stroke general medicine mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"ischemic stroke" AND "treatment"
I now have comprehensive content from the textbooks and recent PubMed evidence. Let me compile the full MBBS-level stroke guide.
Stroke - General Medicine (MBBS)
Classification
Stroke is broadly divided into:
| Type | Proportion |
|---|---|
| Ischemic stroke | ~85% |
| Hemorrhagic stroke - Intracerebral (ICH) | ~10-15% |
| Hemorrhagic stroke - Subarachnoid (SAH) | ~5% |
1. Ischemic Stroke
Definition
Acute focal neurological deficit caused by thrombotic or embolic occlusion of a cerebral artery, resulting in brain infarction.
Vascular Anatomy (Circle of Willis)
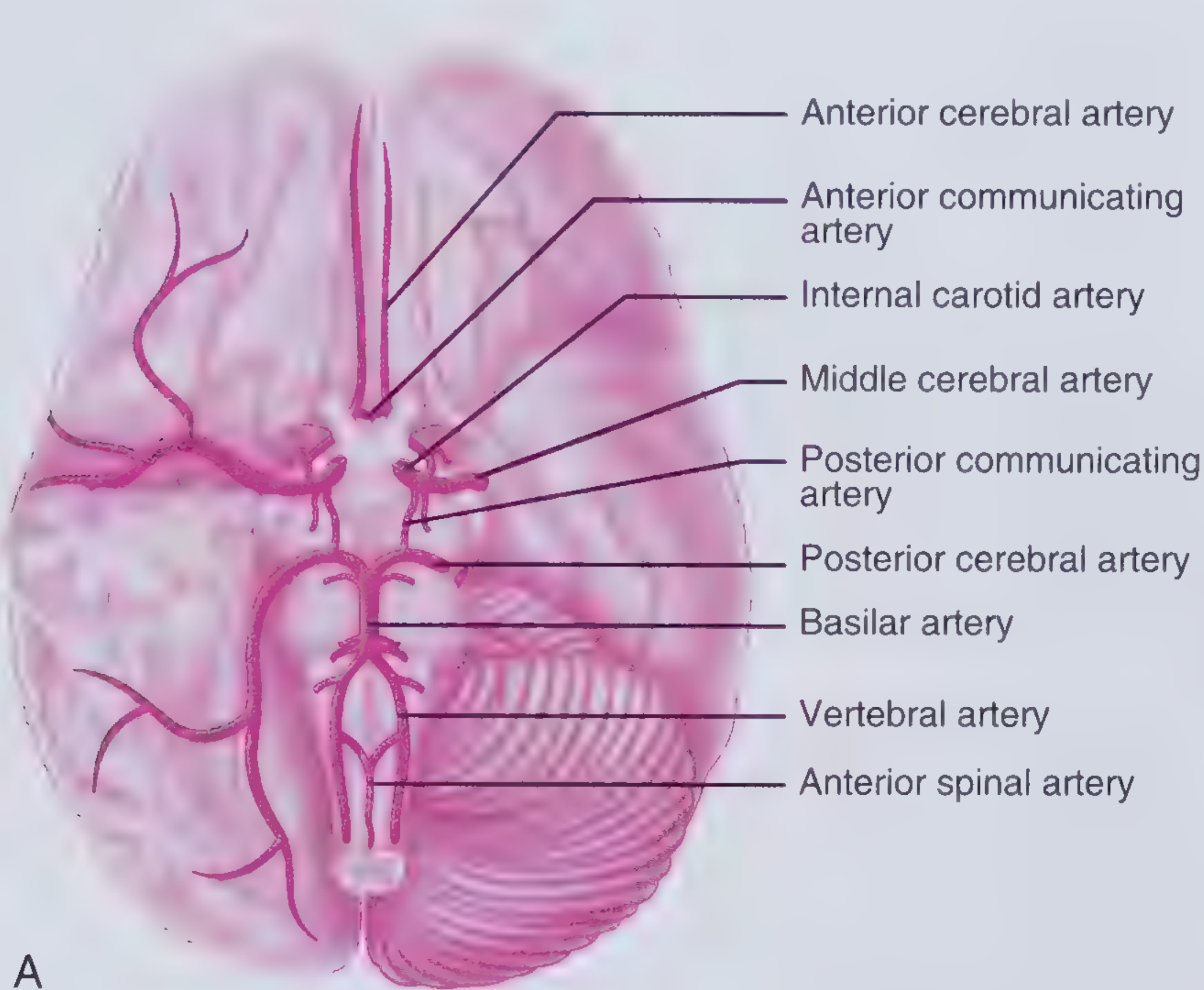
- Anterior circulation: ICA → MCA + ACA (supplies most of cerebral hemispheres)
- Posterior circulation: Vertebral arteries → Basilar artery → PCA (supplies brainstem, cerebellum, occipital & medial temporal lobes)
- The Circle of Willis provides an anastomosis allowing collateral flow when one system is compromised.
Subtypes of Ischemic Stroke
1. In situ thrombosis (large vessel atherosclerosis)
- Atherosclerotic plaques in large vessels (ICA, MCA, vertebral/basilar arteries) rupture and cause local thrombus formation
- Gradual onset, often with preceding TIA ("stuttering" course)
- TOAST classification category: Large artery atherosclerosis
2. Embolic stroke
- Cardioembolic (most common embolic cause): Atrial fibrillation, mural thrombus (post-MI), dilated cardiomyopathy, valvular disease (mitral stenosis), infective endocarditis
- Artery-to-artery embolism: Atherosclerotic plaque fragments travel distally
- Paradoxical embolism: Venous thrombus crosses a patent foramen ovale (PFO) to enter arterial circulation
- Clinical clue: Multiple vascular territory involvement; sudden onset with maximum deficit at onset
3. Small vessel disease (lacunar stroke)
- Affects penetrating arteries (<1.5 mm diameter) supplying basal ganglia, thalamus, internal capsule, pons
- Caused by lipohyalinosis (fibrinoid/lipid deposition causing luminal obliteration) or microatheroma - both linked to chronic hypertension
- Pure motor, pure sensory, sensorimotor, ataxic hemiparesis, clumsy-hand dysarthria syndromes
- Normal cortex (no aphasia, no neglect, no visual field defects)
4. Watershed (borderzone) infarction
- Occurs at junctions between major vascular territories during systemic hypotension or severe ICA stenosis
- Most often subcortical watershed ("man-in-a-barrel" syndrome when bilateral)
5. Other/cryptogenic
- Cervical artery dissection (~20% of strokes in young/middle-aged adults)
- Hypercoagulable states (antiphospholipid syndrome, protein C/S deficiency, polycythemia vera)
- Vasculitis, fibromuscular dysplasia, Moyamoya disease
TOAST Classification Summary
| Category | Key Feature |
|---|---|
| Large artery atherosclerosis | Stenosis >50% in major artery |
| Cardioembolism | AF, recent MI, valve disease |
| Small vessel occlusion | Lacunar syndrome + small infarct |
| Other determined etiology | Dissection, vasculitis, hypercoagulable |
| Undetermined (cryptogenic) | No cause found after workup |
Clinical Features by Artery
| Artery | Territory | Clinical Features |
|---|---|---|
| MCA (most common) | Lateral hemisphere | Contralateral hemiplegia (arm > leg), hemianesthesia, homonymous hemianopia; dominant hemisphere: aphasia; non-dominant: neglect/anosognosia |
| ACA | Medial frontal/parietal | Contralateral leg > arm weakness, gait apraxia, abulia |
| PCA | Occipital, thalamus | Homonymous hemianopia, thalamic pain, memory loss |
| Basilar artery | Brainstem, cerebellum | "Locked-in" syndrome, quadriplegia, cranial nerve palsies, cerebellar signs, coma |
| PICA | Lateral medulla | Wallenberg syndrome: ipsilateral face + contralateral body sensory loss, Horner's, dysphagia, vertigo |
TIA (Transient Ischemic Attack)
- Same mechanism as ischemic stroke but symptoms resolve within 24 hours (classically; newer tissue-based definition: no infarct on MRI)
- High short-term stroke risk: 10-15% within 3 months, with greatest risk in first 48 hours
- ABCD2 score (Age, Blood pressure, Clinical features, Duration, Diabetes) guides urgency of workup
2. Hemorrhagic Stroke
A. Intracerebral Hemorrhage (ICH)
Risk factors: Hypertension (most common), older age, Black/Asian ethnicity, excessive alcohol use, low LDL
Causes:
- Hypertensive vasculopathy (lipohyalinosis of deep penetrating arteries)
- Cerebral amyloid angiopathy (CAA): Amyloid deposition in leptomeningeal/cortical vessels → lobar hemorrhages in elderly
- AVM, cavernous malformation
- Coagulopathy, anticoagulant use
- Trauma (ICH in ~50% of traumatic brain injury patients)
- Hemorrhagic transformation of ischemic stroke (spontaneous: ~2nd week; with thrombolytics: earlier)
Location by cause:
- Hypertension: Putamen/internal capsule (most common), thalamus, pons, cerebellum
- CAA: Lobar (cortical/subcortical)
- CVT: Adjacent to affected vein; hyperattenuating cortical/deep vein on CT is a clue
CT appearance:
- Hyperattenuating (bright) round/oval lesion on non-contrast CT
- Early: 40-60 HU (heterogeneous) → 60-80 HU within hours/days → 80-100 HU over days (homogeneous hyperdense clot)
- Surrounding hypodense edema ring
Clinical presentation:
- Sudden onset headache + focal neurological deficits + nausea/vomiting + elevated BP
- Consciousness impairment depends on size and location
B. Subarachnoid Hemorrhage (SAH)
Causes: Ruptured berry (saccular) aneurysm (~85%), AVM, perimesencephalic non-aneurysmal SAH (better prognosis)
Risk factors: Family history, hypertension, hyperlipidemia, smoking (4 strongest)
Classic presentation: "Thunderclap headache" - worst headache of life, sudden onset; meningism (neck stiffness, photophobia), ± loss of consciousness, nausea/vomiting
Sentinel headache: Sudden severe headache preceding major SAH by up to 2 weeks
Diagnosis: Non-contrast CT (sensitive in first 12 hours) → if CT negative and clinical suspicion high: lumbar puncture (xanthochromia)
3. Diagnosis
Initial Assessment - Imaging
- Non-contrast CT brain: First-line, immediate - rules out hemorrhage, guides tPA eligibility
- Ischemic: May be normal in first hours; early signs: loss of gray-white differentiation at insular cortex, sulcal effacement, hypodense basal ganglia, "dense MCA sign" (hyperdense clot in proximal MCA)
- Hemorrhagic: Hyperattenuating lesion
- CT Angiography (CTA): Identifies vessel occlusion and stenosis (sensitivity ~97%, specificity ~99.5% for >50% stenosis)
- MRI DWI (Diffusion-Weighted Imaging): Most sensitive for acute ischemia (detects within minutes of onset); restriction of diffusion = cytotoxic edema
- CT Perfusion / MR Perfusion: Identifies ischemic penumbra (tissue at risk); used for extended thrombolysis/thrombectomy window decisions
- ASPECTS score: Summarizes early CT ischemic changes in MCA territory (max 10 = normal; <7 = poor prognosis)
Workup (after stabilization)
- ECG and cardiac monitoring: Look for AF
- Echocardiography: Mural thrombus, valvular disease, PFO
- Carotid Doppler ultrasound / CTA neck: Carotid stenosis, dissection
- Lipid profile, fasting glucose, HbA1c
- CBC, coagulation studies
- In young patients: Thrombophilia screen, homocysteine, antiphospholipid antibodies
4. Treatment
Acute Ischemic Stroke
Time is brain: ~1.9 million neurons die every minute during ischemic stroke
IV Thrombolysis (tPA)
- Drug: Alteplase (recombinant tPA), 0.9 mg/kg IV (max 90 mg), 10% as bolus + 90% over 1 hour
- Window: Up to 4.5 hours from symptom onset
- Key contraindications: Active bleeding, recent surgery, prior ICH, platelets <100,000, INR >1.7, systolic BP >185 mmHg (uncontrolled), blood glucose <50 or >400
- Main risk: Symptomatic intracranial hemorrhage in ~6% (NINDS trial)
- Hemorrhagic conversion risk factors: Older age, higher NIHSS (worse deficit), early infarct signs on CT, dense MCA sign, hyperglycemia, hypertension, longer time to treatment
- Patients benefitting from 3-4.5 hour window: Age <80, NIHSS ≤25, no prior stroke + diabetes combined, not on anticoagulation
- Tenecteplase is emerging as an alternative (single bolus, recent meta-analyses [PMID 39413337] show non-inferiority to alteplase within 4.5 hours)
Mechanical Thrombectomy
- Endovascular removal of clot using stent-retriever or aspiration device
- For large vessel occlusion (ICA, M1-MCA, basilar)
- Traditional window: up to 6 hours; can extend to 24 hours with favorable perfusion imaging (penumbra present)
- Landmark trials: MR CLEAN, EXTEND-IA, SWIFT PRIME
- Can be combined with tPA or used alone if tPA contraindicated
Blood Pressure Management (Acute)
- If tPA given: Maintain BP <180/105 mmHg
- If tPA not given: Permissive hypertension (allow up to 220/120 mmHg) - avoid aggressive lowering as it reduces perfusion to ischemic penumbra
- Exceptions: Hypertensive emergency with end-organ damage
Antiplatelet Therapy
- Aspirin 300 mg oral ASAP (if no hemorrhage and not thrombolysed, or 24 hours after tPA)
- For secondary prevention: Aspirin 75-100 mg daily; or clopidogrel; or aspirin + dipyridamole
- Dual antiplatelet (aspirin + clopidogrel) for 21 days after minor stroke/TIA reduces early recurrence (POINT/CHANCE trials)
Anticoagulation
- For AF-associated stroke: Start anticoagulation to prevent recurrence; timing optimized by stroke size (CATALYST meta-analysis, Lancet 2025 [PMID 40570866] - IPD meta-analysis of RCTs guiding early vs delayed anticoagulation)
- Acute anticoagulation with heparin for stroke-in-evolution or cervical artery dissection in selected cases
Statin Therapy
- Start high-intensity statin regardless of baseline LDL (reduces recurrence)
Glucose and Temperature Control
- Treat hyperglycemia (worsens infarct)
- Treat fever aggressively (increases metabolic demand in penumbra)
Hemorrhagic Stroke Management
Intracerebral Hemorrhage
- Reverse anticoagulation immediately (Vitamin K + PCC/FFP for warfarin; specific antidotes for NOACs)
- Blood pressure lowering: Target SBP <140 mmHg (reduces hematoma expansion)
- No role for tPA (contraindicated)
- Surgical evacuation: For cerebellar hemorrhage >3 cm with deterioration, or superficial lobar hemorrhage with mass effect
- ICP management if indicated
Subarachnoid Hemorrhage
- Neurosurgical/interventional referral (clipping vs. coiling of aneurysm)
- Nimodipine 60 mg q4h for 21 days (prevents cerebral vasospasm)
- Avoid hypovolemia; monitor for delayed cerebral ischemia (Days 4-14)
- Watch for hydrocephalus (CSF obstruction by blood)
5. Complications of Stroke
| Complication | Timing | Management |
|---|---|---|
| Cerebral edema / herniation | Days 2-5 | Mannitol, hypertonic saline; hemicraniectomy for malignant MCA infarct |
| Hemorrhagic transformation | 2nd week (earlier with thrombolytics) | Monitor; reverse anticoagulation if needed |
| Seizures | Acute or delayed | AEDs; not routinely prophylactic |
| Aspiration pneumonia | Early | Dysphagia screen; NG tube if needed |
| DVT / PE | Immobility | Compression stockings, early mobilization, prophylactic LMWH |
| Depression | Weeks-months | SSRI (also reduces neurological disability) |
| Vasospasm (SAH) | Days 4-14 | Nimodipine |
6. Secondary Prevention
| Intervention | Indication |
|---|---|
| Antiplatelet (aspirin/clopidogrel) | All non-cardioembolic ischemic stroke/TIA |
| Anticoagulation (DOAC preferred over warfarin) | AF-associated stroke |
| Carotid endarterectomy (CEA) | Symptomatic carotid stenosis >70% |
| Carotid stenting | Symptomatic stenosis; high surgical risk |
| High-intensity statin | All ischemic stroke |
| BP control | All stroke (target <130/80 mmHg) |
| Diabetes management | Diabetic patients |
| Smoking cessation / alcohol reduction | Modifiable risk factors |
| PFO closure | Selected patients with cryptogenic stroke <60 years |
7. NIHSS (National Institutes of Health Stroke Scale)
- Scores 0-42 (higher = worse deficit)
- Assesses: Level of consciousness, gaze, visual fields, facial palsy, arm/leg motor, limb ataxia, sensory, language, dysarthria, extinction/neglect
- Used to guide tPA eligibility and predict outcomes
8. Prognosis
- Ischemic stroke: 30-day mortality ~10-20%; functional outcome depends on stroke size, location, NIHSS, age, comorbidities
- ICH: Higher acute mortality (~40% at 30 days); long-term functional status similar to ischemic stroke survivors
- SAH: ~50% mortality overall; good prognosis for perimesencephalic non-aneurysmal SAH
Recent Evidence (2024-2026)
- Tenecteplase vs alteplase within 4.5h: Systematic review (Neurology, 2024) - tenecteplase is non-inferior and has practical advantages (single bolus)
- Anticoagulation timing post-stroke with AF: CATALYST IPD meta-analysis (Lancet, 2025) - provides individualized timing guidance
- Thrombolysis beyond 4.5h window: Meta-analysis (Stroke, 2025) - benefit in extended window with imaging selection
Sources: Frameworks for Internal Medicine (Wolters Kluwer); Bradley and Daroff's Neurology in Clinical Practice; Plum and Posner's Diagnosis and Treatment of Stupor and Coma; Fuster and Hurst's The Heart, 15th Edition; Adams and Victor's Principles of Neurology, 12th Edition
This is a shared conversation. Sign in to Orris to start your own chat.