A 5 0 year old male slept overnight on the armchair with arm hanging on side. Next day he consulted orthopedic with the chief complaint of wrist being dropped-in flex position and unable to do active extension o f his wrist. Answer the following questions on basis of above clinical case- a) Name the nerve likely to be involved in this case. (1 mark) b) Describe beginning, course, relations, branches and applied anatomy off related nerve. ( 6 marks) c) Boundaries and contents of lower triangular space around scapula (2 marks) d) Which structures are supplied by this nerve in hand?!
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a complete, detailed answer. Here it is:
Clinical Case: Wrist Drop after Sleeping in Armchair
a) Nerve Involved
The Radial Nerve (C5, C6, C7, C8, T1) - arising from the posterior cord of the brachial plexus.
This is a classic case of "Saturday Night Palsy" (also called "Honeymooner's palsy") - compression of the radial nerve in the radial groove of the humerus from prolonged pressure of the arm hanging over the edge of a chair while asleep. The result is wrist drop with inability to actively extend the wrist.
b) Radial Nerve - Beginning, Course, Relations, Branches & Applied Anatomy
Origin / Beginning
The radial nerve arises from the posterior cord of the brachial plexus (C5-T1) in the axilla. It is the largest branch of the brachial plexus.
Course
The radial nerve follows a distinct path through three regions:
1. In the Axilla:
- Lies posterior to the axillary artery, between it and the subscapularis, teres major, and latissimus dorsi muscles.
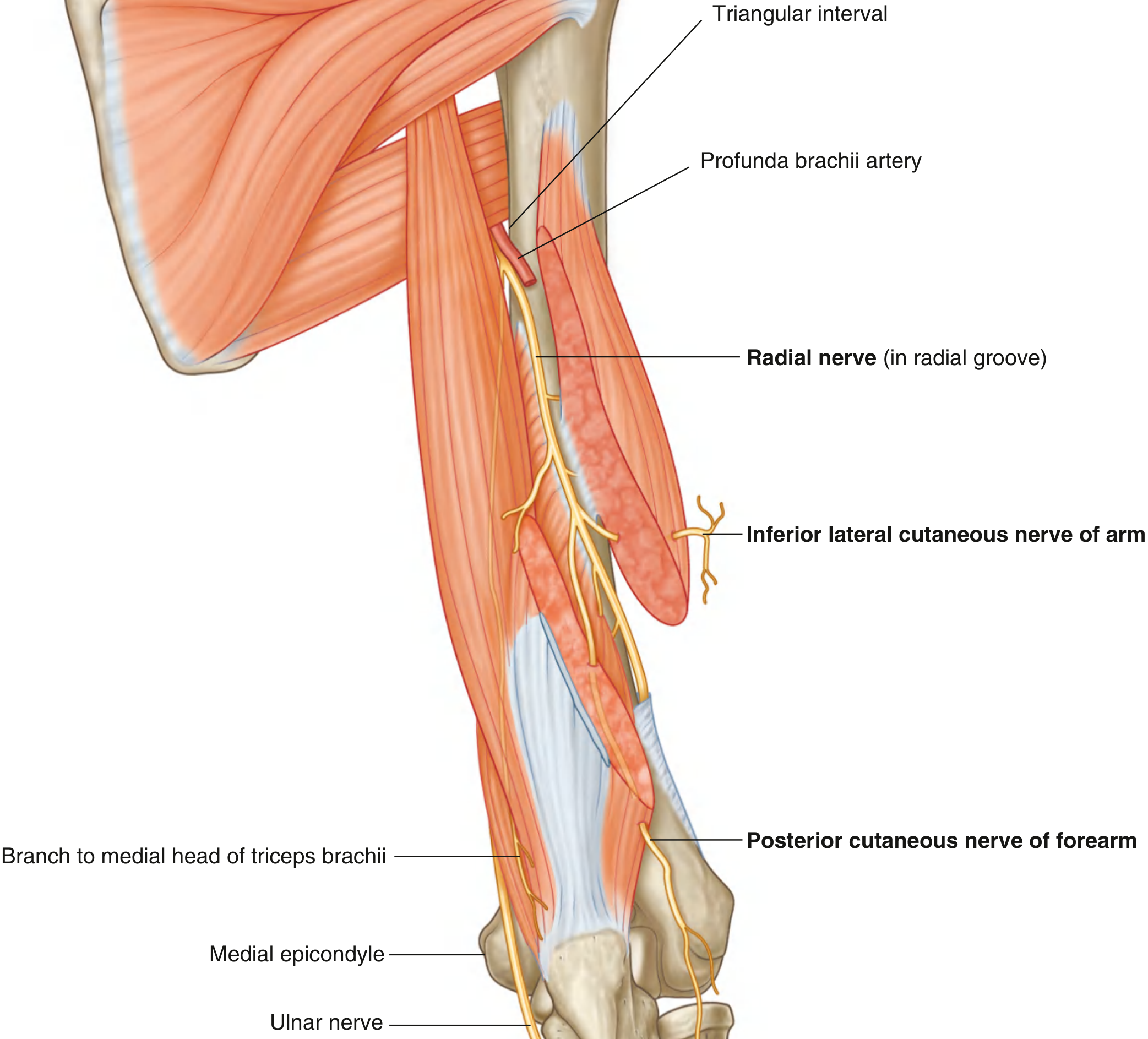
- Exits the axilla by passing through the triangular interval (lower triangular space), accompanied by the profunda brachii artery.
2. In the Arm (Posterior Compartment):
- Enters the posterior compartment of the arm through the triangular interval.
- Accompanied by the profunda brachii artery, it passes diagonally from medial to lateral through the posterior compartment, lying in the radial groove directly on bone (between the medial and lateral heads of triceps brachii).
- On the lateral side of the arm, it pierces the lateral intermuscular septum and enters the anterior compartment.
- It then lies between the brachialis and brachioradialis muscles, entering the forearm anterior to the lateral epicondyle, just deep to brachioradialis.
3. In the Forearm (Cubital Fossa and Beyond):
- At the lateral border of the cubital fossa, deep to brachioradialis, the radial nerve bifurcates into superficial and deep branches.
- Deep branch: Predominantly motor; passes between the superficial and deep layers of the supinator muscle. It supplies supinator, then emerges as the posterior interosseous nerve, running between the superficial and deep muscle layers of the posterior compartment of the forearm to supply all remaining extensors. Terminates as articular branches to the wrist.
- Superficial branch: Purely sensory; runs down the anterolateral forearm deep to brachioradialis, in association with the radial artery. About two-thirds down, it winds posteriorly around the radial side of the forearm to reach the hand (dorsolateral surface).
Relations (Key)
- In the radial groove: lies directly on bone, between medial and lateral heads of triceps brachii, with the profunda brachii artery.
- In the cubital fossa: between brachioradialis (lateral) and brachialis (medial).
Branches
| Region | Branch | Type |
|---|---|---|
| Axilla | Posterior cutaneous nerve of the arm | Cutaneous |
| Posterior arm | Inferior lateral cutaneous nerve of the arm | Cutaneous |
| Posterior arm | Posterior cutaneous nerve of the forearm | Cutaneous |
| Arm | Muscular branches to triceps brachii (all 3 heads), anconeus, brachioradialis, extensor carpi radialis longus, lateral part of brachialis | Motor |
| Cubital fossa | Articular branches to elbow joint | Articular |
| Forearm | Deep branch → posterior interosseous nerve (motor) | Motor |
| Forearm | Superficial branch (sensory to dorsolateral hand) | Sensory |
Applied Anatomy
-
Saturday Night Palsy / Radial Groove Injury (this case): Compression of the radial nerve in the radial groove (arm hanging over armchair overnight) causes wrist drop due to paralysis of posterior compartment extensors. Triceps and sensation over the posterior arm are spared (those branches arise proximal to the groove). Sensation over the posterior aspect of the hand is reduced. Recovery is usually spontaneous (neuropraxia).
-
Axillary injury: Crutch palsy or fracture-dislocation of proximal humerus - all radial nerve muscles paralyzed including triceps (full loss).
-
Posterior interosseous nerve injury: Fracture or dislocation of radial head - finger drop without wrist drop, no sensory loss.
-
Midshaft humerus fracture: The nerve is tightly bound in the radial groove and may be stretched or transected - wrist drop with sensory loss over dorsum of hand. The nerve must always be tested when midshaft humeral fracture is suspected.
As noted in [S. Das Manual on Clinical Surgery](p. 6854): "Pressure on the arm at the edge of a chair after deep sleep being drunk - Saturday night palsy" - the exact mechanism in this case.
c) Boundaries and Contents of the Lower Triangular Space (Triangular Interval)
Note: The question says "lower triangular space around scapula" - this refers to the Triangular Interval (not the triangular space), which is the space through which the radial nerve travels. The triangular space is a separate entity dealt with below. Both are described.
Triangular Space (Upper)
Boundaries:
- Medial: Medial margin of the long head of triceps brachii
- Superior: Inferior margin of teres minor
- Inferior: Superior margin of teres major
Contents: Circumflex scapular artery and vein
Triangular Interval (Lower Triangular Space) - the clinically relevant one here
Boundaries:
- Medial: Lateral margin of the long head of triceps brachii
- Lateral: Shaft of the humerus
- Superior: Inferior margin of teres major
Contents:
- Radial nerve
- Profunda brachii artery (deep artery of arm)
- Accompanying veins (venae comitantes)
This interval serves as the passageway between the axilla and the posterior compartment of the arm, through which the radial nerve exits the axilla. - Gray's Anatomy for Students
d) Structures Supplied by the Radial Nerve in the Hand
The radial nerve has no motor supply to intrinsic muscles of the hand - all intrinsic hand muscles are supplied by median and ulnar nerves.
Sensory Supply in the Hand:
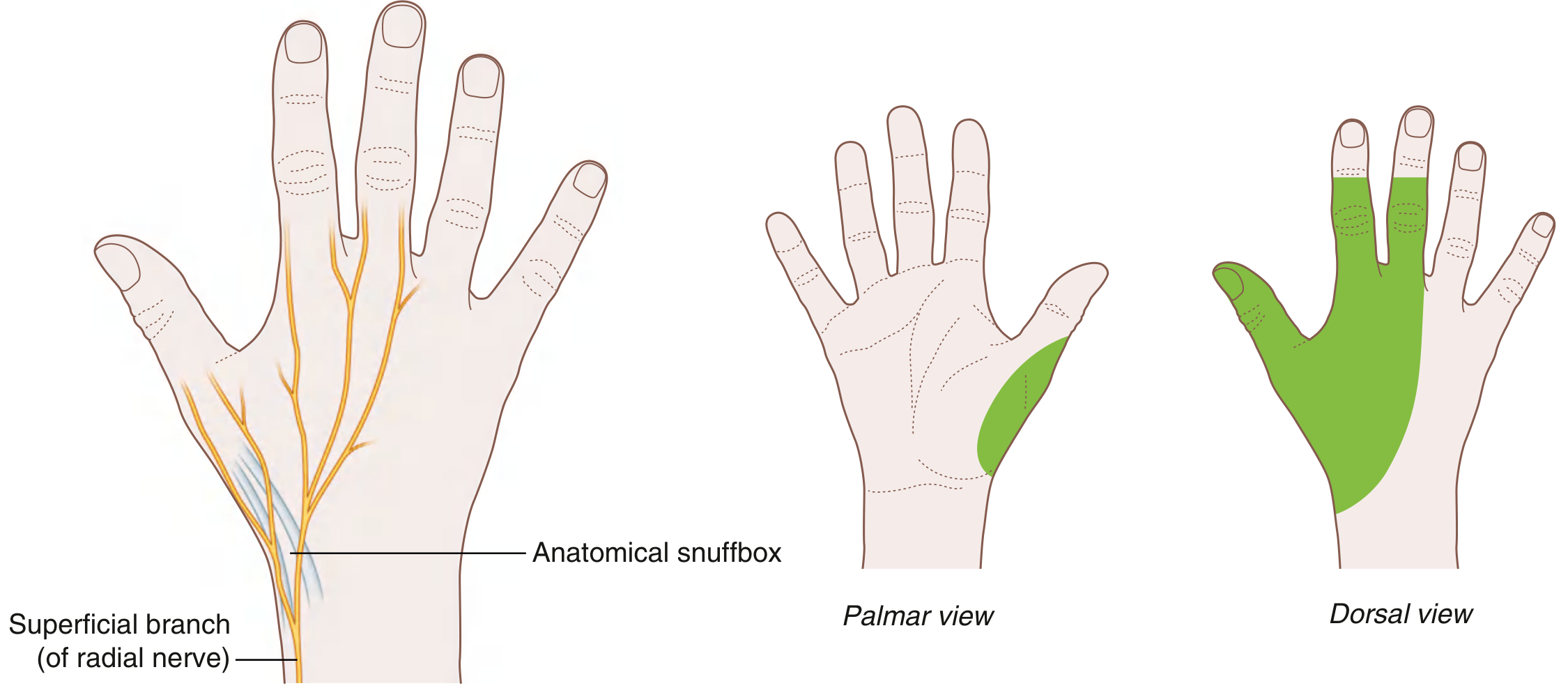
- The superficial branch of the radial nerve provides cutaneous innervation to:
- The posterolateral (dorsolateral) surface of the hand
- The lateral aspect of the dorsum of metacarpal I (thumb metacarpal)
- The dorsum of the first web space (the most consistent autonomous zone)
- Skin over the posterior surfaces of the lateral 3½ digits (thumb, index, middle, and lateral half of ring finger) - though only the proximal phalanges, as the distal phalanges are supplied by the median nerve
Motor (Extrinsic) Supply via Radial Nerve to Hand Function:
The radial nerve produces:
- Extension of the wrist (via extensor carpi radialis longus, brevis, and extensor carpi ulnaris)
- Extension of metacarpophalangeal joints of all fingers (via extensor digitorum)
- Extension and abduction of the thumb (via extensor pollicis longus, extensor pollicis brevis, and abductor pollicis longus)
Important distinction: Extension of the interphalangeal joints is carried out by the interossei (supplied by the ulnar nerve) through the extensor expansions - these are NOT affected in radial nerve palsy. This can be mistakenly interpreted as signs of nerve recovery if this anatomical point is not recognized. - S. Das Manual on Clinical Surgery, p. 6872
In this case, since the injury is at the radial groove level, the triceps and sensation over the posterior arm are spared, but the patient loses wrist extension (wrist drop), finger extension at MCP joints, and has reduced sensation over the dorsum of the hand.
Sources: Gray's Anatomy for Students (9780323934237); S. Das Manual on Clinical Surgery 13th Ed; Schwartz's Principles of Surgery 11th Ed; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.