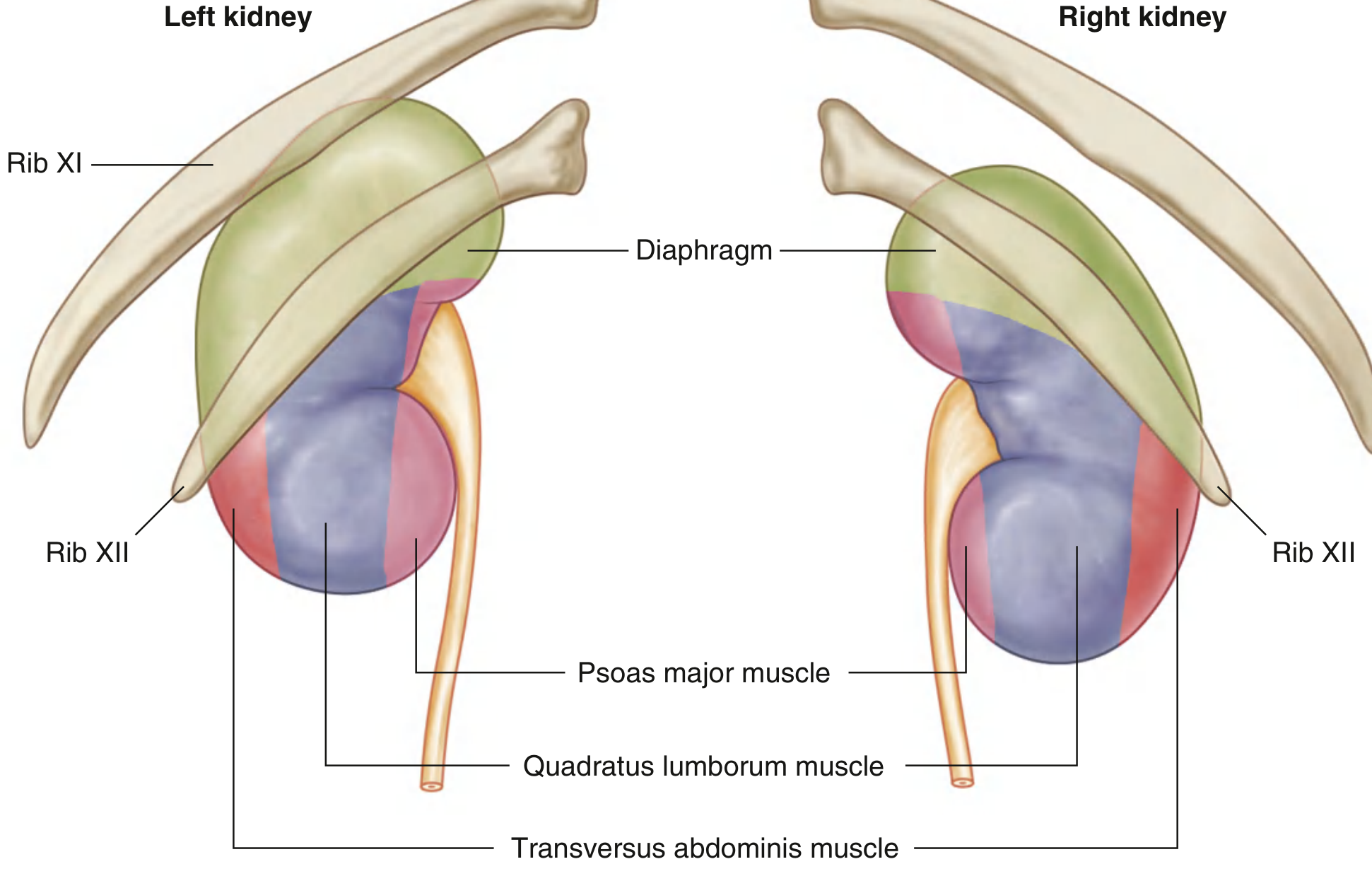
Fig. 4.154 - Structures Related to the Posterior Surface of Each Kidney (Gray's Anatomy for Students)
The posterior relations are more consistent between right and left kidneys. From medial to lateral, and from superior to inferior:
Muscles Posterior to the Right Kidney
| Muscle | Position/Relation |
|---|---|
| Diaphragm | Posterior to the upper pole (superior third) |
| Psoas major | Posterior and medial, covering the medial part of the kidney |
| Quadratus lumborum | Posterior, covering the middle-lateral part of the kidney |
| Transversus abdominis | Posterior to the lateral border / lower pole area |
Other Posterior Structures
- Rib XII - crosses posterior to the upper portion of the right kidney
- Pleura (costodiaphragmatic recess) - extends posterior to the kidney; risk of pleural injury during upper pole access
- Subcostal nerve and vessels (T12)
- Iliohypogastric nerve (L1)
- Ilioinguinal nerve (L1)
Clinical relevance: Because the lung lies above the 11th rib, direct lung injury is possible only if the 10th intercostal space is used for percutaneous access. The pleura is at risk during any upper pole puncture.
4. Summary Table
| Surface | Structure | Notes |
|---|---|---|
| Anterior - upper | Right suprarenal gland | Direct contact, small area |
| Anterior - upper | Liver | Via peritoneum (hepatorenal pouch) |
| Anterior - medial | 2nd part of duodenum | Direct contact, retroperitoneal |
| Anterior - lower lateral | Right colic flexure | Direct contact |
| Anterior - lower medial | Small intestine | Via peritoneum |
| Posterior - superior | Diaphragm | Upper pole |
| Posterior - medial | Psoas major | Most medial posterior contact |
| Posterior - middle | Quadratus lumborum | Central posterior contact |
| Posterior - lateral | Transversus abdominis | Lateral/lower posterior |
| Posterior - nerves | Subcostal, iliohypogastric, ilioinguinal | Pass behind kidney |
5. Clinical Relevance of These Relations
- Renal colic vs duodenal pathology: Because the duodenum directly contacts the right kidney, inflammation of either can mimic the other
- Percutaneous nephrolithotomy (PCNL): Posterior access must avoid the pleura (upper pole) and the colon (which can be retrorenal, especially on the right in ~9% of patients at the lower pole level)
- Surgical access: The liver can cover the entire anterior surface in some individuals, making anterior surgical approaches more complex on the right
- Psoas sign: An inflamed kidney (pyelonephritis, perinephric abscess) can irritate the psoas muscle, causing pain on hip extension
Sources:
- Gray's Anatomy for Students, pp. 436-439 (Figs. 4.153, 4.154)
- Campbell Walsh Wein Urology, Perirenal Anatomy, pp. 206-207
This is a shared conversation. Sign in to Orris to start your own chat.