Mri brachial plexus radiology 1. Normal anatomy 2. relevant pathology and it's imaging findings 3.normal mri appearance included images
Reading File
Finding Sources
Searching the Web
MRI brachial plexus normal anatomy imaging findings radiology
Reading File
Reading File
Finding Sources
Reading Web Page
https://appliedradiology.com/articles/mri-of-the-brachial-pl…
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have rich content and images to write a comprehensive answer. Let me compile the full response.
MRI of the Brachial Plexus: Comprehensive Radiology Review
1. Normal Anatomy
Overview
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5, C6, C7, C8, and most of T1. It originates in the neck, passes laterally and inferiorly over the first rib, and enters the axilla. Its organization follows the mnemonic: Roots - Trunks - Divisions - Cords - Branches (Randy Travis Drinks Cold Beer).

| Component | Details |
|---|---|
| Roots | Anterior rami C5-T1; pass between anterior and middle scalene muscles |
| Trunks | Superior (C5+C6), Middle (C7), Inferior (C8+T1); pass over rib I into the axilla |
| Divisions | Each trunk splits into anterior + posterior divisions (6 total) at the clavicular level |
| Cords | Lateral (anterior divisions of superior + middle), Medial (anterior division of inferior), Posterior (all three posterior divisions); named by relationship to the axillary artery |
| Terminal branches | Musculocutaneous, median, ulnar, radial, and axillary nerves |
Key spatial relationships:
- Roots and trunks lie in the posterior triangle of the neck, posterior to the subclavian artery, between anterior and middle scalene muscles (interscalene space)
- At the level of the clavicle - the costoclavicular space
- Infraclavicular - the retropectoralis minor space (beneath the pectoralis minor muscle)
- Cords surround the axillary artery in the axilla
MRI Protocol
The normal medial-to-superior orientation of the plexus makes standard axial/coronal/sagittal sequences difficult to interpret, because the nerve course runs obliquely. Standard protocol includes:
- Oblique coronal T2 fat-suppressed - best plane for overall plexus visualization; allows bilateral comparison
- Oblique sagittal T2 - best for evaluating individual nerve segments and foraminal exit zones
- Axial T1 / T2 - good for relationship to vascular structures
- 3D T2/STIR (heavy T2 myelographic sequences) - critical for nerve root visualization and detecting meningoceles
- T1 post-gadolinium fat-sat - for detecting neoplastic infiltration and enhancement
- Field strength: 3T preferred (better SNR), though 1.5T is adequate
Normal MRI Signal Characteristics
On standard MRI, normal brachial plexus nerves appear as:
- T1-weighted: intermediate signal, similar to muscle; individual roots appear as small oval/round structures within the neural foramina surrounded by epidural fat (which gives bright T1 signal, providing natural contrast)
- T2-weighted: mildly hyperintense compared to muscle; slightly brighter due to the endoneurial fluid content - but LESS bright than surrounding fat or CSF
- STIR / fat-suppressed T2: nerves are intermediate-to-slightly hyperintense; fat suppression removes background fat signal and makes nerves easier to delineate
The critical principle: normal nerves should NOT show bright T2 signal - significant T2 hyperintensity indicates edema or pathology.
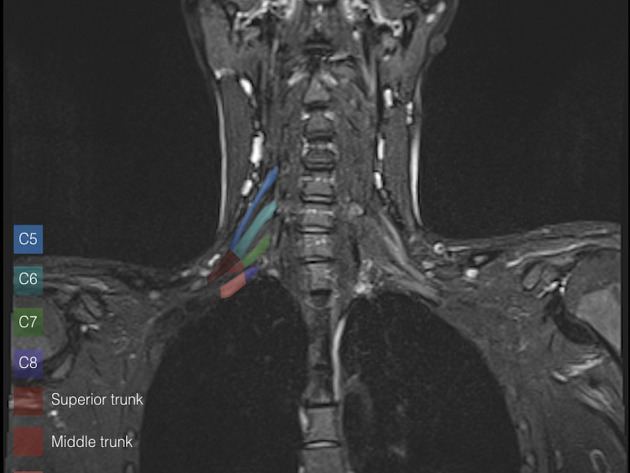

Normal Appearance - Segment by Segment
| Segment | MRI Landmark | Appearance |
|---|---|---|
| Nerve roots (preganglionic) | Within neural foramina | Oval low-signal structures surrounded by bright epidural fat on T1 |
| Dorsal root ganglion | Neural foramen | Slightly enlarged rounded structure, may show faint T2 brightness |
| Postganglionic roots | Interscalene triangle | Thin linear structures between anterior and middle scalene muscles |
| Trunks | Between scalene muscles and clavicle | Round/oval structures, isointense to slightly hyperintense on T2-STIR |
| Divisions | At the clavicle | Flat, ribbon-like structures; divided into anterior and posterior |
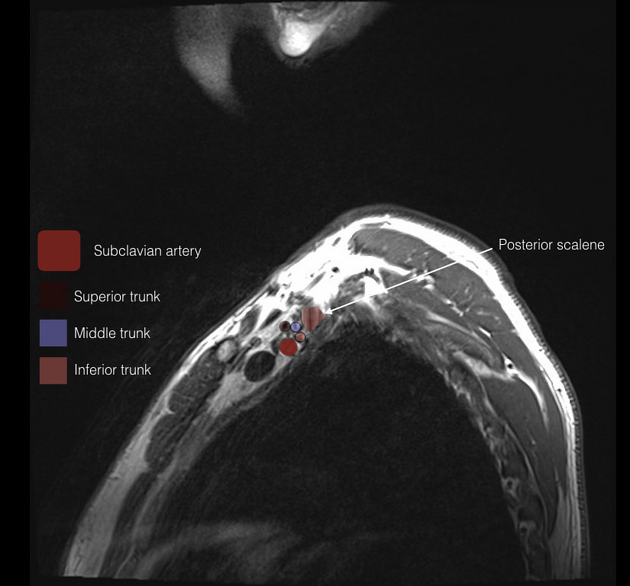
| Cords | Infraclavicular, around axillary artery | Bundle surrounding the axillary artery; named by position relative to it |
2. Relevant Pathology and Imaging Findings
A. Traumatic Brachial Plexus Injury
Traumatic injury is the most common indication for brachial plexus MRI, typically from high-velocity traction (motorcycle accidents, birth trauma). Injuries are classified as preganglionic (proximal to dorsal root ganglion, not repairable by nerve grafting) vs postganglionic (distal, potentially repairable).
75% of clinical brachial plexus injuries involve root avulsion from the cord; 25% are confined to the distal plexus - Grainger & Allison's Diagnostic Radiology
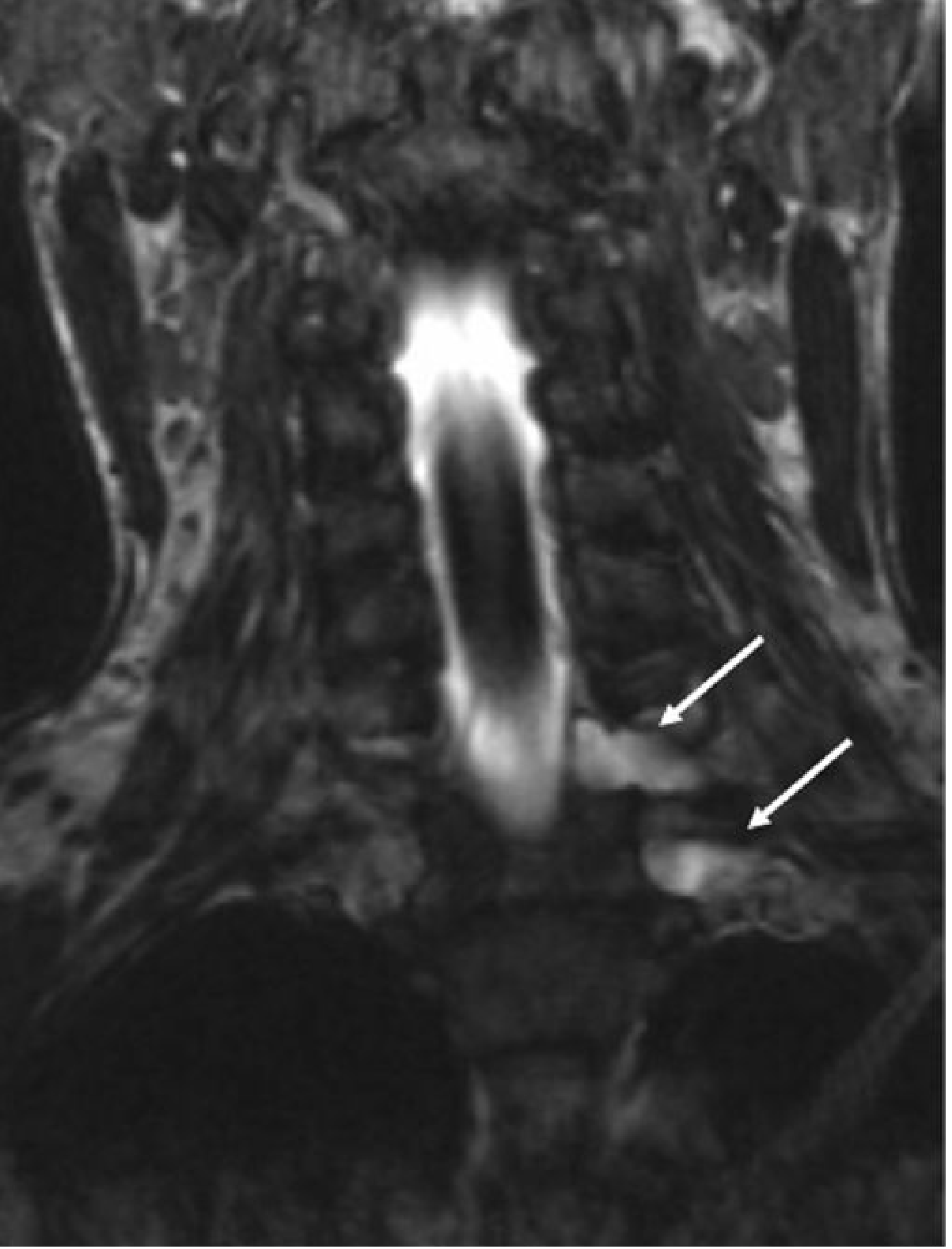
Preganglionic (Root Avulsion) - MRI Findings:
- Traumatic pseudomeningocele - CSF-filled outpouching extending through the torn dural sleeve into the paraspinal region; appears as a bright T2 / dark T1 fluid collection extending from the foramen (PATHOGNOMONIC of avulsion)
- Absent intradural nerve root - the normal linear filling defect within the hyperintense CSF is absent on myelographic T2 sequences
- Cord edema - diffuse T2 hyperintensity of the spinal cord; must not be confused with direct cord injury
- Denervation changes in paraspinal muscles - multifidus and semispinalis capitis atrophy (these receive dorsal ramus branches from the avulsed roots)

Postganglionic Injury - MRI Findings:
- Nerve enlargement with T2 hyperintensity (edema/neuritis)
- Disruption or discontinuity of nerve fibers on high-resolution sequences
- Intact nerve roots visible on myelographic sequences (distinguishes from preganglionic)
- Surrounding hematoma / edema in surrounding soft tissues
- Late changes: fatty replacement and atrophy of denervated muscles
B. Neoplastic Plexopathy
Metastatic / Tumor Infiltration
Common primary tumors: breast, lung (especially Pancoast), lymphoma, sarcoma.
MRI findings:
- A mass lesion adjacent to or engulfing brachial plexus elements
- T2 hyperintensity and nerve enlargement in involved segments
- Avid contrast enhancement - mass-like or infiltrative pattern
- May show epidural extension (very important surgical consideration)
- MRI sensitivity for detecting tumor infiltration: 96%, specificity 95% - Bradley and Daroff's Neurology in Clinical Practice
- Typically involves the lower plexus (C8-T1) for Pancoast tumors (weakness of intrinsic hand muscles, 4th and 5th digit paresthesias, Horner syndrome)
Pancoast tumor (superior sulcus tumor): apical lung mass on chest radiograph; MRI demonstrates invasion of lower plexus roots, first rib, vertebral body, and subclavian vessels.
C. Radiation-Induced Plexopathy
Occurs as a delayed complication (3 months to 26 years; mean ~6 years) following radiotherapy, most often for breast cancer or lung cancer.
Mechanism: ischemic insult to vasa nervorum causing endoneural/perineural fibrosis + direct myelin/axon damage.
MRI findings:
- Diffuse thickening of plexus elements within the radiation field
- T2 signal increase - moderate, diffuse rather than focal
- No discrete mass (helps distinguish from metastatic plexopathy)
- Fibrosis may produce low T2 signal in chronic cases
- On Gadolinium: may show enhancement in acute/subacute phase
- Surrounding muscles may show post-radiation fatty atrophy
Clinical pearl: if there is NO identifiable mass on MRI and appropriate history + clinical signs are present, MRI reliably distinguishes radiation plexopathy from metastatic recurrence. - Grainger & Allison's Diagnostic Radiology
D. Thoracic Outlet Syndrome (TOS)
Compression of the brachial plexus (neurogenic TOS) within one of three anatomic spaces: interscalene triangle, costoclavicular space, or subcoracoid (pectoralis minor) space.
Causes: cervical rib, fibrous band from short cervical rib to first rib (angulates the lower trunk), scalene anomalies, clavicular/first rib fracture malunion.
MRI findings:
- Dynamic MRI (provocative positions: arm abduction, external rotation) most useful
- Cervical rib or elongated C7 transverse process on coronal sequences
- Fibrous band stretching/angulating the inferior trunk
- Neural compression visible at the scalene triangle or costoclavicular space
- Associated subclavian/axillary vessel compression may be seen
Coronal image showing SA = subclavian artery and SV = subclavian vein in relation to plexus:

E. Inflammatory Plexopathy (Parsonage-Turner Syndrome / Neuralgic Amyotrophy)
Idiopathic or post-infectious/post-vaccination immune-mediated plexitis.
MRI findings:
- T2 hyperintensity and mild enlargement of affected nerves - often patchy, multifocal
- May involve the suprascapular nerve, long thoracic nerve, or multiple cord levels
- Denervation edema in affected muscles (T2 bright, T1 dark initially)
- Late: fatty atrophy of denervated muscles (T1 bright)
- Often normal early in the course - MRI changes may lag symptoms by several weeks
- Magnetic resonance neurography (MRN) is the most sensitive technique
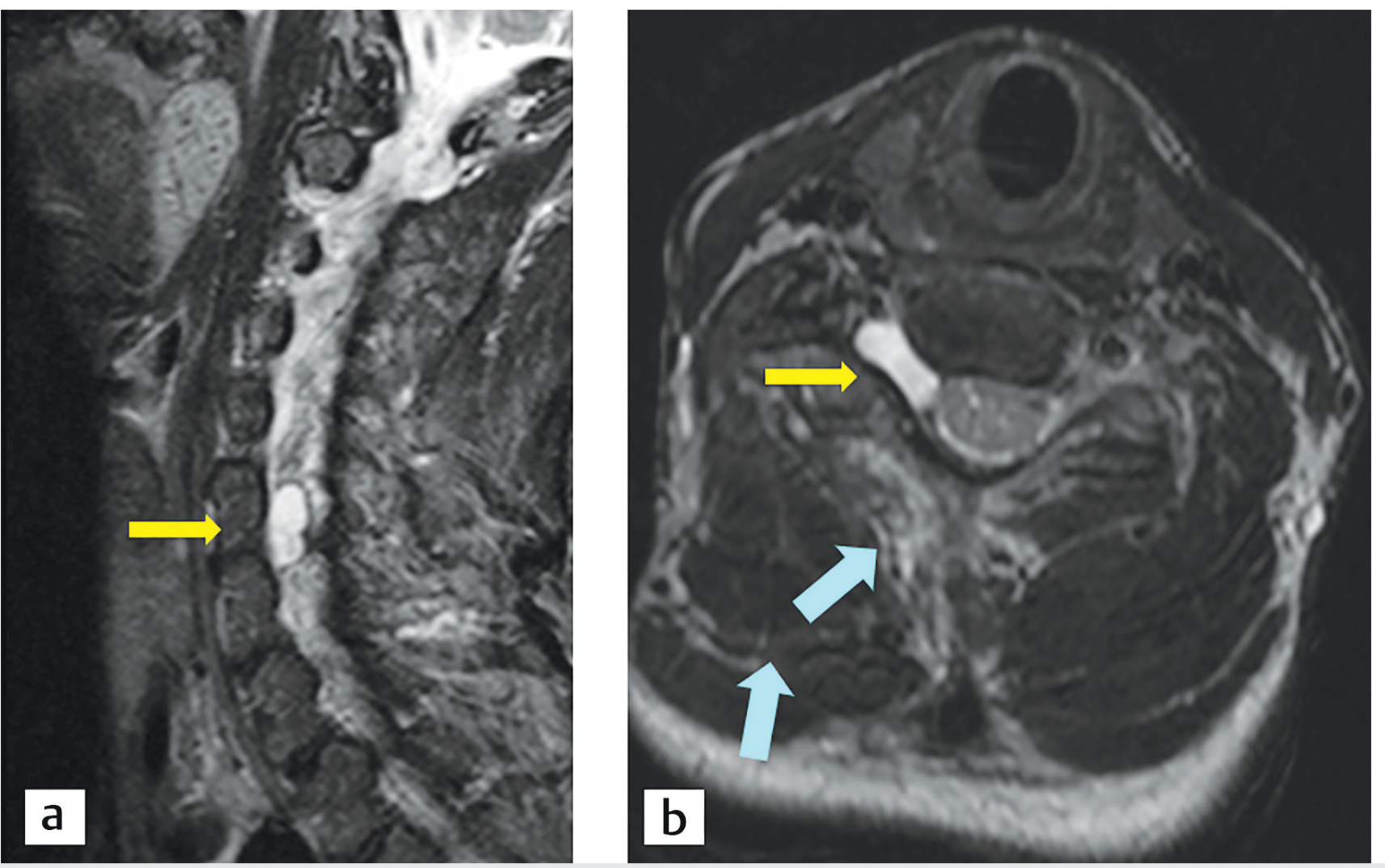
F. Peripheral Nerve Sheath Tumors
Schwannoma and neurofibroma are the most common benign peripheral nerve tumors. Neurofibromas are strongly associated with NF1.
MRI findings:
- Fusiform mass along the course of a nerve (spindle-shaped)
- T1: isointense to muscle
- T2: markedly hyperintense ("target sign" - central low T2 with peripheral high T2 - characteristic of neurofibroma)
- Gadolinium enhancement: avid, usually homogeneous for schwannoma; heterogeneous for large neurofibromas
- Malignant peripheral nerve sheath tumors (MPNST): irregular margins, rapid growth, heterogeneous enhancement, perineural spread, satellite nodules
Summary Table: Pathology at a Glance
| Pathology | Key MRI Features | Location |
|---|---|---|
| Root avulsion (preganglionic) | Pseudomeningocele, absent root, cord edema, paraspinal denervation | Foraminal / intradural |
| Postganglionic injury | Nerve T2 hyperintensity, enlargement, late atrophy | Interscalene to infraclavicular |
| Metastatic plexopathy | Mass + nerve enhancement, ± epidural extension | Often lower plexus (C8-T1) |
| Radiation plexopathy | Diffuse thickening, no mass, T2 increase in field | Within radiation field |
| TOS | Dynamic compression, cervical rib/fibrous band | Interscalene / costoclavicular |
| Parsonage-Turner | Patchy T2 hyperintensity, muscle denervation | Variable, often upper plexus |
| Schwannoma | Fusiform nerve mass, avid T2 signal, enhancement | Along any segment |
| Neurofibroma | Target sign on T2, fusiform, associated NF1 | Along any segment |
3. Normal MRI Appearance - Summary
On T1:
- Roots surrounded by bright epidural fat within foramina (natural contrast)
- Trunks and cords: round/oval structures, isointense to muscle
- Scalene muscles provide easily recognizable landmarks
On T2/STIR fat-suppressed:
- Nerves are mildly hyperintense relative to muscle
- Clearly distinguishable from surrounding fat (which is suppressed)
- Normal nerves should be smooth, symmetrical in caliber, and without focal T2 bright signal
Key structures to assess on every brachial plexus MRI:
- Nerve root exit foramina (C5-T1) - patent, no compression
- Interscalene triangle - scalene muscles normal, no fibrous bands
- Costoclavicular space - no cervical rib or clavicular deformity
- Pectoralis minor space - normal
- Axillary artery and subclavian vessels - no vascular compression
- Paravertebral/paraspinal muscles - symmetric, no denervation changes
- Lung apex - exclude Pancoast tumor
- Cervical spine - disc herniations, osteophytes, cord changes
Sources:
- Grainger & Allison's Diagnostic Radiology, Block 10 & 12 (Brachial Plexus Injury; Radiation Plexopathy)
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Block 2 (Ventral Rami, Upper Trunk, Divisions)
- Gray's Anatomy for Students, Block 4-5 (Brachial Plexus)
- Bradley and Daroff's Neurology in Clinical Practice, Block 27 & 6 (Plexopathies, Cancer)
- Vijayasarathi A, Chokshi FH. "MRI of the brachial plexus: A practical review." Applied Radiology, 2016.
This is a shared conversation. Sign in to Orris to start your own chat.