Vit A
Reading File
Finding Sources
Searching PubMed
"vitamin A" AND deficiency
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is the full breakdown:
Vitamin A (Retinol)
Overview
Vitamin A is a fat-soluble vitamin that exists in several interconvertible forms:
- Retinol - transport and storage form
- Retinal - active form in the visual cycle
- Retinoic acid - active form for gene regulation and cell differentiation
- Retinyl ester - storage form (liver, peripheral tissues)
- Beta-carotene - plant-derived provitamin (contributes ~30% of dietary vitamin A)
Dietary Sources
| Source Type | Examples |
|---|---|
| Animal (preformed, retinyl ester) | Liver, fish, eggs, milk, butter |
| Plant (provitamin, beta-carotene) | Carrots, squash, spinach, yellow/leafy green vegetables |
The RDA is expressed in retinol equivalents (RE), which accounts for contributions from both preformed vitamin A and beta-carotene. Conversion: 10,000 IU = 3,000 mcg vitamin A.
Metabolism
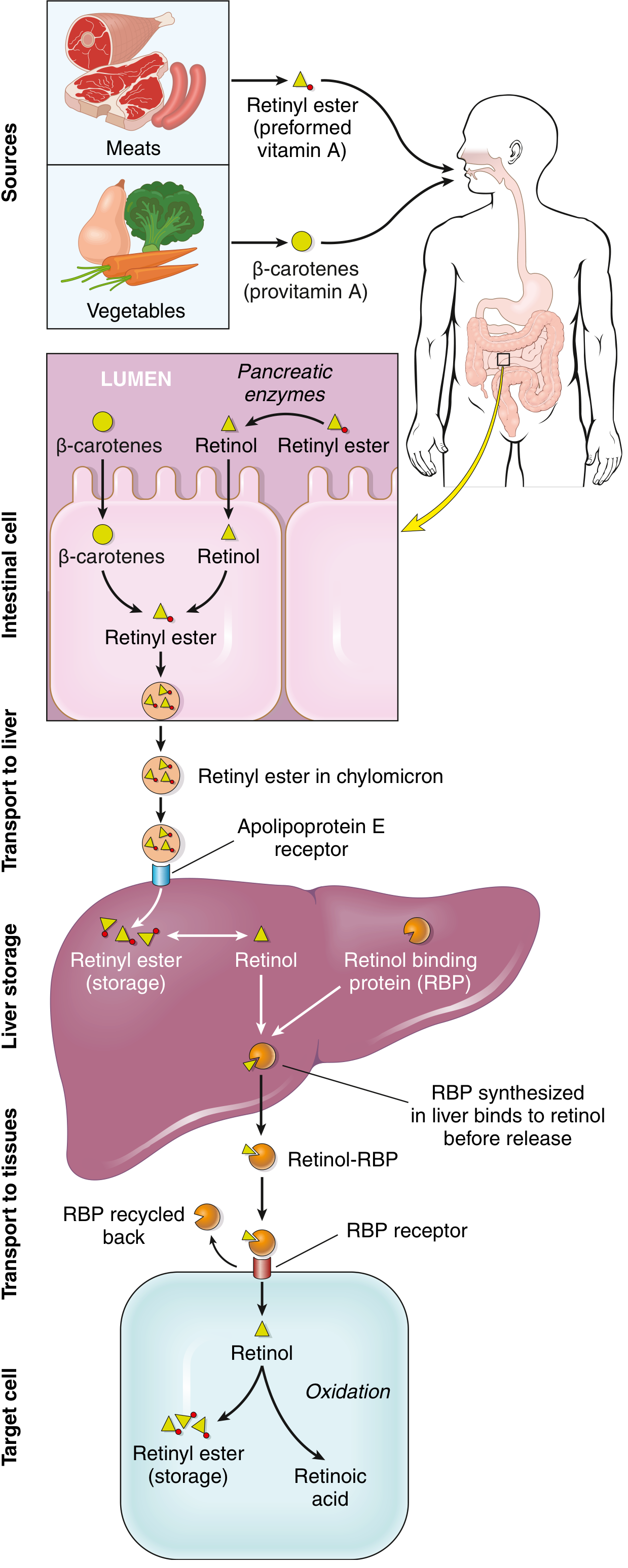
Key steps (from Robbins & Kumar Basic Pathology):
- Absorption - Requires bile, pancreatic enzymes, and dietary fat. Retinyl esters are cleaved to retinol by pancreatic enzymes; beta-carotene is converted to retinol in intestinal cells.
- Transport to liver - Retinol is packaged as retinyl ester in chylomicrons and taken up by the liver via the apolipoprotein E receptor.
- Storage - >90% of body's vitamin A is stored in the liver as retinyl ester in perisinusoidal stellate (Ito) cells. Reserves last at least 6 months on adequate diet.
- Release - Retinol binds retinol-binding protein (RBP) (synthesized in liver) for circulation. RBP is recycled after retinol delivery to peripheral cells.
- In target cells - Retinol is either stored as retinyl ester or oxidized to retinoic acid.
Functions
1. Vision
Vitamin A is a component of four visual pigments:
- Rhodopsin (rod cells) - for low-light/dim-light vision
- Three iodopsins (cone cells) - for color vision in bright light
Deficiency reduces synthesis of all four, causing night blindness as the earliest sign.
2. Epithelial Differentiation
Retinoic acid binds retinoic acid receptors (RARs), which heterodimerize with retinoid X receptors (RXRs). The RAR/RXR complex binds retinoic acid response elements (RAREs) on DNA, regulating genes for growth factor receptors, tumor suppressors, and secretory proteins. This governs the orderly differentiation of mucus-secreting columnar epithelium. Without vitamin A, epithelium undergoes squamous metaplasia and keratinization.
3. Metabolic Effects
Retinoids inhibit adipogenesis and stimulate lipid breakdown. RXR forms heterodimers with PPARs and vitamin D receptors, linking vitamin A to lipid and calcium metabolism.
4. Immune Function & Anti-infective
Vitamin A supplementation reduces diarrhea morbidity by ~15% and mortality by ~30%. It promotes regeneration of damaged epithelia and supports immune cell function. In populations where deficiency is prevalent, supplementation reduces overall child mortality by 20-30%.
Deficiency
Causes
- Poor nutrition (most common globally, especially in developing countries)
- Fat malabsorption: celiac disease, Crohn disease, colitis, biliary atresia, cystic fibrosis
- Bariatric surgery
- Continuous use of mineral oil laxatives
- Infants on non-dairy formula lacking vitamin A
Clinical Features (in order of progression)
| Feature | Mechanism |
|---|---|
| Night blindness | Earliest sign; reduced rhodopsin synthesis |
| Xerosis conjunctivae | Keratinization of conjunctival epithelium (dry eye) |
| Bitot spots | White foamy plaques at corneal margin from keratin debris |
| Keratomalacia | Corneal ulceration, softening, and destruction - leads to blindness |
| Squamous metaplasia of airways | Predisposes to secondary pulmonary infections |
| Urinary tract keratinization | Renal/bladder stones from keratin debris |
| Follicular/papular dermatosis | Hyperkeratinization + plugging of adnexal ducts |
Collectively, the eye changes are called xerophthalmia.
Toxicity (Hypervitaminosis A)
Acute Toxicity
Symptoms: headache, dizziness, vomiting, stupor, blurred vision - can mimic a brain tumor (pseudotumor cerebri).
Historical note: first described in 1597 after crew members ate polar bear liver. Polar bear, whale, shark, and halibut liver are all dangerously high in vitamin A.
Chronic Toxicity
- Weight loss, anorexia, nausea, vomiting
- Bone and joint pain, hyperostoses
- Retinoic acid stimulates osteoclast activity → increased bone resorption → fracture risk
- Dry, pruritic skin
- Pseudotumor cerebri with papilledema
Chronic toxicity threshold: daily intake of >25,000 IU (though most cases involve much higher doses). Average reported toxic dose: ~100,000 IU/day over 7.2 years.
Hepatotoxicity (from Sleisenger & Fordtran's GI and Liver Disease)
Vitamin A is the most important hepatotoxin among vitamin supplements when taken in supratherapeutic doses. Key facts:
- Dose- and duration-dependent injury
- Liver half-life: 50 days to 1 year - fibrosis may progress even after stopping supplementation
- Mechanism: activation of hepatic stellate cells → hyperplasia/hypertrophy → sinusoidal compression → portal hypertension + collagen synthesis
- Biopsy: characteristic greenish autofluorescence under UV light; "Swiss cheese/honeycomb" appearance from enlarged stellate cells
- Histology: 59% cirrhosis, 34% chronic hepatitis, 21% microvesicular steatosis, 14% perisinusoidal fibrosis, 3% peliosis hepatitis
- Water-miscible/emulsified formulations are up to 10x more hepatotoxic than oil-based preparations
- Ethanol + beta-carotene combination is particularly hepatotoxic
Severe cases present with hepatomegaly, splenomegaly, ascites, variceal bleeding.
Therapeutic Use & Dosing (Harriet Lane Handbook)
| Indication | Dose |
|---|---|
| Measles supplementation (<6 mo) | 50,000 IU/day PO x 2 days |
| Measles supplementation (6 mo - <1 yr) | 100,000 IU/day PO x 2 days |
| Measles supplementation (1-5 yr) | 200,000 IU/day PO x 2 days |
| Malabsorption prophylaxis (>8 yr, adult) | 10,000-50,000 IU/day PO (water-miscible) |
| Cystic fibrosis (infant) | 1,500 IU/day PO |
| Cystic fibrosis (1-3 yr) | 5,000 IU/day PO |
| Cystic fibrosis (4-8 yr) | 5,000-10,000 IU/day PO |
| Cystic fibrosis (≥9 yr) | 10,000 IU/day PO |
Formulations: Caps (7,500-25,000 IU), Tabs (10,000-15,000 IU), Oral drops (2,500 IU/0.3 mL), IM injection (Aquasol A: 50,000 IU/mL).
Important: High-dose vitamin A is teratogenic (Category X). Never use above the RDA in pregnancy.
Lab Reference
- Normal serum retinol: lower limit 20 mcg/dL
- Toxicity suggested: >100 mcg/dL (Bradley & Daroff's Neurology)
Sources:
- Robbins & Kumar Basic Pathology, pp. 292-293
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- Bradley and Daroff's Neurology in Clinical Practice
- The Harriet Lane Handbook, 23rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.