Acute coronary syndrome
Reading File
Finding Sources
Searching PubMed
"acute coronary syndrome"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
The large truncated output from my previous call (offset 2443) contained the full management details. I now have comprehensive information from Goldman-Cecil Medicine. Let me compile the full answer using all the content gathered.
Acute Coronary Syndrome (ACS)
Definition and Classification
Acute coronary syndrome describes the continuum of myocardial ischemia or infarction. It encompasses three entities:
| Entity | Troponin | ECG | Mechanism |
|---|---|---|---|
| Unstable Angina (UA) | Negative | No ST elevation | Subtotal occlusion, no necrosis |
| NSTEMI | Positive | No ST elevation | Subtotal occlusion with necrosis |
| STEMI | Positive | Persistent ST elevation (>20 min) | Total occlusion |
UA and NSTEMI together are termed Non-ST Elevation ACS (NSTE-ACS) because they share the absence of ST elevation and similar initial management.
Epidemiology
- ~1.2 million hospitalizations annually in the United States
- ~2/3 are NSTE-ACS; 1/3 are STEMI
-
50% of NSTE-ACS patients are older than 65 years; nearly half are women
- Risk factors: atherosclerosis, peripheral vascular disease, chronic inflammatory disorders (rheumatoid arthritis, psoriasis, lupus, chronic infection)
Pathophysiology
Type 1 MI (Most Common)
The precipitating event is atherosclerotic plaque rupture or erosion, followed by:
- Platelet adhesion, activation, and aggregation at the ruptured plaque
- Thrombus formation -> partial (NSTEMI/UA) or complete (STEMI) coronary occlusion
- Downstream myocardial ischemia/necrosis
Mechanisms of plaque vulnerability:
- Inflammatory cells (macrophages, T-lymphocytes) secrete cytokines (TNF, IL-1, IFN-γ) that inhibit collagen synthesis
- Matrix metalloproteinases and cathepsins degrade the fibrous cap
- Sites of low shear stress (vessel bifurcations) accumulate lipids and inflammatory cells, thinning the fibrous cap
- Rich plaque neovascularization (driven by VEGF, FGF, placental growth factor) contributes to intraplaque hemorrhage and rupture
Type 2 MI (Oxygen Supply-Demand Mismatch)
Caused by conditions other than plaque rupture:
- Supply reduction: severe hypotension, anemia, hypoxemia, coronary vasospasm (Prinzmetal angina), cocaine, chemotherapy, triptans, spontaneous coronary artery dissection (most common in peripartum women)
- Demand increase: severe tachycardia, hypertensive crisis, thyrotoxicosis
Clinical Features
Symptoms
- Classic: Chest pressure/tightness, radiation to left arm, jaw, or neck; diaphoresis, nausea, shortness of breath
- Atypical (more common in elderly, women, diabetics): dyspnea alone, syncope, fatigue, abdominal pain, diaphoresis, back/shoulder pain, delirium
- In patients ≥85 years, classic chest pain is present in only ~50% of STEMI cases
- One-third of women >65 years with MI present with abdominal pain alone
Physical Examination
- May be entirely normal
- Signs of heart failure: S3 gallop, pulmonary crackles, elevated JVP
- Mitral regurgitation murmur (papillary muscle dysfunction/rupture)
- Cardiogenic shock: hypotension, cool extremities, altered mental status
Diagnosis
ECG
- STEMI: New ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads; new LBBB; posterior MI (ST depression V1-V3 with tall R waves)
- NSTEMI/UA: ST depression, T-wave inversions, or normal ECG
- Serial ECGs are essential - initial ECG may be normal in up to 50% of ACS
Biomarkers
- Troponin I and T (high-sensitivity): Gold standard for myocardial necrosis. Rise within 3-4 hours, peak at 12-24 hours, remain elevated 7-10 days
- CK-MB: Less sensitive/specific; useful for re-infarction (returns to normal in 48-72 hours)
- Serial troponins (at 0 and 3 hours, or 0 and 1 hour with hs-troponin) are required to rule in or rule out MI
- Troponin elevation without ACS: myocarditis, PE, sepsis, heart failure, renal failure (type 2 MI or myocardial injury)
Imaging
- CXR: Pulmonary edema, cardiomegaly, alternative diagnoses (aortic dissection)
- Echocardiography: Regional wall motion abnormalities confirm ischemia, assess LV function, detect complications (VSD, free wall rupture, pericardial effusion)
- Coronary angiography: Definitive diagnosis and revascularization
Risk Stratification Tools
- TIMI Score (0-7): Predicts 14-day MACE in NSTE-ACS
- GRACE Score: Better calibrated for in-hospital and 6-month mortality
- HEART Score: Used in the ED to risk-stratify chest pain
Management
Immediate General Measures (All ACS)
- MONA: Morphine (for refractory pain), Oxygen (if SpO2 <90%), Nitrates (sublingual/IV for ongoing pain), Aspirin 162-325 mg chewed immediately
- Continuous ECG monitoring, IV access, bedrest
- Avoid NSAIDs (increase cardiovascular risk)
Antiplatelet Therapy
- Aspirin: 162-325 mg loading, then 75-100 mg daily indefinitely
- P2Y12 inhibitors (dual antiplatelet therapy, DAPT):
- Ticagrelor 180 mg load, 90 mg twice daily (preferred over clopidogrel for ACS)
- Prasugrel 60 mg load, 10 mg daily (avoid if prior stroke/TIA, age ≥75, weight <60 kg)
- Clopidogrel 300-600 mg load, 75 mg daily (when others contraindicated)
- DAPT duration: 12 months post-ACS; may extend or de-escalate based on bleeding/ischemic risk
- Recent meta-analyses (2024-2025) support de-escalation to ticagrelor monotherapy after 3-6 months as safe and possibly preferable to reduce bleeding (Lancet 2024, PMID 39226909)
Anticoagulation
- UFH (unfractionated heparin): IV bolus + infusion; standard for PCI
- Enoxaparin: 1 mg/kg SC twice daily; preferred for medical management
- Fondaparinux: 2.5 mg SC daily; lowest bleeding risk; not for use during PCI alone
- Bivalirudin: IV direct thrombin inhibitor; used during PCI
Anti-Ischemic Therapy
- Beta-blockers: Metoprolol or carvedilol; reduce heart rate and oxygen demand; start oral within 24 hours if no contraindications (acute HF, low-output state, AV block, reactive airway)
- Nitrates: IV nitroglycerin for ongoing ischemia, hypertension, or pulmonary edema
- Calcium channel blockers: Non-dihydropyridines (diltiazem, verapamil) when beta-blockers contraindicated; avoid if LV dysfunction
- ACE inhibitors/ARBs: Start within 24 hours; beneficial in EF <40%, anterior MI, diabetes, hypertension
Statins
- High-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg) immediately; reduce recurrent events independent of LDL level
Reperfusion Strategy
STEMI
Time is muscle - every minute counts.
- Primary PCI (preferred): Target door-to-balloon time <90 minutes (or <120 min if transferred). Superior to thrombolysis in reducing mortality, recurrent MI, and stroke when performed in time.
- Fibrinolytic therapy (if PCI unavailable within 120 min): tPA, tenecteplase, reteplase. Door-to-needle time <30 min. Absolute contraindications: prior intracranial hemorrhage, ischemic stroke <3 months, active bleeding, suspected aortic dissection.
- Rescue PCI: After failed thrombolysis (persistent ST elevation >50% or hemodynamic instability)
NSTE-ACS
- Early invasive strategy (coronary angiography within 24-72 hours): preferred for intermediate-high risk (elevated troponin, new ST changes, GRACE score >140, hemodynamic instability, refractory ischemia)
- Conservative (ischemia-guided) strategy: For low-risk patients or those with significant comorbidities
- Recent 2025 meta-analysis (PMID 40549394) supports early invasive approach even in older patients
Complications
| Complication | Timing | Features |
|---|---|---|
| Cardiogenic shock | Hours | Hypotension, poor perfusion; highest mortality |
| Acute HF/pulmonary edema | Hours-days | Dyspnea, crackles, hypoxia |
| Ventricular arrhythmias (VF, VT) | Hours | Most common cause of pre-hospital death |
| Papillary muscle rupture | 2-7 days | Acute MR, flash pulmonary edema |
| Ventricular septal rupture | 3-5 days | New harsh systolic murmur, biventricular failure |
| Free wall rupture | 1-10 days | Cardiac tamponade, electromechanical dissociation |
| Pericarditis (Dressler's) | 1-8 weeks | Pleuritic chest pain, friction rub, fever |
| LV thrombus | Days-weeks | Anteroapical MI; anticoagulate with heparin/warfarin |
| RV infarction | At presentation | Hypotension + clear lungs + JVD; avoid nitrates/diuretics; use IV fluids + early PCI |
Secondary Prevention (Post-Discharge)
| Drug Class | Agent | Indication |
|---|---|---|
| Antiplatelet | Aspirin + P2Y12 x 12 months | All ACS |
| Beta-blocker | Metoprolol succinate/carvedilol | EF ≤40% or post-MI (continue ≥3 years) |
| ACE inhibitor/ARB | Ramipril, lisinopril | All, especially EF ≤40% |
| Statin | Atorvastatin 80 mg | All ACS |
| Aldosterone antagonist | Eplerenone | EF ≤35% + HF or diabetes |
Additional measures:
- Cardiac rehabilitation (reduces mortality ~20-25%)
- Smoking cessation
- Blood pressure control (<130/80 mmHg)
- Diabetes management (HbA1c <7%)
- Physical activity (30 min moderate exercise 5 days/week after recovery)
- SGLT2 inhibitors (empagliflozin, dapagliflozin) in post-MI HFrEF for cardiorenal protection
Special Populations
Elderly (>75 years)
- Atypical presentations predominate; ACS may mimic HF, syncope, or delirium
- Higher risk of bleeding with anticoagulants - dose-adjust enoxaparin
- Early invasive approach still beneficial (After Eighty Study: superior outcomes vs. conservative in stable octogenarians)
- Acute HF at presentation occurs in ~50% of STEMI patients ≥85 years (vs. only 1.7% in those <65 years)
Women
- More likely to present atypically; diagnosis often delayed
- Higher rates of type 2 MI; spontaneous coronary artery dissection more common
- Similar benefit from reperfusion; slightly higher bleeding risk with anticoagulants
Diabetes
- Often "silent" MI; higher risk of multivessel disease
- Aggressive glycemic and cardiovascular risk factor control; SGLT2 inhibitors reduce CV events
Key Recent Evidence Updates (2024-2025)
- De-escalation of DAPT (PMID 39226909): Ticagrelor monotherapy after 3-6 months post-PCI reduces bleeding without increasing ischemic events vs. 12-month DAPT.
- Elderly ACS strategy (PMID 40549394): Meta-analysis confirms early invasive approach reduces major adverse cardiac events in older ACS patients.
- Monotherapy after PCI (PMID 40803759): P2Y12 inhibitor monotherapy (especially ticagrelor) may be preferred over aspirin monotherapy after short-course DAPT in ACS post-PCI.
Sources: Goldman-Cecil Medicine, 27th Edition (Chapter 57); Rosen's Emergency Medicine, 9th Edition; Harrison's Principles of Internal Medicine
Asthma
Reading File
Finding Sources
Searching PubMed
"asthma"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive asthma overview. Let me compile the full answer.
Asthma
Definition
Asthma is a chronic inflammatory airway disease characterized by mostly reversible airway obstruction resulting from bronchial smooth muscle contraction, mucosal edema, and excessive mucus secretion in response to various triggers. Unlike COPD, it is not a progressive disease - but if left untreated, it can cause permanent airway remodeling, increasing exacerbation frequency and severity.
Epidemiology
- Affects ~300 million people worldwide; one of the most common chronic diseases globally
- Global burden data (Lancet Respir Med, 2025, PMID 40147466): 262 million cases in 2021, with projections to increase by 2050
- Prevalence highest in high-income English-speaking countries
- ~4% of pregnant women have asthma; one-third experience exacerbations during pregnancy
- Risk factors: atopy, family history, allergen exposure, air pollution, obesity, early childhood respiratory infections
Pathophysiology
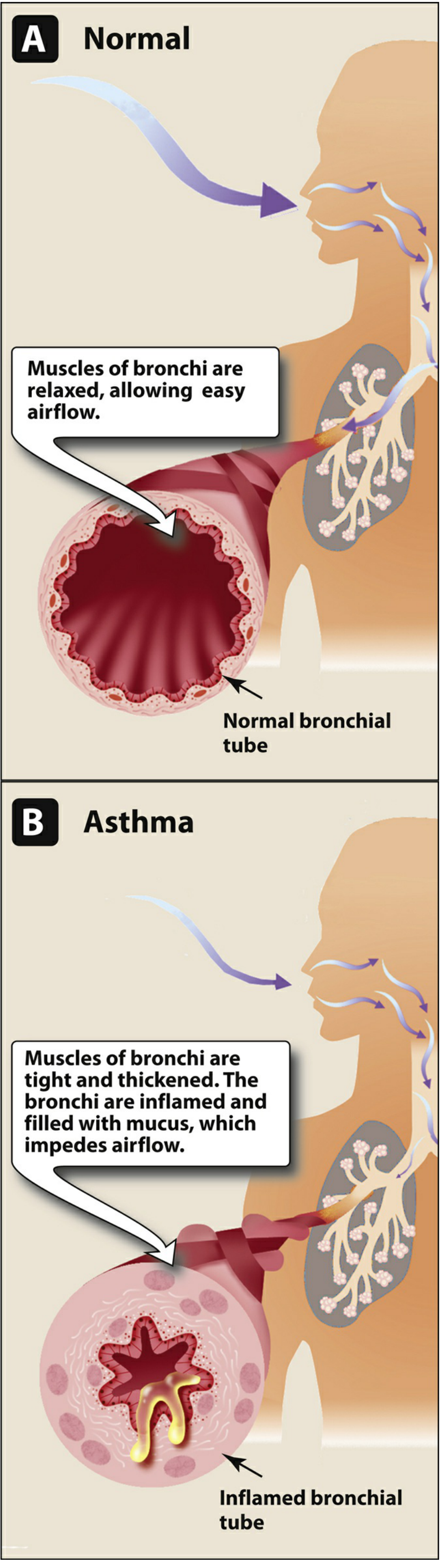
Airflow obstruction arises from three mechanisms acting together:
- Bronchial smooth muscle contraction (bronchoconstriction) - the dominant acute component
- Mucosal inflammation and edema - driven by eosinophils, mast cells, T lymphocytes, macrophages
- Hypersecretion of mucus - plugging small airways
Inflammatory Cascade
- Allergen exposure -> IgE-mediated mast cell activation -> release of histamine, prostaglandins, leukotrienes
- Eosinophil recruitment driven by IL-5
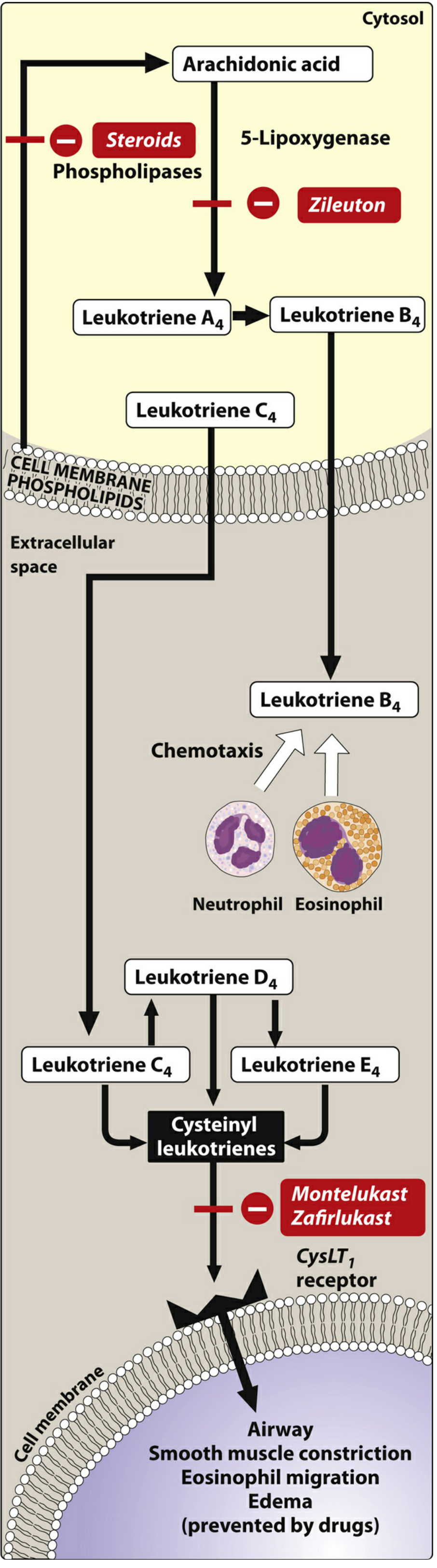
- Cysteinyl leukotrienes (LTC4, LTD4, LTE4) cause smooth muscle contraction, mucosal edema, eosinophil migration
- Chronic inflammation leads to airway remodeling: subepithelial fibrosis, smooth muscle hypertrophy/hyperplasia, angiogenesis, and mucous gland enlargement
Drug targets in the leukotriene pathway:
Common Triggers
- Allergens (house dust mite, pollen, pet dander, mold)
- Respiratory infections (viral URTIs are the most common trigger)
- Exercise (especially in cold/dry air)
- Air pollutants, smoke, strong odors
- NSAIDs/aspirin (aspirin-exacerbated respiratory disease)
- Beta-blockers
- GERD, emotional stress, cold air
Clinical Features
Symptoms (classic triad)
- Wheeze - polyphonic, expiratory (can be absent in very severe attack - "silent chest")
- Dyspnea - especially nocturnal or early morning (circadian variation in airway tone)
- Cough - may be the only symptom (cough-variant asthma); often worse at night
Signs
- Mild-moderate attack: Tachypnea, expiratory wheeze, prolonged expiratory phase, use of accessory muscles
- Severe attack: Inability to complete sentences, SpO2 <92%, pulsus paradoxus >25 mmHg, silent chest (ominous), cyanosis
- Between attacks: physical exam may be completely normal
Diagnosis
Spirometry (cornerstone)
- Obstructive pattern: FEV1/FVC ratio <0.70 (or below lower limit of normal)
- Reversibility: ≥12% AND ≥200 mL improvement in FEV1 after bronchodilator - confirms asthma
- FEV1 may be normal in mild asthma; serial measurements are important
Bronchoprovocation Testing
- Methacholine challenge: PC20 (concentration causing ≥20% fall in FEV1) is diagnostic of airway hyperresponsiveness
- Used when spirometry is normal but asthma is suspected
Peak Expiratory Flow (PEF)
- Daily PEF monitoring: diurnal variation >20% is diagnostic
- Home monitoring guides step-up/step-down therapy
Additional Tests
- FeNO (fractional exhaled nitric oxide): Elevated (>25 ppb) indicates eosinophilic airway inflammation; predicts corticosteroid response
- Blood eosinophil count: Useful for phenotyping and biologic eligibility
- Serum IgE + skin prick testing: Identifies allergic triggers
- CXR: Usually normal; may show hyperinflation during exacerbation; rules out alternative diagnoses
ATS Impairment Rating (for disability assessment)
| Domain | Metric | Score 0 → 4 |
|---|---|---|
| A | Post-bronchodilator FEV1 (% predicted) | >LLN → <50% |
| B | FEV1 reversibility or PC20 | <10% → ≥30% |
| C | Minimum medication need | None → daily oral steroids |
Classification (GINA Framework)
By Symptom Control (treatment-based, GINA preferred)
| Severity | Definition |
|---|---|
| Mild | Well controlled on Step 1 or Step 2 treatment |
| Moderate | Well controlled on Step 3 treatment |
| Severe | Requires Step 4-5 to remain controlled, or is still uncontrolled |
By Symptom Frequency (NHLBI/traditional classification)
| Category | Daytime Symptoms | Nocturnal | FEV1 |
|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2x/month | ≥80% |
| Mild persistent | >2 days/week but not daily | 3-4x/month | ≥80% |
| Moderate persistent | Daily | >1x/week | 60-79% |
| Severe persistent | Continuous | Frequent (7x/week) | <60% |
Pharmacological Management (GINA Stepwise)
Key Drug Classes
1. Inhaled Corticosteroids (ICS) - Controller Foundation
- Mechanism: Inhibit phospholipase A2 → block arachidonic acid release → reduce leukotriene synthesis and eosinophilic inflammation; reverse mucosal edema, decrease capillary permeability
- Examples: Budesonide, fluticasone propionate/furoate, beclomethasone, mometasone, ciclesonide
- Must be used regularly to achieve benefit; several months of use reduce airway hyperresponsiveness
- Adverse effects: Oropharyngeal candidiasis, hoarseness (rinse mouth after use); high-dose systemic effects (adrenal suppression, cataracts, osteoporosis)
2. Short-Acting Beta-2 Agonists (SABA) - Reliever
- Examples: Albuterol (salbutamol), levalbuterol
- Mechanism: Activate beta-2 receptors → smooth muscle relaxation → bronchodilation
- Onset within minutes; used for acute symptom relief
- GINA update: SABA-only treatment (without ICS) is no longer first-line; as-needed low-dose ICS-formoterol preferred
3. Long-Acting Beta-2 Agonists (LABA) - Controller Add-on
- Examples: Formoterol (fast-onset), salmeterol
- Must never be used as monotherapy in asthma (FDA black box warning - increased asthma deaths)
- Always combine with ICS; ICS-LABA combinations preferred for moderate-severe asthma
- Low-dose ICS-LABA is equally effective as high-dose ICS alone for moderate-severe asthma
4. Leukotriene Receptor Antagonists (LTRA)
- Montelukast, zafirlukast - block CysLT1 receptor
- Block smooth muscle contraction, edema, eosinophil migration
- Useful adjuncts; especially beneficial in aspirin-exacerbated asthma and allergic rhinitis-asthma overlap
- Montelukast: FDA black box warning for neuropsychiatric events (mood changes, suicidality)
5. Zileuton (5-Lipoxygenase Inhibitor)
- Blocks 5-lipoxygenase → prevents leukotriene A4 synthesis → inhibits all leukotrienes
- Hepatotoxic; requires LFT monitoring
6. Anticholinergics
- Ipratropium (SAMA): Add-on to SABA in acute exacerbations in ED; not for routine maintenance
- Tiotropium (LAMA): Add-on therapy in severe asthma with frequent exacerbations; also useful in asthma-COPD overlap
7. Theophylline
- Methylxanthine bronchodilator; has anti-inflammatory properties
- Largely replaced by safer agents; narrow therapeutic index (seizures, fatal arrhythmias at toxic levels)
- Monitor serum concentrations; multiple CYP1A2 drug interactions
GINA Stepwise Treatment (Ages ≥12 years)
| Step | Symptoms | Preferred Controller | Preferred Reliever |
|---|---|---|---|
| Step 1 | <2x/month | Low-dose ICS-formoterol as needed | (same - as needed only) |
| Step 2 | >2x/month, <4-5 days/week | Low-dose ICS-formoterol as needed | (same) |
| Step 3 | Most days or awakening ≥1x/week | Low-dose ICS-formoterol maintenance | Low-dose ICS-formoterol PRN |
| Step 4 | Daily symptoms, low lung function | Medium-dose ICS-formoterol maintenance | Low-dose ICS-formoterol PRN |
| Step 5 | Uncontrolled on Step 4 | Add biologic therapy or tiotropium | Low-dose ICS-formoterol PRN |
Alternative (ICS + SABA regimen): Low-dose maintenance ICS + SABA as needed at Steps 1-2; medium/high-dose ICS-LABA at Steps 3-4.
Biologic Therapies (Step 5 Add-on)
For severe asthma unresponsive to Steps 4-5 conventional therapy:
| Biologic | Target | Indication | Dosing |
|---|---|---|---|
| Omalizumab | Free IgE | Moderate-severe allergic asthma; IgE 30-700 IU/mL; ≥6 years | SC every 2-4 weeks |
| Mepolizumab | IL-5 ligand | Severe eosinophilic asthma; AEC ≥150-300 cells/μL; ≥6 years | 100 mg SC q4 weeks |
| Reslizumab | IL-5 ligand | Severe eosinophilic asthma; AEC ≥400 cells/μL; ≥18 years | 3 mg/kg IV q4 weeks |
| Benralizumab | IL-5 receptor-α | Severe eosinophilic asthma; AEC ≥300 cells/μL; ≥12 years | 30 mg SC q4wk x3, then q8wk |
| Dupilumab | IL-4 receptor-α (blocks IL-4 + IL-13) | Severe eosinophilic or T2 asthma; AEC ≥150 or FeNO ≥25 ppb; ≥12 years | 400-600 mg loading, then 200-300 mg SC q2wk |
All biologics reduce exacerbations and hospitalizations; dupilumab additionally reduces oral steroid dependence. Adverse effects include anaphylaxis (rare), arthralgias, fever, rash, and increased infection risk.
Acute Exacerbation Management
Severity Assessment
| Feature | Mild-Moderate | Severe | Life-Threatening |
|---|---|---|---|
| Speaks in | Full sentences | Phrases | Words/unable |
| RR | <25/min | 25-30/min | >30/min |
| HR | <110/min | 110-130/min | >130 or bradycardia |
| SpO2 | ≥94% | 90-94% | <90% |
| PEF | >50% predicted | 33-50% | <33% ("near fatal") |
| Auscultation | Wheeze | Wheeze | Silent chest |
ED Treatment
Step 1 - Bronchodilation (all severities):
- Inhaled SABA (albuterol) - mainstay; MDI with spacer as effective as nebulizer for mild-moderate; continuous nebulization for severe
- MDI-based approach causes fewer side effects (less tachycardia, nausea, tremor) vs. nebulizer
Step 2 - Corticosteroids (moderate-severe):
- Oral prednisone/prednisolone 40-60 mg OR IV methylprednisolone (preferred if unable to swallow)
- Start within the first hour of ED presentation - reduces hospitalization risk and relapse
- Response begins within 1 hour; maximal at 8-12 hours
- Dexamethasone single dose (0.6 mg/kg) has shown equivalent efficacy to 5-day prednisolone course
- No taper needed for short courses (<2 weeks)
Step 3 - Anticholinergics (severe/refractory):
- Ipratropium bromide added to SABA in severe exacerbations; reduces hospitalizations
Step 4 - Refractory/Severe:
- IV magnesium sulfate (2 g over 20 min): Smooth muscle relaxation via calcium channel blockade; used for severe cases not responding to initial treatment (PMID 38395640 - supported in pediatric meta-analysis)
- IV beta-2 agonists: When inhaled route is insufficient due to severely diminished air entry
- Heliox (70:30 helium-oxygen): Reduces airway resistance; bridging therapy
- IV theophylline: Rarely used; risk of toxicity
- Intubation and mechanical ventilation: Last resort; use permissive hypercapnia strategy
Disposition
- Mild exacerbation with good response: Discharge with SABA + short oral steroid course
- ICS should be prescribed at discharge for all persistent asthma (not mild intermittent)
- Identify and address triggers; check inhaler technique
- Follow-up within 1-2 weeks
Special Populations
Asthma in Pregnancy
- ~4% of pregnant women affected; 1/3 experience exacerbations
- Moderate-severe asthma increases risk of preterm birth, low birth weight, preeclampsia, perinatal death
- Pregnancy physiology: Tidal volume and minute ventilation increase (progesterone effect); FEV1, FVC, and PEFR remain unchanged; residual volume decreases
- Untreated asthma is more dangerous to the fetus than treating with medications
- Albuterol: safe for all severity levels; ICS budesonide: first-line controller (most safety data)
- Oral corticosteroids: safe for exacerbations; minimal risk of cleft palate with brief courses
- Avoid leukotriene antagonists as first-line unless well-controlled pre-pregnancy
Exercise-Induced Bronchoconstriction (EIB)
- SABA 10-15 minutes before exercise as pretreatment
- ICS reduces baseline airway inflammation and prevents EIB
- Warm-up exercise and wearing a face mask in cold weather reduces EIB
Occupational Asthma
- Work-related new-onset asthma (sensitizer-induced) or worsening of pre-existing asthma
- Common sensitizers: isocyanates, flour, animal proteins, latex
- Remove from exposure early; ICS + allergen avoidance
Monitoring and Follow-Up
- Asthma Control Test (ACT): 5-item validated tool; score ≤19 = uncontrolled
- Asthma Control Questionnaire (ACQ): Score ≥1.5 = uncontrolled
- Assess: Symptom frequency, reliever use, nocturnal awakening, activity limitation, exacerbations, spirometry
- Step up if uncontrolled; step down if well controlled for ≥3 months
- Review inhaler technique and adherence at every visit - poor technique is a major cause of treatment failure
- Avoid known triggers (allergen avoidance, smoking cessation, treat GERD)
Complications
| Complication | Notes |
|---|---|
| Status asthmaticus | Severe attack unresponsive to initial bronchodilator therapy; can be fatal |
| Pneumothorax/pneumomediastinum | From high intrathoracic pressures during severe attack |
| Airway remodeling | Subepithelial fibrosis, irreversible fixed obstruction (asthma-COPD overlap) |
| Respiratory failure | Hypercapnia is an ominous late sign; indicates fatigue and impending arrest |
| Cor pulmonale | Long-term severe uncontrolled asthma |
Key Recent Evidence (2024-2026)
- Global burden (PMID 40147466): 262 million cases globally in 2021; atopic dermatitis-asthma overlap is growing
- IV magnesium sulfate in children (PMID 38395640): Meta-analysis confirms benefit of IV MgSO4 in pediatric exacerbations not responding to initial therapy
- ARIA-EAACI guidelines 2024-2025 (PMID 41324154): Intranasal corticosteroids remain first-line for allergic rhinitis, which is a key driver of asthma control
Sources: Lippincott Illustrated Reviews: Pharmacology; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Tintinalli's Emergency Medicine; Washington Manual of Medical Therapeutics; Textbook of Family Medicine
This is a shared conversation. Sign in to Orris to start your own chat.