Act as a world-class educator and teach me this chapter [chapter name] from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_40__MUSCULOSKELETAL_CARE_MODALITIES.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') # Extract first 5 pages to understand structure for i, page in enumerate(pdf.pages[:5]): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text[:2000]) "
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_40__MUSCULOSKELETAL_CARE_MODALITIES.pdf') as pdf: for i, page in enumerate(pdf.pages[5:]): text = page.extract_text() if text: print(f'--- PAGE {i+6} ---') print(text) "
🦴 Chapter 40: Musculoskeletal Care Modalities
From Absolute Basics to Complete Mastery
🗺️ SIMPLE OVERVIEW (Read This First)
- Casts, splints, braces - hold bones still so they heal
- Traction - uses weights/pulling force to align bones
- External fixation - metal frame outside the body holding bones in place
- Joint replacement - surgery for worn-out hips/knees
- Surgical nursing - care before and after orthopedic operations
"Watch for neurovascular compromise before it becomes permanent damage."
📚 SECTION 1: Key Vocabulary - Your Foundation
| Term | What It Means | Simple Analogy |
|---|---|---|
| External Fixation | Pins go INTO the bone, connected to a frame OUTSIDE the body | Like scaffolding on a building - the scaffold is outside but anchored to the structure |
| Internal Fixation | Screws, plates, rods surgically placed INSIDE the body | Like a metal skeleton inside a broken sculpture |
| Traction | A controlled pulling force to line up bones | Like pulling on a bent straw from both ends to straighten it |
📚 SECTION 2: Casts, Splints, and Braces
What Are They For?
- Keep fracture pieces in the right position while they heal
- Reduce pain and muscle spasm
- Prevent deformity
- Allow healing
Easy way to remember: Think of a cast like a "body brace" for a bone - it holds everything in place so the body can do its repair work.
Patient Teaching: What Does the Nurse Teach?
- ❌ NEVER poke objects inside the cast to scratch itching (causes skin breakdown + infection)
- ❌ NEVER get the cast wet (causes skin maceration - skin gets soggy and breaks down)
- ✅ Elevate the limb to reduce swelling, especially in the first days
- ✅ Report immediately: increasing pain, numbness, tingling, swelling, cool skin, skin color changes, inability to move fingers/toes, or a feeling of tightness
- Skin color (pale? blue?)
- Skin temperature (cool compared to other side?)
- Sensation (numb? tingling?)
- Movement of fingers or toes
- Capillary refill
Example scenario: A patient with a leg cast calls the nurse and says "my toes feel numb and I can't move them well." This is a MEDICAL EMERGENCY - it could be compartment syndrome.
Nursing Assessment: The 6 P's of Neurovascular Check
| P | Stands For | What to Assess |
|---|---|---|
| Pain | Pain | Pain out of proportion to injury? Pain with passive stretch? |
| Paresthesia | Abnormal Sensation | Tingling, numbness distal to cast |
| Pallor | Paleness | Unusual paleness - reduced blood flow |
| Paralysis | Loss of Movement | Can't move fingers/toes? |
| Pulselessness | No Pulse | Absent distal pulse - LATE and CRITICAL sign |
| Poikilothermia | Temperature Change | Limb cooler than the opposite side |
Memory trick: "6 P's - Pain, Paresthesia, Pallor, Paralysis, Pulselessness, Poikilothermia." If you only remember one thing, remember that pain out of proportion + pain with passive stretch = call the doctor NOW.
Nursing Management by Body Region
- Maintain alignment and support
- Assist with safe mobility
- Watch for immobility complications: constipation, pressure injuries, blood clots (DVT)
- Protect skin at edges and bony prominences
- Frequent turning (needs multiple helpers)
- Toileting adaptations - protect cast from moisture/soiling
- Support breathing if the chest is restricted
- Neurovascular checks of both legs
Complications of Casts
- Escalating pain (especially pain with passive stretch - earliest sign)
- Paresthesia (tingling/numbness)
- Tense, firm swelling
- Pallor
- Paralysis
- Pulselessness (LATE - tissue already dying)
- Only with body casts
- The cast compresses the bowel, causing nausea, vomiting, abdominal pain
- Report GI symptoms in any body cast patient
- Caused by pressure points, moisture, or objects poked under the cast
- Prevent with padding, keeping cast dry, repositioning, checking cast edges
- Can happen during cast application if the material gets too hot
- Patient should immediately report any burning sensation during application
📚 SECTION 3: Traction
What Is It and Why Use It?
- Aligns broken bones
- Reduces muscle spasm
- Corrects deformity
- Immobilizes injured areas
4 Principles of Effective Traction
- Traction must be continuous - interrupting it reduces the therapeutic effect
- Weights must hang freely - weights resting on the floor = zero traction force
- Patient must be in correct alignment with the line of pull
- Countertraction must be maintained - usually by the patient's own body weight and proper bed positioning
Exam tip: If a question says "the patient's traction weight is resting on the floor" - the correct nursing action is to reposition the weights so they hang freely.
Types of Traction
| Type | How Applied | Advantages | Risks |
|---|---|---|---|
| Skin Traction | Through skin via boots, straps, bandages | Noninvasive | Skin breakdown, nerve compression |
| Skeletal Traction | Pins/wires directly into bone | Stronger, more precise | Pin site infection, osteomyelitis, pain |
- Used for lower extremity (hip fractures pre-op, muscle spasm)
- Reduces muscle spasm, maintains alignment until surgery
- Nursing: assess extremity, maintain alignment, prevent skin problems
Nursing Management of Traction
- Verify weights are correct and hanging freely at all times
- Ensure ropes and pulleys are unobstructed
- Maintain correct body alignment; no twisting
- Frequent neurovascular checks distal to traction (compare with unaffected limb)
- For skin traction: check skin under/around straps frequently
- Protect bony prominences
- Scheduled turning and pressure redistribution
- Pulmonary hygiene: deep breathing, coughing
- GI: hydration + fiber; bowel regimen if needed
- VTE (blood clot) prevention = BIG priority: prescribed exercises, compression devices, anticoagulation if ordered
📚 SECTION 4: External Fixation
When Is It Used?
- Fractures are severe or open (bone breaking through skin)
- There is substantial swelling
- Repeated wound access is needed (to clean infected tissue)
- Soft tissue needs to heal before internal hardware is placed
Visual: Imagine a scaffolding tower bolted to the outside of a building. The metal pins go through the skin into the bone, and a rigid external frame connects them all together.
Nursing Management
- Monitor for: redness, warmth, swelling, drainage, increasing pain at pin sites
- Perform pin site care per facility protocol (sterile or clean technique as required)
- Signs of infection at a pin site = notify provider
- Continue frequent neurovascular checks distal to the fixator
- Assist with movement while protecting the fixator from impact (it's fragile!)
- Teach safe ambulation and transfer techniques
- How to recognize infection signs at pin sites
- When to seek urgent care
- Device safety and skin protection
📚 SECTION 5: Joint Replacement Care
Total Hip Arthroplasty (THA) vs. Total Knee Arthroplasty (TKA)
🚨 PREVENT HIP DISLOCATION
- The hip adducts (moves toward midline)
- The hip internally rotates
- Use an abduction pillow/device between legs if prescribed
- Maintain neutral alignment - no crossing legs, no turning foot inward
- Teach patient movement precautions (do not bend hip past 90 degrees, no crossing legs, no pivoting on surgical leg)
- Also: prevent VTE and infection (major postoperative risks)
- Pain control and early mobility - early movement supports function and prevents complications
- Protect the surgical site - prevent infection
- Prevent VTE (blood clots - a major risk after knee surgery)
- Restore knee range of motion - per rehabilitation plan
Comparison summary: Hip replacement = dislocation prevention is the distinct priority. Knee replacement = pain control + early mobility + VTE prevention.
📚 SECTION 6: Orthopedic Surgery - Nursing Process Framework
Preoperative Phase
- Does a baseline neurovascular assessment (so you have a comparison point post-op)
- Documents baseline mobility status
- Teaches the patient about:
- Pain control plan
- Deep breathing and coughing exercises
- Mobility plan and physical therapy expectations
- Incision care
- Warning signs to report
Postoperative Phase: Priority Nursing Diagnoses
| Nursing Diagnosis | Key Nursing Actions |
|---|---|
| Acute Pain | Pharmacologic + nonpharmacologic measures; evaluate response |
| Impaired Physical Mobility | Prevent complications; promote safe movement; coordinate rehab |
| Risk for Peripheral Neurovascular Dysfunction | Frequent neurovascular checks; rapid escalation for any changes |
| Risk for Infection | Incision care; aseptic technique; patient teaching; especially critical with fixation devices |
| Risk for VTE | Prevention: exercises, compression devices, anticoagulant therapy if ordered |
Discharge Planning
- Cast/brace or joint precautions and safety at home
- Medication adherence (especially anticoagulants for VTE)
- Clear list of warning signs needing urgent evaluation
🔗 HOW IT ALL CONNECTS
FRACTURE / JOINT PROBLEM
↓
How do we stabilize it?
↙ ↓ ↘
CAST/SPLINT TRACTION EXTERNAL FIXATION → JOINT REPLACEMENT
↓ ↓ ↓ ↓
ALL require the SAME core nursing priorities:
1. Neurovascular checks (6 P's)
2. Prevent skin breakdown
3. Prevent VTE
4. Prevent infection
5. Pain management
6. Patient education
- Compartment syndrome risk → watch the 6 P's
- Infection risk → especially with pins (external fixation) and surgical wounds
- VTE risk → immobility = clots; always prevent
- Dislocation risk → specific to total hip replacement
⚡ FINAL RAPID REVISION SUMMARY
Top 10 Things to Know for Exams:
-
6 P's of neurovascular assessment: Pain, Paresthesia, Pallor, Paralysis, Pulselessness, Poikilothermia - memorize and apply to every modality
-
Compartment syndrome red flag = pain out of proportion + pain with passive stretch - respond immediately
-
Traction rules: Weights hang freely, traction is continuous, correct alignment, maintain countertraction
-
Buck extension = skin traction for lower extremity; used pre-op for hip fractures
-
Skeletal traction vs. Skin traction: Skeletal = stronger but infection risk at pin sites; Skin = noninvasive but skin breakdown risk
-
External fixation pin site care = most important nursing intervention; watch for infection signs
-
Total hip replacement #1 priority = prevent dislocation (abduction pillow, no adduction, no internal rotation, no hip flexion >90°)
-
Total knee replacement #1 priorities = pain control + early mobility + VTE prevention
-
VTE prevention applies to ALL orthopedic modalities - exercises, compression devices, anticoagulation
-
Patient teaching for casts: No objects in cast, keep dry, elevate, report the 6 P's immediately
Quick Reference Card:
| Modality | #1 Specific Risk | #1 Nursing Priority |
|---|---|---|
| Cast/Splint | Compartment syndrome | Neurovascular checks (6 P's) |
| Body cast | Cast syndrome (SMA) | GI monitoring + skin protection |
| Skin traction | Skin breakdown | Skin checks under straps |
| Skeletal traction | Pin site infection | Pin care + neurovascular checks |
| External fixation | Pin site infection | Pin site care |
| Total hip arthroplasty | Hip dislocation | Abduction + movement precautions |
| Total knee arthroplasty | VTE | Early mobility + anticoagulation |
Memory Anchors:
- "Weights on the floor = traction no more" (weights must hang freely)
- "6 P's - Pale, Pulseless, Paralyzed = emergency - call fast"
- "Hip replacement - NO crossing, NO adducting, NO rotating inward"
- "Pin sites: red + warm + draining = infection - tell the doctor"
- "Never scratch inside a cast - break the skin, start an infection"
Explain compartment syndrome
"compartment syndrome" AND "acute" AND "management"
Compartment Syndrome - Complete Explanation
Step 1: Understand the Anatomy First
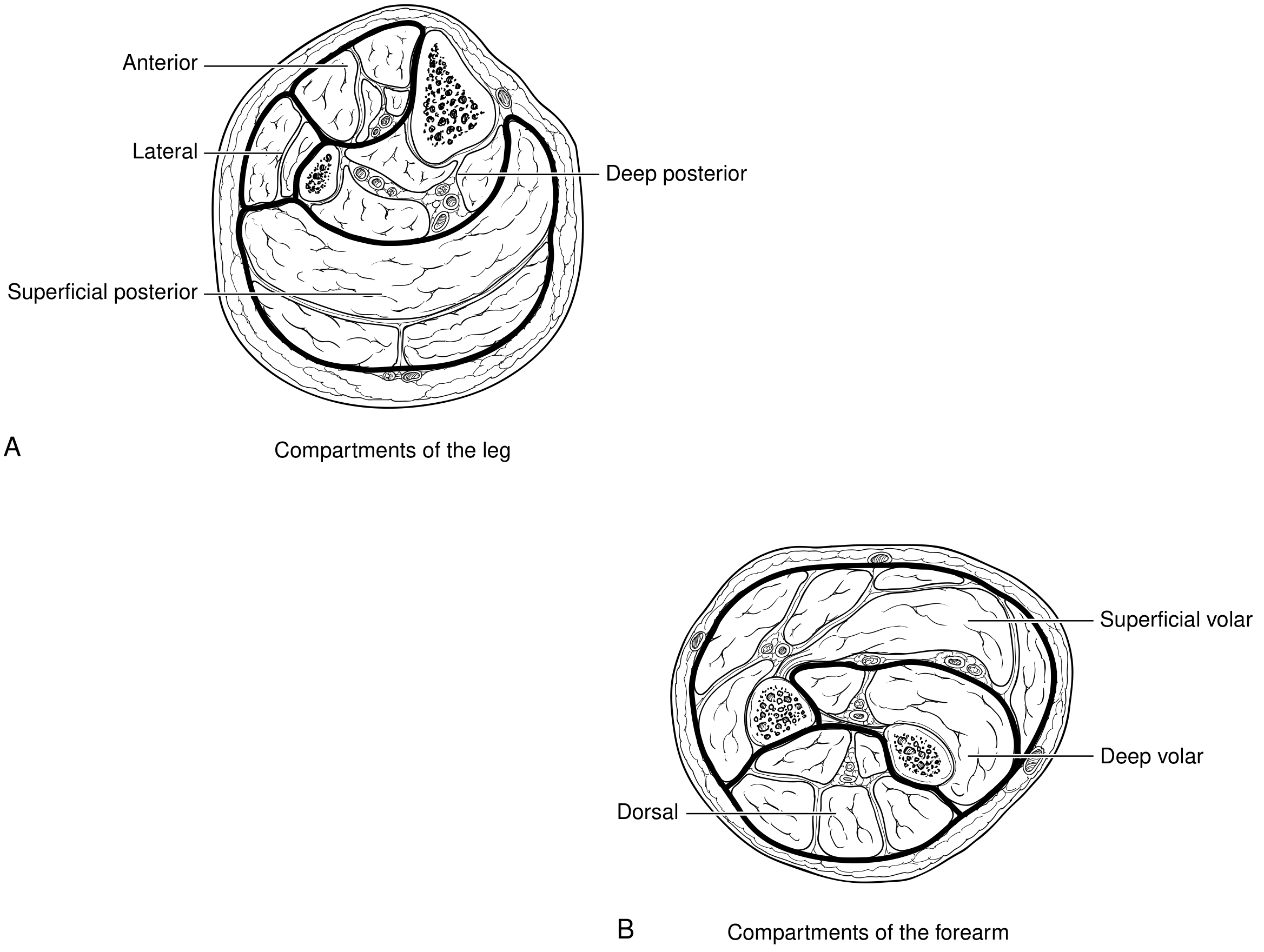
- The leg has 4 compartments: anterior, lateral, deep posterior, superficial posterior
- The forearm has 3: superficial volar, deep volar, dorsal
- Other common sites: the hand, foot, thigh, buttock, and upper arm
Step 2: What IS Compartment Syndrome?
Compartment syndrome = pressure rising inside a fascial compartment to a level that cuts off blood flow to muscles and nerves inside it.
Injury/Swelling → Pressure rises in closed compartment
↓
Capillary perfusion is blocked
↓
Muscle and nerve ischemia (no oxygen)
↓
Cellular damage, more edema released
↓
Even higher pressure (vicious cycle)
↓
Irreversible necrosis (within 6-8 hours if untreated)
Step 3: What Causes It?
- Fractures - 70% (especially tibia, forearm bones)
- Soft tissue crush injuries - 23%
- Bleeding disorders / anticoagulation therapy
- Burns (especially circumferential third-degree burns)
- Reperfusion after arterial ischemia (blood returns after vascular repair, causing massive swelling)
- Tight casts or dressings (external pressure compressing from outside)
- IV fluid extravasation under pressure
Important pitfall: Compartment syndrome can occur even in open fractures (where bone pierces skin). Many clinicians assume an open wound "releases" the pressure - this is wrong. Always maintain a high index of suspicion regardless.
Step 4: Signs and Symptoms - Chronological Order
EARLY Signs (most important - act here):
| Sign | What It Looks Like | Why It Happens |
|---|---|---|
| Pain out of proportion | Pain far worse than the injury should cause | Ischemic nerve fibers |
| Pain with passive stretch | Moving the toes/fingers passively causes severe pain | Stretches ischemic muscle |
| Paresthesia | Tingling, numbness | Nerve ischemia starting |
LATE Signs (tissue already dying):
| Sign | Meaning |
|---|---|
| Pallor | Reduced arterial supply |
| Paralysis | Motor nerve death |
| Pulselessness | EXTREMELY late - major vessel compressed |
Critical teaching point from Bailey and Love's Surgery: "Paralysis, numbness and pallor are late signs and pulselessness is an extremely late sign." By the time the pulse is gone, permanent damage is nearly certain. You must act on the early signs - pain + paresthesia.
Step 5: Diagnosis
- The diagnosis is uncertain
- The patient cannot communicate (sedated, head injury, altered consciousness, intubated)
- You want objective confirmation
- Absolute compartment pressure ≥ 30 mmHg
- OR Delta pressure (diastolic BP - compartment pressure) ≤ 30 mmHg (Bailey & Love)
- OR Delta pressure < 10 mmHg (Current Surgical Therapy) - some sources use this threshold
What NOT to rely on: Elevated CPK (creatine kinase) and myoglobin in the urine are late markers of muscle destruction, not early diagnostic tools. Do not wait for these to rise before acting.
Step 6: Treatment
Immediate Nursing Actions:
- Split/bivalve the cast immediately (if cast is present) - this alone can reduce pressure significantly
- Remove all constrictive dressings down to skin
- Elevate the limb to heart level (do NOT raise above heart - reduces arterial inflow)
- Notify the provider urgently
Definitive Treatment - Fasciotomy:
- Lower leg: requires 4-compartment fasciotomy via medial and lateral incisions
- Forearm: releases the volar (palm-side) and dorsal compartments
- Fasciotomy wounds are left open (not closed) - closing too early causes necrosis
- A vacuum-assisted closure device is applied post-op to manage edema
Timing matters enormously: Fasciotomy within 6-8 hours of onset = good chance of full recovery. After that, irreversible muscle and nerve death accelerates rapidly. Delay = limb loss and possible mortality.
Step 7: Complications if Untreated or Late-Treated
| Complication | Mechanism |
|---|---|
| Volkmann's Ischemic Contracture | Forearm muscles die, replaced by fibrotic scar tissue, leaving a permanently flexed/claw hand |
| Rhabdomyolysis | Dead muscle releases myoglobin into bloodstream |
| Acute Tubular Necrosis / Renal Failure | Myoglobin is toxic to kidney tubules |
| Permanent nerve damage | Paralysis, chronic numbness |
| Limb loss (amputation) | Muscle gangrene when left untreated |
| Death | From systemic effects of massive tissue necrosis |
Step 8: Key Points for Nurses
| Priority | What to Do |
|---|---|
| Assess frequently | Every 1-2 hours post-op or post-injury in high-risk patients |
| Pain is your best early warning | Escalating pain, especially with passive stretch = emergency |
| Don't be falsely reassured by a present pulse | Pulselessness is a VERY late sign - act before this |
| Open fractures are NOT protected | Maintain high suspicion even when skin is broken |
| High-risk window | Prolonged ischemia > 6 hours before repair is the highest-risk scenario |
| Post-fasciotomy care | Wound left open; watch for fluid/electrolyte imbalances, monitor renal function, check urine color for myoglobinuria |
Quick Revision Summary
COMPARTMENT SYNDROME IN 60 SECONDS
WHAT: Pressure in fascial compartment → cuts off perfusion → ischemia → necrosis
CAUSES: Fracture (70%), crush, tight cast, reperfusion injury, burns
DIAGNOSIS: CLINICAL - pain out of proportion + pain with passive stretch
Confirm with compartment pressure ≥30 mmHg or ΔP ≤30 mmHg
EARLY → LATE signs:
Pain → Paresthesia → Pallor → Paralysis → Pulselessness (act EARLY)
TREATMENT:
Immediate → split cast, remove dressings, notify doctor
Definitive → FASCIOTOMY (leave wound open)
COMPLICATIONS if missed:
Volkmann's contracture, rhabdomyolysis, renal failure, limb loss, death
NURSING RULE: Pain out of proportion = call immediately, do not wait
Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_41__MANAGEMENT_OF_PATIENTS_WITH_MUSCULOSKELETAL_DISORDERS.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
📘 Chapter 41: Management of Patients with Musculoskeletal Disorders
From Absolute Basics to Complete Mastery
🗺️ SIMPLE OVERVIEW (Start Here)
| Bucket | What It Covers |
|---|---|
| 1. Low Back Pain | Most common musculoskeletal complaint - causes, management, nursing care |
| 2. Upper Extremity Disorders | Problems of the hand, wrist, shoulder |
| 3. Foot Problems | Common foot conditions requiring nursing care |
| 4. Metabolic Bone Disease | Osteoporosis (the big one) and related disorders |
| 5. Nursing Process | How to apply nursing care to all of the above |
"Assess neurovascular status, manage pain, promote safe mobility, prevent complications, and educate the patient."
🔑 KEY VOCABULARY FIRST
| Term | Definition | Memory Hook |
|---|---|---|
| Bursitis | Inflammation of a bursa (fluid-filled friction-reducing sac) | "Bursa = cushion; -itis = inflamed" |
| Tendonitis | Inflammation of a tendon | "Tendon on fire from overuse" |
| Contracture | Abnormal shortening of muscle or fibrosis of a joint | "The joint got stuck in a contracted position" |
| Radiculopathy | Disease of a spinal nerve root → pain and extreme touch sensitivity | "Radix = root; the root is sick" |
| Sciatica | Inflammation of the sciatic nerve → pain along thigh and leg | Named after the sciatic nerve it affects |
| Osteopenia | Low bone mineral density (precursor to osteoporosis) | "Osteo = bone; penia = poverty" |
| Osteoporosis | Degenerative bone disease - reduced mass, deteriorated matrix, diminished strength | "Porous bone - full of holes" |
| Sequestrum | Dead bone inside an abscess cavity (seen in osteomyelitis) | "Sequestered = isolated; dead bone is isolated" |
| Involucrum | New bone that grows AROUND a sequestrum | "Involucrum = envelope; new bone envelopes the dead bone" |
📚 SECTION 1: Low Back Pain
What Is It?
What Causes It?
- Acute lumbosacral strain (most common) - improper lifting, sudden movement, repetitive stress, poor posture
- Weak abdominal and back muscles - reduce spinal stability
- Intervertebral disc problems - degeneration or displacement that compresses nerve roots
- Unstable lumbosacral ligaments
- Unequal leg length
Example: A nurse who lifts patients incorrectly for years develops lumbar disc degeneration. The disc bulges and presses on the sciatic nerve, causing radiating pain down the leg (sciatica).
Key Manifestations
- Localized or radiating low back pain
- Muscle spasm, stiffness, reduced range of motion
- Pain worsened by movement, lifting, prolonged sitting/standing
- If nerve roots are compressed: radiculopathy (tingling, numbness, weakness)
- Sciatica = sciatic nerve specifically inflamed → pain and tenderness all the way down the thigh and leg
Diagnosis
- Most uncomplicated cases need no imaging - clinical assessment is sufficient
- Imaging (X-ray, MRI) reserved for: persistent severe pain, neurologic deficits, or suspicion of serious cause
- Assessment focuses on: pain character, triggers, activity limitations, occupational risks, neurologic exam
Medical Management
| Treatment | Goal |
|---|---|
| NSAIDs (ibuprofen, naproxen) | Reduce pain AND inflammation |
| Acetaminophen | Reduce pain only (NOT anti-inflammatory) |
| Muscle relaxants | Short-term, for acute muscle spasm |
| Physical therapy | Restore function and prevent recurrence |
| Heat or cold therapy | Symptom relief |
| Early mobilization | Encouraged - prolonged bed rest is AVOIDED |
Important NSAID mechanism: NSAIDs work by blocking prostaglandin formation via COX-1 and COX-2 inhibition. COX-2 selective agents (like celecoxib) inhibit only COX-2, sparing the GI-protective effects of COX-1.
Nursing Management
- Administer pain medications and evaluate effectiveness
- Encourage gradual return to activity (not rest!)
- Teach proper body mechanics and posture - this is health education priority #1
- Reinforce physical therapy adherence
- Promote lifestyle changes: weight loss, smoking cessation, exercise
- Provide emotional support (depression is a comorbidity and barrier to recovery)
📚 SECTION 2: Common Upper Extremity Disorders
2A. Bursitis
2B. Tendonitis
2C. Loose Bodies ("Joint Mice")
Analogy: Like gravel getting into a hinge - the joint can't move smoothly because there's debris inside.
2D. Impingement Syndrome (Shoulder)
Repetitive overhead motion
↓
Tendon/bursa irritation and inflammation
↓
Pain, limited range of motion, muscle spasm, edema
↓
If untreated → disuse atrophy → partial/complete ROTATOR CUFF TEAR
- NSAIDs or intra-articular corticosteroid injections
- Cold or heat therapy (subjective symptom relief)
- Therapeutic exercise program = required for real improvement
- Rest the joint in a position that minimizes stress
- Support the arm on pillows while sleeping
- Gradually resume motion - don't force it
- Avoid working/lifting above shoulder level
- Do NOT push against a "locked" shoulder
- Perform prescribed daily range-of-motion and strengthening exercises
2E. Carpal Tunnel Syndrome (CTS) ⭐ HIGH PRIORITY
- Repetitive hand/wrist movements (typing, assembly work)
- Rheumatoid arthritis
- Diabetes mellitus
- Hypothyroidism / Hyperthyroidism / Acromegaly
- Wrist trauma
- Pain, numbness, paresthesia (tingling) in the thumb, index, and middle fingers (median nerve distribution)
- Night pain - a classic symptom
- Waking with clenched fists - classic
- Weakness of the thumb
- Wrist splints (prevent hyperextension/prolonged flexion)
- Oral corticosteroids (short-term only)
- Intra-articular corticosteroid injections
- NSAIDs
- Acupuncture (with or without electrical stimulation)
- Yoga, laser therapy, ultrasound therapy, diuretics, vitamin B6, prolotherapy
2F. Ganglion Cyst
2G. Dupuytren Disease (Dupuytren Contracture)
Visual: Imagine the palm fascia slowly shrinking like a drying leather strap, pulling the ring and little fingers permanently toward the palm.
Nursing Management: Hand/Wrist Surgery
Preoperative:
- Full neurovascular baseline (color, temperature, capillary refill, sensation, movement, pulses)
- Assess pain, range of motion, strength, and ability to do ADLs
- Patient education: expected procedure, postoperative immobilization
- Address anxiety about loss of hand function and work limitations
Postoperative Priorities (in order):
| Priority | Action |
|---|---|
| #1 Neurovascular monitoring | Check color, temp, capillary refill, sensation, movement of fingers frequently |
| #2 Pain management | Analgesics + elevate hand above heart level |
| #3 Edema control | Elevate above heart especially first 24-48 hours; gentle finger movement if permitted |
| #4 Immobilization protection | Maintain splint/cast integrity; ensure not too tight |
| #5 Wound care | Monitor for bleeding, drainage, infection signs (redness, warmth, swelling, fever) |
| #6 Rehab | Early controlled motion as prescribed; OT/PT collaboration |
- Increasing pain unrelieved by medication
- Numbness or tingling
- Pallor or cyanosis
- Excessive swelling
Discharge Teaching:
- Proper hand elevation technique
- Splint/cast care at home
- Wound care and hygiene
- Activity restrictions: no heavy lifting or repetitive motion until cleared
- Warning signs to report: pain, swelling, numbness, color changes, fever, drainage
- Stress that full recovery depends on therapy compliance
📚 SECTION 3: Common Foot Problems
| Condition | What It Is | Key Feature |
|---|---|---|
| Callus | Thickened skin from friction/pressure | On weight-bearing areas; protective but can become painful |
| Corn | Small thickened skin over bony prominence | Has a central core that presses on tissue - painful |
| Hallux Valgus | Lateral deviation of great toe + bunion | "Bunion" = enlarged first metatarsal head; pain, difficulty with shoes |
| Hammer Toe | PIP joint flexion deformity (claw-like) | Usually 2nd-4th toe; from muscle imbalance or ill-fitting shoes |
| Ingrown Toenail | Nail edge grows into surrounding tissue | Great toe most common; can become infected |
| Morton Neuroma | Thickened nerve tissue between 3rd & 4th toes | "Walking on a pebble" sensation; burning, numbness, tingling |
| Pes Cavus | Abnormally HIGH arch | Uneven weight distribution → pain, instability, calluses |
| Pes Planus | Flat foot (LOW/absent arch) | Sole touches ground entirely; foot fatigue, altered gait |
| Plantar Fasciitis | Inflammation of plantar fascia (heel to forefoot) | Sharp heel pain first thing in the morning - classic symptom |
Memory trick for arches: "Cavus = Cave = high arch." "Planus = Plane = flat."
Nursing Management: Foot Surgery
Preoperative:
- Assess pain, deformity, skin integrity, circulation, sensation, gait/balance
- Review comorbidities that affect healing: diabetes and peripheral vascular disease are critical
- Neurovascular baseline documentation
- Patient education: immobilization, weight-bearing restrictions, assistive devices
- Fall prevention education - altered mobility post-op creates fall risk
Postoperative Priorities:
| Priority | Foot-Specific Actions |
|---|---|
| Neurovascular monitoring | Assess color, temp, capillary refill, sensation, toe movement, pulses |
| Pain + Edema | Elevate foot above heart level; cold therapy if prescribed |
| Weight bearing | Reinforce non-weight-bearing or limited weight-bearing restrictions |
| Ambulation safety | Teach correct use of crutches/walker; fall prevention measures |
| Wound care | Especially important in diabetic patients (impaired healing) |
- Proper footwear
- Ongoing foot care and inspection
- Foot protection strategies
📚 SECTION 4: Metabolic Bone Disorders
OSTEOPOROSIS ⭐ MAJOR TOPIC
What Is It?
- Reduced bone mass
- Deterioration of bone matrix (microarchitecture)
- Diminished architectural strength
Pathophysiology
Normal: Resorption = Formation → Stable bone density
Osteoporosis: Resorption > Formation → Bone mass DECREASES
- Estrogen deficiency (postmenopause) → accelerates osteoclastic (bone-destroying) activity
- Aging → decreased calcium absorption, reduced vitamin D synthesis
- Trabecular bone (spine, hip, wrist) is most affected because it has higher metabolic activity
Risk Factors
- Advanced age
- Female sex
- Family history
- Small body frame
- White or Asian ethnicity
- Inadequate calcium and vitamin D intake
- Physical inactivity
- Smoking
- Excessive alcohol consumption
- Long-term corticosteroid use
- Endocrine disorders, malabsorption syndromes
Clinical Manifestations
- Back pain (from vertebral fractures)
- Loss of height (vertebrae compress)
- Kyphosis - "Dowager's hump" (thoracic spine curvature from multiple vertebral compression fractures)
- Fractures from minimal trauma: vertebral compression, hip, wrist (Colles' fracture)
Diagnosis
- Dual-Energy X-ray Absorptiometry (DEXA) is the most commonly used test
- Measures bone mineral density (BMD)
- Predicts fracture risk, particularly at the hip and spine
- Other methods: quantitative CT, quantitative ultrasound
Prevention (Prevention > Treatment)
| Strategy | Why It Helps |
|---|---|
| Adequate calcium + vitamin D | Supports bone mineralization |
| Weight-bearing exercise | Stimulates bone formation, slows resorption |
| Muscle-strengthening exercise | Improves stability, reduces falls |
| Avoid smoking | Smoking accelerates bone loss |
| Limit alcohol | Alcohol accelerates bone loss |
| Fall prevention | Reduces fracture events |
| Early risk identification | Start prevention before fractures occur |
Medical Management
- Calcium + Vitamin D supplementation (foundational)
- Medications that inhibit bone resorption (bisphosphonates like alendronate) OR enhance bone formation
- Exercise programs: strength, balance, posture focused
- Treatment is long-term - requires adherence and monitoring
Gerontologic Considerations
- Bones are already weakened by years of negative bone balance
- Fall risk is higher due to balance problems, muscle weakness, medications
- Chronic pain
- Reduced mobility
- Loss of independence
- Increased morbidity and mortality (hip fractures carry serious 1-year mortality risk)
Nursing Process: Patient with Osteoporotic Vertebral Fracture
A. Nursing Assessment:
- Pain intensity, location, and characteristics
- Mobility and ability to perform ADLs
- Posture, height loss, and spinal deformity
- Immobility complications (skin breakdown, constipation, DVT)
B. Nursing Diagnoses:
- Acute pain
- Impaired physical mobility
- Risk for falls
- Imbalanced nutrition: less than body requirements
- Risk for injury
C. Nursing Interventions:
| Diagnosis | Interventions |
|---|---|
| Acute pain | Administer prescribed analgesics; supportive positioning; comfort measures |
| Impaired mobility | Encourage safe movement; gradual activity; physical therapy |
| Risk for falls | Safety measures; home safety education |
| Nutrition | Dietary teaching: calcium-rich foods, vitamin D |
| Risk for injury | Medication adherence; fall prevention |
D. Evaluation Criteria:
- Decreased pain levels
- Improved or maintained mobility
- No additional fractures
- Patient demonstrates understanding of osteoporosis management
Other Metabolic Bone Disorders (Brief Overview)
| Disorder | Key Feature |
|---|---|
| Osteomalacia | Soft bones due to vitamin D deficiency - bone matrix forms but doesn't mineralize |
| Paget Disease | Excessive disorganized bone remodeling → thick, weak, deformed bones |
| Septic (Infectious) Arthritis | Joint infection - requires urgent treatment to prevent joint destruction |
| Osteomyelitis | Bone infection; involves sequestrum (dead bone) and involucrum (new bone around it) |
| Bone Tumors | Primary (starts in bone) or metastatic (spreads from elsewhere); nursing focuses on pain and monitoring |
🔗 HOW ALL SECTIONS CONNECT
MUSCULOSKELETAL DISORDERS
│
┌─────┴──────────────────────────────┐
│ │
STRUCTURAL METABOLIC
(Mechanical/Overuse) (Bone Disease)
│ │
Low Back Pain Osteoporosis
Upper Extremity Disorders Osteomalacia
Foot Problems Paget Disease
Bone Infections/Tumors
│ │
└──────────────┬─────────────────────┘
│
SAME NURSING PRIORITIES APPLY:
1. Neurovascular assessment
2. Pain management
3. Fall/injury prevention
4. Patient education
5. Promote mobility and independence
- All conditions cause pain → nurse manages pain and evaluates response
- All conditions affect mobility → nurse promotes safe movement and prevents immobility complications
- All conditions have education needs → body mechanics, footwear, calcium intake, exercise, warning signs
- All surgical conditions share neurovascular monitoring as the #1 postoperative priority
⚡ FINAL RAPID REVISION SUMMARY
Top 12 Exam Points:
-
Low back pain = mostly mechanical (strain); prolonged bed rest is AVOIDED; NSAIDs first-line; teach body mechanics
-
NSAIDs mechanism = block prostaglandin formation via COX-1/COX-2 inhibition; acetaminophen = analgesic only, NOT anti-inflammatory
-
Impingement syndrome = rotator cuff pinching; avoid overhead activities; can progress to rotator cuff tear if untreated
-
Carpal tunnel syndrome = median nerve compression; median nerve distribution = thumb, index, middle fingers; night pain is classic; wrist splints are first-line; DEXA NOT used here
-
CTS ineffective treatments = yoga, laser therapy, ultrasound, vitamin B6, diuretics (these are commonly tested as distractors)
-
Dupuytren contracture = ring and little fingers pulled into flexion by contracted palmar fascia
-
Plantar fasciitis = heel pain worst with FIRST STEPS in the morning
-
Morton neuroma = "walking on a pebble" sensation between 3rd and 4th toes
-
Osteoporosis = often asymptomatic until fracture; DEXA scan is primary diagnostic tool; estrogen deficiency = major driver
-
Osteoporosis signs = back pain, loss of height, kyphosis (dowager's hump)
-
Postoperative priority for ALL orthopedic surgeries = neurovascular assessment first (color, temperature, capillary refill, sensation, movement, pulse)
-
Sequestrum vs Involucrum (osteomyelitis): Sequestrum = dead bone; Involucrum = new bone growing around the dead bone
Quick-Fire Disease Summary Table:
| Condition | Key Defining Feature | Primary Nursing Action |
|---|---|---|
| Low back pain | Pain worse with movement; may radiate (sciatica) | Teach body mechanics; avoid bed rest |
| Bursitis | Inflamed bursa → pain at joint | Rest, NSAIDs, ice |
| Tendonitis | Inflamed tendon from overuse | Rest, NSAIDs, rehab |
| Carpal tunnel | Median nerve compression; night pain | Wrist splint; avoid repetitive motion |
| Dupuytren | Ring + little finger fixed in flexion | Post-op neurovascular checks |
| Hallux valgus | Great toe deviates laterally (bunion) | Proper footwear; post-op weight-bearing restrictions |
| Plantar fasciitis | Heel pain first steps in AM | Stretching, supportive footwear |
| Morton neuroma | "Pebble" sensation 3rd-4th toes | Wider shoes, orthotics, possible injection |
| Osteoporosis | Porous bone → fractures; DEXA for diagnosis | Calcium + Vit D; fall prevention; exercise |
| Osteomyelitis | Bone infection with sequestrum/involucrum | IV antibiotics; wound care; neuro checks |
Memory Anchors:
- "Carpal tunnel = MEDIAN nerve = thumb, index, MIDDLE = wakes you at NIGHT"
- "Dupuytren = ring and LITTLE fingers CURL IN"
- "Plantar fasciitis = FIRST STEPS hurt most"
- "Osteoporosis = SILENT until BROKEN"
- "DEXA = the ONLY way to measure bone density"
- "Post-op #1 = Neurovascular check ALWAYS"
- "Bed rest is BAD for back pain - keep MOVING"
“Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_41__MANAGEMENT_OF_PATIENTS_WITH_MUSCULOSKELETAL_DISORDERS_PART_2.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
📘 Chapter 41 Part 2: Management of Patients with Musculoskeletal Disorders
From Absolute Basics to Complete Mastery
🗺️ SIMPLE OVERVIEW (Read This First)
| Section | Topic | Core Problem |
|---|---|---|
| 1 | Osteomalacia | Bones form but don't harden - vitamin D deficiency |
| 2 | Paget Disease | Bones remodel too fast and become disorganized, enlarged, and brittle |
| 3 | Musculoskeletal Infections (Osteomyelitis + Septic Arthritis) | Bacteria invade bone or joints - causes destruction and necrosis |
| 4 | Bone Tumors | Abnormal cell growth weakens bone - primary or spread from elsewhere |
"Manage pain, prevent complications (especially fractures and functional loss), control infection when present, and educate the patient on long-term adherence."
📚 SECTION 1: Osteomalacia
What Is It - In Plain English?
- The protein framework (osteoid - like the scaffolding)
- The mineral coating (calcium + phosphate - the concrete that hardens the scaffold)
Key distinction to know for exams:
- Osteoporosis = bone mass is LOST (scaffold itself is reduced)
- Osteomalacia = bone mass is present but NOT MINERALIZED (scaffold exists but stays soft)
What Causes It?
- Low phosphate levels
- Malabsorption syndromes (Crohn's, celiac disease)
- Poor dietary intake
- Reduced sun exposure (skin makes vitamin D from sunlight)
Who Is at Highest Risk?
- Institutionalized patients (nursing home residents - little sunlight, limited diet)
- Homebound older adults
- Those with reduced renal function (kidneys activate vitamin D)
Warning: Bone pain and weakness in older adults is often dismissed as "just aging" - this delays diagnosis. Always consider osteomalacia.
Clinical Manifestations
- Diffuse bone pain and tenderness - especially hips, pelvis, lower back
- Proximal muscle weakness - difficulty climbing stairs, rising from a chair
- Difficulty walking
- Increased fracture risk with minimal trauma
- Microfractures (tiny stress fractures throughout the soft bones)
Diagnosis
| Test | What It Shows |
|---|---|
| Serum vitamin D | LOW |
| Serum calcium | Low or normal |
| Serum phosphate | LOW |
| X-ray | Decreased bone density, characteristic demineralization changes |
| Clinical picture | Bone pain + muscle weakness + lab findings together = diagnosis |
Medical Management
- Vitamin D supplementation (oral or parenteral depending on absorption ability)
- Calcium supplementation
- Treat the underlying cause:
- Manage malabsorption syndromes
- Improve nutrition
- Safe sun exposure when appropriate
- Long-term follow-up to monitor response and prevent recurrence
Good news: With adequate treatment, bone pain and weakness usually improve and fracture risk decreases.
📚 SECTION 2: Paget Disease of the Bone
What Is It - In Plain English?
Analogy: Imagine a construction crew demolishing and rebuilding a wall simultaneously, working frantically and without any blueprint. The wall gets rebuilt quickly but it's thick, misshapen, full of structural flaws, and will crack under stress.
Three Phases of Paget Disease
| Phase | What Happens | Key Player |
|---|---|---|
| 1. Osteolytic Phase | Excessive bone DESTRUCTION | Overactive osteoclasts eat bone rapidly |
| 2. Mixed Phase | Simultaneous destruction AND rebuilding | Both osteoclasts and osteoblasts working at once |
| 3. Osteoblastic (Sclerotic) Phase | New bone FORMS but it's disorganized, enlarged, and weak | Osteoblasts lay down chaotic bone |
- Dense but brittle
- Poorly organized
- Highly vascular (lots of blood vessels inside)
What Bones Are Affected?
- Pelvis (most common)
- Spine
- Skull
- Femur
- Tibia
Clinical Manifestations
| Symptom | Cause |
|---|---|
| Bone pain (deep, aching, persistent) | Most common symptom; caused by bone remodeling and nerve compression |
| Bowing of long bones | Structural weakness from disorganized bone |
| Enlarging skull (increasing hat size) | Skull bones grow abnormally |
| Hearing loss | Skull changes compress auditory nerve |
| Headaches + Radicular pain | Nerve compression by enlarged, deformed bone |
| Warmth over affected bones | Bone is highly vascular - extra blood flow = warm skin |
| Pathologic fractures | Brittle bone breaks under normal stress |
| Secondary osteoarthritis | Deformed bones stress adjacent joints |
Many patients are asymptomatic early - disease is often found incidentally during testing for another condition.
Key Diagnostic Finding
- ALP reflects bone turnover activity
- In Paget disease, bone is remodeling at an extreme rate → ALP spikes
- Serum calcium and phosphate are usually normal (contrast with osteomalacia)
- X-ray: bone enlargement, deformity, areas of lysis AND sclerosis side by side
- Bone scan: identifies which bones are affected and how active the disease is
Medical Management
| Treatment | Purpose |
|---|---|
| Bisphosphonates (first-line) | Inhibit osteoclastic activity → slow down the runaway bone destruction → normalize bone turnover |
| Calcitonin (selected cases) | Alternative to bisphosphonates - inhibits osteoclasts |
| Analgesics | Pain control |
| Orthopedic surgery | For fractures, severe deformities, or joint degeneration |
- Relieve bone pain
- Slow disease progression
- Prevent complications (fractures, deformity, nerve compression)
Gerontologic Considerations
- Paget disease typically appears after age 50
- Symptoms may be attributed to normal aging → delayed diagnosis
- Fall prevention + pain management + maintaining functional independence are the nursing care pillars
📚 SECTION 3: Musculoskeletal Infections
PART A: OSTEOMYELITIS (Bone Infection)
What Is It?
How Do Bacteria Get Into Bone?
| Route | Example |
|---|---|
| Hematogenous spread | Bacteria from a distant infection (UTI, skin infection) travel through the bloodstream to bone |
| Direct invasion | Open fracture, surgery, or penetrating trauma drives bacteria directly into bone |
| Contiguous spread | Nearby soft tissue infection (diabetic foot ulcer) slowly spreads into underlying bone |
The Pathophysiology Cascade (Step by Step)
Bacteria enter bone
↓
Inflammatory response triggered
↓
Intramedullary pressure rises
↓
Blood flow to bone is reduced
↓
Bone ischemia and necrosis occur
↓
Dead bone separates → SEQUESTRUM forms
↓
Body attempts repair → new bone grows around dead bone → INVOLUCRUM forms
↓
Infection becomes chronic if sequestrum persists
(dead bone is like a "hiding place" for bacteria - antibiotics can't reach it)
Why is chronic osteomyelitis so hard to treat? Because the sequestrum (dead bone) acts as a reservoir for bacteria that antibiotics cannot penetrate. Surgical removal is often necessary.
Clinical Manifestations
- Localized bone pain and tenderness
- Swelling, redness, warmth over the area
- Limited movement of the affected limb
- Fever, chills, malaise (systemic infection signs)
- Persistent or intermittent pain
- Sinus tracts - tunnels that form from the infected bone to the skin surface, draining pus
- Delayed wound healing
Diagnosis
| Test | Purpose |
|---|---|
| WBC + inflammatory markers | Elevated (confirms infection/inflammation) |
| Blood cultures | Identify the causative organism |
| Bone biopsy + culture | DEFINITIVE diagnosis |
| X-ray | Shows bone destruction (but delayed - may be normal early) |
| MRI/CT | Better for early infection and extent of involvement |
Prevention
- Prompt treatment of open fractures and soft-tissue infections
- Strict aseptic technique during surgical procedures
- Early identification and treatment of bloodstream infections
- Careful wound management in diabetes/vascular disease patients
- Patient education on wound care and early infection signs
Medical Management
| Treatment | Details |
|---|---|
| Long-term IV antibiotics | Mainstay of treatment; guided by culture and sensitivity |
| Surgical debridement | Remove necrotic bone and tissue |
| Abscess drainage | Drain any pus collections |
| Sequestrum removal | Remove the dead bone (essential in chronic cases) |
| Immobilization | Reduces pain and promotes healing |
| Nutritional support | Adequate protein/calories are essential for tissue repair |
Nursing Process: Patient with Osteomyelitis
- Pain characteristics and severity
- Temperature and systemic infection signs
- Inspect affected area: swelling, redness, drainage
- Mobility and functional limitations
- Lab and culture results
- Acute or chronic pain
- Impaired physical mobility
- Risk for infection spread
- Impaired skin integrity
- Imbalanced nutrition: less than body requirements
| Problem | Actions |
|---|---|
| Infection control | Administer antibiotics on schedule; monitor therapeutic effects and side effects |
| Pain | Analgesics; position affected limb comfortably |
| Mobility | Encourage appropriate activity while protecting the area |
| Wound care | Dressing changes with strict aseptic technique |
| Education | Complete the full antibiotic course; wound care at home; signs of recurrence |
- Pain reduction or absence
- Resolution of infection signs
- Improved mobility and function
- Patient understands self-care and treatment
PART B: SEPTIC (INFECTIOUS) ARTHRITIS
What Is It?
Why is it an emergency? Bacteria inside a joint space rapidly destroy cartilage. Cartilage has NO blood supply and CANNOT regenerate. Once destroyed, the joint is permanently damaged.
Commonly Affected Joints (in order):
- Knee (most common)
- Hip
- Shoulder
- Wrist
Clinical Manifestations
- Sudden onset of severe joint pain - this is dramatic and rapid
- Swelling, warmth, erythema over the joint
- Marked limitation of motion
- Joint is held in a position of comfort (usually slight flexion - reduces capsule tension)
- Fever and chills
- Malaise and fatigue
Nursing alert: Older adults, immunocompromised patients, and patients with pre-existing joint disease may have less obvious fever - do not be falsely reassured by a low-grade or absent fever.
Diagnosis
- Fluid is purulent (pus-like)
- Elevated WBCs in the fluid
- Causative organism identified on culture
- Blood WBC + inflammatory markers (elevated)
- Blood cultures (may identify organism)
- Imaging (to evaluate joint and rule out other causes)
Medical Management
| Treatment | Purpose |
|---|---|
| Immediate IV antibiotics | Start NOW - do not wait for cultures to begin treatment |
| Joint drainage | Remove infected synovial fluid - essential to stop destruction |
| Needle aspiration | Simple, bedside drainage |
| Arthroscopic drainage | More thorough visualization and washout |
| Surgical drainage | For severe or complicated cases |
| Short-term immobilization | Reduce pain during acute phase |
| Gradual rehabilitation | Begin range-of-motion once infection is controlled - prevent stiffness |
Nursing Management
| Priority | Actions |
|---|---|
| Treat as medical emergency | Report suspected septic arthritis IMMEDIATELY |
| Pain management | Analgesics; position joint for comfort |
| Infection control | IV antibiotics exactly as prescribed; aseptic technique during aspiration |
| Joint protection | Immobilize during acute phase |
| Recovery mobility | Gradual, prescribed ROM exercises with PT collaboration |
| Monitoring | Temperature; joint pain, swelling, mobility; lab results |
| Education | Complete antibiotic course; early signs of recurrence; follow-up importance |
📚 SECTION 4: Bone Tumors
Types of Bone Tumors
BONE TUMORS
│
├── PRIMARY (originate in bone)
│ ├── Benign (non-cancerous)
│ └── Malignant (cancerous)
│ ├── Osteosarcoma
│ ├── Chondrosarcoma
│ └── Ewing Sarcoma
│
└── METASTATIC (spread to bone from elsewhere) ← MORE COMMON
└── Source: Breast, Prostate, Lung, Kidney, Thyroid
Primary Malignant Bone Tumors
| Tumor | Origin | Who Gets It | Key Feature |
|---|---|---|---|
| Osteosarcoma | Bone-forming cells | Children and adolescents (most common age group) | Most common primary malignant bone tumor |
| Chondrosarcoma | Cartilage-forming cells | Adults | Slower growing than osteosarcoma |
| Ewing Sarcoma | Uncertain origin | Children and young adults | Highly aggressive |
Metastatic Bone Tumors
- Breast
- Prostate
- Lung
- Kidney
- Thyroid
- Spine (most common)
- Pelvis
- Femur
- Ribs
Pathophysiology: How Do Tumors Damage Bone?
Tumor cells grow in bone
↓
Normal bone remodeling disrupted
↓
Bone structure weakened
↓
Blood supply interfered with
↓
Malignant tumors may:
• Destroy bone (osteolytic activity)
• Cause PATHOLOGIC FRACTURES (fracture from minimal or no trauma)
• Invade surrounding tissue
• Metastasize further
- Increase bone resorption (eat the bone away)
- Replace normal bone marrow with tumor cells → causes anemia
Clinical Manifestations
| Symptom | Details |
|---|---|
| Pain (most common) | Deep, aching, persistent; worse at night or with activity |
| Swelling/palpable mass | Over the affected bone |
| Pathologic fractures | Fracture with minimal or no trauma - classic |
| Decreased ROM / functional impairment | Tumor interferes with joint or movement |
| Fatigue, weight loss, anemia | Systemic effects (especially metastatic disease) |
| Neurologic deficits | If tumor compresses nerve or spinal cord |
Diagnosis
| Test | Purpose |
|---|---|
| X-ray | Identifies bone destruction, lesions, deformities (first-line imaging) |
| Advanced imaging (CT/MRI) | Defines tumor size, location, soft tissue involvement |
| Bone biopsy | DEFINITIVE diagnosis - determines tumor type and malignancy |
| Lab work | May show anemia; specific tumor markers depending on type |
| History | History of known malignancy = strong suggestion of metastatic disease |
Medical Management
| Modality | When Used |
|---|---|
| Surgery - limb-sparing | Preferred when feasible - removes tumor while saving the limb |
| Amputation | Required in advanced disease when limb cannot be saved |
| Radiation therapy | Tumor control, pain relief, inoperable tumors |
| Chemotherapy | Primarily for osteosarcoma and Ewing sarcoma (given pre- and post-surgery) |
| Palliative management | Advanced/metastatic disease - focus on pain relief, mobility, quality of life |
Nursing Management
- Frequent, thorough pain assessment
- Administer prescribed analgesics (bone tumor pain is often severe)
- Nonpharmacologic comfort measures
- Protect affected bone from stress - at risk for pathologic fracture
- Fall prevention strategies (a fall = potential fracture at tumor site)
- Assist with ambulation and transfers
- Pathologic fractures
- Neurologic compromise (cord compression = emergency)
- Infection
- Monitor labs and imaging results
- Bone cancer diagnosis is deeply distressing
- Fear, anxiety, body image concerns (especially if amputation involved)
- Encourage expression of feelings
- Involve family and support systems
- This is not optional - it is a core nursing intervention
- Explain diagnostic tests and treatment plan
- Reinforce therapy adherence
- Teach signs/symptoms requiring immediate medical attention (sudden pain increase, neurologic changes, fracture)
🔗 HOW ALL SECTIONS CONNECT
BONE/JOINT DISEASE MECHANISMS
│
┌───────┼──────────────────┐
│ │ │
METABOLIC INFECTION TUMORS
│ │ │
Soft/weak Necrosis & Destruction &
bones destruction pathologic fractures
│ │ │
└───────┴──────────────────┘
│
SAME NURSING PRIORITIES:
1. Pain management
2. Protect bone from fracture
3. Prevent/control infection
4. Promote mobility safely
5. Psychosocial support
6. Patient education + adherence
| Link | Connection |
|---|---|
| Osteomalacia → Osteoporosis | Both weaken bone and increase fracture risk; different mechanisms |
| Osteomyelitis → Paget | Both involve abnormal bone remodeling; Paget is non-infectious |
| Osteomyelitis → Septic arthritis | Both are bone/joint infections; both emergencies; both require IV antibiotics + drainage/debridement |
| Septic arthritis → Bone tumors | Both cause pain, swelling, limited motion; tumor pain is persistent and worse at night |
| All conditions | Pathologic fracture risk is a common thread - always protect the bone |
⚡ FINAL RAPID REVISION SUMMARY
Top 12 Exam Points:
-
Osteomalacia vs Osteoporosis: Osteomalacia = bone matrix forms but DOESN'T mineralize (soft). Osteoporosis = bone mass is LOST. Both cause fractures.
-
Osteomalacia cause = vitamin D deficiency → low calcium absorption → soft, unmineralized bones. Treat with vitamin D + calcium.
-
Paget disease = 3 phases: osteolytic → mixed → osteoblastic. Result: dense BUT brittle, disorganized bone.
-
Paget key lab finding = markedly elevated serum alkaline phosphatase (ALP). Calcium/phosphate usually normal.
-
Paget treatment = bisphosphonates (inhibit osteoclasts, normalize bone turnover).
-
Osteomyelitis = sequestrum (dead bone) + involucrum (new bone around it). Chronic cases are hard to treat because antibiotics can't penetrate the sequestrum.
-
Osteomyelitis treatment = long-term IV antibiotics + surgical debridement + removal of sequestrum.
-
Septic arthritis = MEDICAL EMERGENCY. Synovial fluid analysis = KEY diagnostic test (purulent fluid + high WBC). Start IV antibiotics IMMEDIATELY.
-
Most common joint for septic arthritis = knee.
-
Metastatic bone tumors > primary bone tumors in frequency. Sources: Breast, Prostate, Lung, Kidney, Thyroid.
-
Bone tumor types by age: Osteosarcoma = children/adolescents; Chondrosarcoma = adults; Ewing sarcoma = children/young adults + highly aggressive.
-
Pathologic fracture = fracture occurring with minimal or no trauma → occurs in osteoporosis, Paget disease, osteomyelitis, and bone tumors - protect bone in all cases.
Quick-Fire Comparison Table:
| Disease | Key Pathology | Key Lab | Key Treatment |
|---|---|---|---|
| Osteomalacia | Unmineralized osteoid | Low vitamin D, low phosphate | Vitamin D + calcium supplementation |
| Paget disease | Disorganized bone remodeling | High ALP | Bisphosphonates |
| Osteomyelitis | Bone infection + necrosis (sequestrum) | High WBC; bone biopsy = definitive | Long-term IV antibiotics + surgery |
| Septic arthritis | Joint infection → cartilage destruction | Purulent synovial fluid | Emergency: IV antibiotics + joint drainage |
| Bone tumors | Abnormal cell growth destroying bone | Bone biopsy = definitive | Surgery ± radiation ± chemotherapy |
Memory Anchors:
- "Osteomalacia = Soft scaffold - the walls never hardened"
- "Paget = Frantic chaotic construction - fast but faulty"
- "ALP up high = Paget nearby" (elevated ALP + normal calcium = Paget)
- "Sequestrum = dead; Involucrum = new shell around it" - the dead bone becomes entombed
- "Septic arthritis = EMERGENCY - joint cartilage won't grow back"
- "Metastatic > primary" in bone tumors
- "Bone tumor pain = deep, aching, WORST AT NIGHT"
- "Pathologic fracture = bone broke without good reason = suspect tumor/infection/metabolic disease"
The Final Big Picture - All of Chapter 41 Parts 1 and 2 Together:
MUSCULOSKELETAL DISORDERS
│
┌────┴────────────────────┐
MECHANICAL DISEASE-BASED
│ │
Low back pain ┌────┴────────────────────────┐
Upper extremity │ │ │
Foot problems METABOLIC INFECTION TUMOR
│ │ │
Osteoporosis Osteomyelitis Primary tumors
Osteomalacia Septic arthritis Metastatic
Paget disease
ALL REQUIRE: Pain control | Mobility support | Fall prevention | Patient education
Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Also, synthesis additional information from other sources pertinent to this chapter that are important for me to know as a nurse. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_42__MANAGEMENT_OF_PATIENTS_WITH_MUSCULOSKELETAL_TRAUMA_.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
- Fracture classification system (open vs. closed, types, Gustilo-Anderson open fracture grading)
- Bone healing stages (5-stage process + what delays healing)
- Fat Embolism Syndrome in full detail - onset timing, classic triad, petechiae, prevention
- Full complications list from both early injury and prolonged immobility
- Damage Control Orthopedics - why polytrauma patients aren't fixed all at once
- Complete amputation section - indications, levels, stump care, figure-8 wrapping, phantom limb pain vs. sensations, positioning to prevent contractures
- Common dislocation sites with specific neurovascular risks per joint (axillary nerve in shoulder, sciatic nerve in hip, popliteal artery in knee)
Generate a quick reference PDF on compartment syndrome recognition and emergency response
ls -la /home/daytona/workspace/ && mkdir -p /home/daytona/workspace/compartment-syndrome-qr
~/compartment-syndrome-qr/generate_pdf.py
from reportlab.lib.pagesizes import letter
from reportlab.lib import colors
from reportlab.lib.units import inch
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import PageTemplate, Frame
from reportlab.lib.colors import HexColor
OUTPUT = "/home/daytona/workspace/compartment-syndrome-qr/Compartment_Syndrome_Quick_Reference.pdf"
# ── Colour palette ────────────────────────────────────────────────────────────
RED = HexColor("#C0392B")
RED_LITE = HexColor("#FADBD8")
ORANGE = HexColor("#E67E22")
ORG_LITE = HexColor("#FDEBD0")
NAVY = HexColor("#1A3A5C")
NAVY_LT = HexColor("#D6E4F0")
GREEN = HexColor("#1E8449")
GRN_LITE = HexColor("#D5F5E3")
GRAY = HexColor("#F2F3F4")
DARK_GRY = HexColor("#5D6D7E")
WHITE = colors.white
BLACK = colors.black
YELLOW = HexColor("#F9E79F")
YEL_BRD = HexColor("#D4AC0D")
doc = SimpleDocTemplate(
OUTPUT,
pagesize=letter,
rightMargin=0.55 * inch,
leftMargin=0.55 * inch,
topMargin=0.5 * inch,
bottomMargin=0.5 * inch,
)
W = letter[0] - 1.1 * inch # usable width
# ── Styles ────────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
def S(name, **kw):
s = ParagraphStyle(name, **kw)
return s
TITLE = S("TITLE",
fontName="Helvetica-Bold", fontSize=22, textColor=WHITE,
alignment=TA_CENTER, spaceAfter=2, leading=26)
SUBTITLE = S("SUBTITLE",
fontName="Helvetica", fontSize=11, textColor=HexColor("#AED6F1"),
alignment=TA_CENTER, spaceAfter=4, leading=14)
SEC_HDR = S("SEC_HDR",
fontName="Helvetica-Bold", fontSize=11, textColor=WHITE,
alignment=TA_LEFT, leading=14)
BODY = S("BODY",
fontName="Helvetica", fontSize=9.5, textColor=BLACK,
leading=13, spaceAfter=3)
BODY_B = S("BODY_B",
fontName="Helvetica-Bold", fontSize=9.5, textColor=BLACK,
leading=13, spaceAfter=3)
SMALL = S("SMALL",
fontName="Helvetica", fontSize=8.5, textColor=DARK_GRY,
leading=12, spaceAfter=2)
SMALL_B = S("SMALL_B",
fontName="Helvetica-Bold", fontSize=8.5, textColor=BLACK,
leading=12, spaceAfter=2)
ALERT = S("ALERT",
fontName="Helvetica-Bold", fontSize=10.5, textColor=RED,
alignment=TA_CENTER, leading=14)
FOOTER = S("FOOTER",
fontName="Helvetica-Oblique", fontSize=7.5, textColor=DARK_GRY,
alignment=TA_CENTER)
CENTERED = S("CENTERED",
fontName="Helvetica", fontSize=9, textColor=BLACK,
alignment=TA_CENTER, leading=12)
CENTERED_B = S("CENTERED_B",
fontName="Helvetica-Bold", fontSize=9, textColor=BLACK,
alignment=TA_CENTER, leading=12)
# ── Helper: coloured section header bar ──────────────────────────────────────
def section_header(text, bg=NAVY, icon=""):
label = f"{icon} {text}" if icon else text
t = Table([[Paragraph(label, SEC_HDR)]], colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("ROWPADDING", (0,0), (-1,-1), 6),
("BOX", (0,0), (-1,-1), 0, bg),
]))
return t
def spacer(h=5):
return Spacer(1, h)
# ─────────────────────────────────────────────────────────────────────────────
story = []
# ══ TITLE BANNER ══════════════════════════════════════════════════════════════
banner = Table(
[[Paragraph("COMPARTMENT SYNDROME", TITLE)],
[Paragraph("Quick Reference Guide | Recognition & Emergency Response", SUBTITLE)]],
colWidths=[W]
)
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("ROWPADDING", (0,0), (-1,-1), 8),
("TOPPADDING", (0,0), (-1,0), 12),
("BOTTOMPADDING",(0,1),(-1,1), 12),
]))
story += [banner, spacer(8)]
# ══ DEFINITION ROW ═══════════════════════════════════════════════════════════
def_data = [[
Paragraph(
"<b>DEFINITION:</b> A condition in which rising pressure within a closed fascial compartment "
"reduces capillary perfusion below the level needed for tissue viability, causing ischaemia "
"and — if untreated — irreversible muscle and nerve necrosis.",
S("DEF", fontName="Helvetica", fontSize=9.5, textColor=NAVY,
leading=14, alignment=TA_JUSTIFY)),
]]
def_tbl = Table(def_data, colWidths=[W])
def_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY_LT),
("ROWPADDING", (0,0), (-1,-1), 8),
("BOX", (0,0), (-1,-1), 1.5, NAVY),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING",(0,0), (-1,-1), 10),
]))
story += [def_tbl, spacer(8)]
# ══ TWO-COLUMN SECTION: CAUSES + COMMON SITES ════════════════════════════════
story.append(section_header("CAUSES & COMMON SITES", NAVY))
story.append(spacer(4))
causes = [
["CAUSES (most common first)", "COMMON ANATOMIC SITES"],
[Paragraph("• Fractures — 70% of cases (esp. tibia, forearm)\n"
"• Crush injuries / soft tissue contusions — 23%\n"
"• Tight casts or circumferential dressings\n"
"• Burns (circumferential third-degree)\n"
"• Reperfusion after arterial ischaemia\n"
"• Bleeding disorders / anticoagulation\n"
"• IV fluid extravasation under pressure", SMALL),
Paragraph("• Leg (4 compartments: anterior, lateral,\n"
" deep posterior, superficial posterior)\n"
"• Forearm (volar / dorsal)\n"
"• Hand and foot\n"
"• Thigh and upper arm\n"
"• Buttock\n\n"
"<i>Open fractures do NOT protect against\n"
"compartment syndrome — stay vigilant.</i>", SMALL)],
]
causes_tbl = Table(causes, colWidths=[W*0.5, W*0.5])
causes_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), DARK_GRY),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
("ROWPADDING", (0,0), (-1,-1), 6),
("GRID", (0,0), (-1,-1), 0.5, HexColor("#BDC3C7")),
("VALIGN", (0,1), (-1,-1), "TOP"),
("BACKGROUND", (0,1), (-1,-1), GRAY),
]))
story += [causes_tbl, spacer(8)]
# ══ 6 P's RECOGNITION TABLE ═══════════════════════════════════════════════════
story.append(section_header("RECOGNITION: THE 6 P's", RED))
story.append(spacer(4))
ps_data = [
["P", "SIGN", "DETAILS", "TIMING"],
["Pain", "Pain out of proportion",
"Far worse than injury alone should cause.\nPain with PASSIVE STRETCH of muscles in the\ncompartment — EARLIEST & MOST RELIABLE sign.",
Paragraph("<b><font color='#C0392B'>EARLY</font></b>", CENTERED_B)],
["Paresthesia", "Tingling / Numbness",
"Nerve ischaemia begins. Tingling or numbness\ndistal to the compartment (fingers / toes).",
Paragraph("<b><font color='#C0392B'>EARLY</font></b>", CENTERED_B)],
["Pressure", "Tense / Firm swelling",
"Compartment feels woody or tense on palpation.\nBeyond normal post-injury swelling.",
Paragraph("<b><font color='#E67E22'>EARLY–MID</font></b>", CENTERED_B)],
["Pallor", "Skin paleness",
"Arterial supply being compromised.\nCompare with unaffected limb.",
Paragraph("<b><font color='#E67E22'>MID–LATE</font></b>", CENTERED_B)],
["Paralysis", "Loss of motor function",
"Motor nerve and muscle ischaemia. Patient\ncannot move digits distal to the compartment.",
Paragraph("<b><font color='#922B21'>LATE</font></b>", CENTERED_B)],
["Pulselessness","Absent distal pulse",
"EXTREMELY LATE sign. Tissue is already dying.\nNEVER wait for this before acting.",
Paragraph("<b><font color='#922B21'>VERY LATE</font></b>", CENTERED_B)],
]
ps_tbl = Table(ps_data, colWidths=[W*0.13, W*0.18, W*0.49, W*0.20])
ps_tbl.setStyle(TableStyle([
# Header row
("BACKGROUND", (0,0), (-1,0), RED),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
# Body
("FONTNAME", (0,1), (1,-1), "Helvetica-Bold"),
("FONTSIZE", (0,1), (-1,-1), 9),
("ROWPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.5, HexColor("#BDC3C7")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
# Alternating rows
("BACKGROUND", (0,1), (-1,1), RED_LITE),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), RED_LITE),
("BACKGROUND", (0,4), (-1,4), WHITE),
("BACKGROUND", (0,5), (-1,5), RED_LITE),
("BACKGROUND", (0,6), (-1,6), WHITE),
# Highlight pain row
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
story += [ps_tbl, spacer(4)]
# Pain-stretch callout
callout = Table([[
Paragraph(
"KEY: Pain with PASSIVE STRETCH is the earliest and most actionable sign. "
"Passively extend the fingers/toes — if this triggers severe pain in the compartment, act immediately. "
"Do NOT wait for pulselessness.",
S("COut", fontName="Helvetica-BoldOblique", fontSize=9, textColor=RED,
leading=13, alignment=TA_LEFT))
]], colWidths=[W])
callout.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), RED_LITE),
("BOX", (0,0),(-1,-1), 1.5, RED),
("ROWPADDING", (0,0),(-1,-1), 7),
("LEFTPADDING", (0,0),(-1,-1), 10),
]))
story += [callout, spacer(8)]
# ══ PRESSURE THRESHOLDS ═══════════════════════════════════════════════════════
story.append(section_header("COMPARTMENT PRESSURE THRESHOLDS (when measured)", ORANGE))
story.append(spacer(4))
thresh_data = [
["THRESHOLD", "VALUE", "ACTION"],
["Absolute compartment pressure",
"≥ 30 mmHg",
"Fasciotomy indicated"],
["Delta pressure (Diastolic BP − Compartment Pressure)",
"≤ 30 mmHg",
"Fasciotomy indicated"],
["High clinical suspicion",
"Any pressure",
"Fasciotomy may still be indicated"],
]
thresh_tbl = Table(thresh_data, colWidths=[W*0.42, W*0.25, W*0.33])
thresh_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), ORANGE),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 9),
("ALIGN", (1,0), (1,-1), "CENTER"),
("ALIGN", (2,0), (2,-1), "CENTER"),
("ROWPADDING", (0,0), (-1,-1), 6),
("GRID", (0,0), (-1,-1), 0.5, HexColor("#BDC3C7")),
("BACKGROUND", (0,1), (-1,1), ORG_LITE),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), ORG_LITE),
("FONTNAME", (0,1), (-1,-1), "Helvetica"),
("FONTNAME", (1,1), (1,-1), "Helvetica-Bold"),
("TEXTCOLOR", (2,1), (2,2), GREEN),
("FONTNAME", (2,1), (2,-1), "Helvetica-Bold"),
("LEFTPADDING", (0,0), (-1,-1), 7),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]))
story += [thresh_tbl, spacer(4)]
note = Paragraph(
"<i>Note: Pressure measurement is used when diagnosis is uncertain or patient cannot communicate "
"(sedated, head injury). Clinical diagnosis takes priority — do not delay treatment waiting for a measurement.</i>",
SMALL)
story += [note, spacer(8)]
# ══ EMERGENCY RESPONSE — STEP-BY-STEP ════════════════════════════════════════
story.append(section_header("EMERGENCY RESPONSE — NURSING ACTIONS (IN ORDER)", RED))
story.append(spacer(4))
steps = [
("STEP 1", "NOTIFY PROVIDER IMMEDIATELY",
"Do not wait. Compartment syndrome is a time-critical emergency. Call the provider and "
"document time of notification. Prepare for urgent intervention.",
RED, RED_LITE),
("STEP 2", "REMOVE ALL CONSTRICTIVE ITEMS",
"Bivalve / split the cast down to skin — this alone can significantly reduce pressure. "
"Remove circumferential dressings, bandages, splints, and any external compressive devices "
"to skin level. Do NOT merely loosen — remove completely.",
ORANGE, ORG_LITE),
("STEP 3", "POSITION THE LIMB AT HEART LEVEL",
"Elevate to heart level only (not above). Raising above heart reduces arterial inflow and "
"worsens ischaemia. Lowering below heart increases venous pressure and worsens oedema. "
"Heart level = optimal perfusion gradient.",
HexColor("#1A5276"), NAVY_LT),
("STEP 4", "ADMINISTER OXYGEN AS ORDERED",
"Supplemental oxygen maximises oxygen delivery to ischaemic tissue while awaiting "
"definitive treatment. Establish IV access if not already present.",
GREEN, GRN_LITE),
("STEP 5", "PREPARE FOR FASCIOTOMY",
"Fasciotomy (surgical release of fascia) is the only definitive treatment. "
"Obtain consent if possible. Prepare OR notification. Window: within 6–8 hours of onset "
"for best outcomes. Wounds are left OPEN post-fasciotomy.",
HexColor("#6C3483"), HexColor("#E8DAEF")),
("STEP 6", "MONITOR CONTINUOUSLY",
"Repeat neurovascular checks (6 P's) every 15–30 minutes until resolved or surgeon arrives. "
"Document all findings with timestamps. Monitor vitals, urine output (watch for myoglobinuria "
"— dark urine = rhabdomyolysis), and fluid balance.",
DARK_GRY, GRAY),
]
for code, title, desc, bg, lite in steps:
row = Table(
[[Paragraph(code, S(f"C{code}", fontName="Helvetica-Bold", fontSize=8,
textColor=WHITE, alignment=TA_CENTER, leading=11)),
Paragraph(f"<b>{title}</b><br/>{desc}",
S(f"D{code}", fontName="Helvetica", fontSize=9,
leading=13, textColor=BLACK))]],
colWidths=[W*0.11, W*0.89]
)
row.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), bg),
("BACKGROUND", (1,0),(1,0), lite),
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
("ROWPADDING", (0,0),(-1,-1), 6),
("LEFTPADDING", (0,0),(0,0), 4),
("RIGHTPADDING",(0,0),(0,0), 4),
("LEFTPADDING", (1,0),(1,0), 8),
("BOX", (0,0),(-1,-1), 0.5, HexColor("#BDC3C7")),
]))
story += [row, spacer(3)]
story.append(spacer(6))
# ══ POST-FASCIOTOMY NURSING CARE ══════════════════════════════════════════════
story.append(section_header("POST-FASCIOTOMY NURSING CARE", GREEN))
story.append(spacer(4))
post_data = [
["ASSESSMENT", "WOUND CARE", "SYSTEMIC MONITORING"],
[Paragraph("• Neurovascular checks q1–2h\n"
"• Compare with unaffected limb\n"
"• Monitor for pain relief (improvement\n"
" confirms decompression)\n"
"• Assess for residual deficits\n"
"• Monitor skin graft take if applicable", SMALL),
Paragraph("• Wounds left OPEN — do not close early\n"
"• Vacuum-assisted closure (VAC) device\n"
" applied to manage oedema\n"
"• Delayed primary closure in 3–5 days\n"
" when swelling resolves\n"
"• Aseptic dressing technique always\n"
"• Monitor for wound infection", SMALL),
Paragraph("• Urine output: target >100 mL/hr\n"
" (rhabdomyolysis risk)\n"
"• Monitor urine colour (dark = myoglobin)\n"
"• IV fluids — aggressive if rhabdo present\n"
"• Urine alkalinisation with bicarbonate\n"
" may be ordered (severe tissue damage)\n"
"• Monitor CPK, BMP, renal function\n"
"• K+ levels — released from necrotic cells", SMALL)],
]
post_tbl = Table(post_data, colWidths=[W/3, W/3, W/3])
post_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), GREEN),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
("ROWPADDING", (0,0), (-1,-1), 6),
("GRID", (0,0), (-1,-1), 0.5, HexColor("#BDC3C7")),
("VALIGN", (0,1), (-1,-1), "TOP"),
("BACKGROUND", (0,1), (-1,1), GRN_LITE),
("LEFTPADDING", (0,0), (-1,-1), 7),
]))
story += [post_tbl, spacer(8)]
# ══ COMPLICATIONS IF UNTREATED ════════════════════════════════════════════════
story.append(section_header("CONSEQUENCES OF DELAYED / MISSED DIAGNOSIS", RED))
story.append(spacer(4))
comp_items = [
("Volkmann's Ischaemic Contracture",
"Forearm muscles replaced by fibrotic scar tissue → permanent claw-hand deformity"),
("Rhabdomyolysis",
"Dead muscle releases myoglobin into bloodstream → toxic to kidneys"),
("Acute Kidney Injury / Renal Failure",
"Myoglobin precipitates in tubules → acute tubular necrosis"),
("Permanent Nerve Damage",
"Chronic numbness, paralysis, neuropathic pain in distribution of affected nerves"),
("Limb Loss (Amputation)",
"Gangrenous muscle cannot be saved if fasciotomy is too late"),
("Death",
"From systemic effects of massive rhabdomyolysis, sepsis, and multi-organ failure"),
]
comp_data = [["COMPLICATION", "MECHANISM / OUTCOME"]]
for c, m in comp_items:
comp_data.append([Paragraph(f"<b>{c}</b>", SMALL_B), Paragraph(m, SMALL)])
comp_tbl = Table(comp_data, colWidths=[W*0.38, W*0.62])
comp_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), RED),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
("ROWPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.5, HexColor("#BDC3C7")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("BACKGROUND", (0,1), (-1,1), RED_LITE),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), RED_LITE),
("BACKGROUND", (0,4), (-1,4), WHITE),
("BACKGROUND", (0,5), (-1,5), RED_LITE),
("BACKGROUND", (0,6), (-1,6), WHITE),
("LEFTPADDING", (0,0), (-1,-1), 7),
]))
story += [comp_tbl, spacer(8)]
# ══ SPECIAL POPULATIONS ═══════════════════════════════════════════════════════
story.append(section_header("SPECIAL POPULATIONS & CLINICAL PEARLS", NAVY))
story.append(spacer(4))
pearls = [
("Altered / Unconscious Patients",
"Cannot verbalise pain. Use compartment pressure measurement as primary tool. "
"Maintain high clinical suspicion in any patient with significant extremity injury who "
"cannot communicate."),
("Paediatric Patients",
"Supracondylar humerus fractures carry highest risk in children. "
"Children may not localise pain well — agitation, crying disproportionate to injury, "
"and refusal to move a limb are important indicators."),
("Open Fractures",
"Do NOT assume an open wound decompresses the compartment. "
"Compartment syndrome occurs in open fractures. Vigilance is mandatory."),
("Post-Operative Patients",
"Tight wound closure, haematoma formation, and positional pressure (e.g., lithotomy) "
"can all cause compartment syndrome in the post-op setting."),
("Cast / Splint Patients",
"Bivalve or remove cast completely (not just loosen) at FIRST sign of concern. "
"Teach all cast patients the 6 P's and to report changes immediately."),
]
pearl_rows = [["POPULATION / SITUATION", "CLINICAL PEARL"]]
for pop, pearl in pearls:
pearl_rows.append([Paragraph(f"<b>{pop}</b>", SMALL_B), Paragraph(pearl, SMALL)])
pearl_tbl = Table(pearl_rows, colWidths=[W*0.30, W*0.70])
pearl_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
("ROWPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.5, HexColor("#BDC3C7")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("BACKGROUND", (0,1), (-1,1), NAVY_LT),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), NAVY_LT),
("BACKGROUND", (0,4), (-1,4), WHITE),
("BACKGROUND", (0,5), (-1,5), NAVY_LT),
("LEFTPADDING", (0,0), (-1,-1), 7),
]))
story += [pearl_tbl, spacer(8)]
# ══ QUICK MEMORY AID ══════════════════════════════════════════════════════════
mem_data = [[
Paragraph(
'<b>MEMORY AID — 6 P\'s:</b> <font color="#C0392B"><b>P</b></font>ain out of proportion '
'→ <font color="#C0392B"><b>P</b></font>aresthesia '
'→ <font color="#C0392B"><b>P</b></font>ressure (tense) '
'→ <font color="#C0392B"><b>P</b></font>allor '
'→ <font color="#C0392B"><b>P</b></font>aralysis '
'→ <font color="#C0392B"><b>P</b></font>ulselessness (act BEFORE this)',
S("MEM", fontName="Helvetica", fontSize=9.5, textColor=NAVY,
leading=14, alignment=TA_CENTER))
]]
mem_tbl = Table(mem_data, colWidths=[W])
mem_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), YELLOW),
("BOX", (0,0),(-1,-1), 2, YEL_BRD),
("ROWPADDING", (0,0),(-1,-1), 9),
("LEFTPADDING", (0,0),(-1,-1), 12),
("RIGHTPADDING",(0,0),(-1,-1), 12),
]))
story += [mem_tbl, spacer(6)]
# ══ FOOTER ════════════════════════════════════════════════════════════════════
story.append(HRFlowable(width=W, thickness=0.5, color=DARK_GRY))
story.append(spacer(3))
story.append(Paragraph(
"Quick Reference | Compartment Syndrome Recognition & Emergency Response | "
"MS III Medical-Surgical Nursing | Unit 9 — Musculoskeletal Function | "
"Sources: Bailey & Love's Surgery 28e, Campbell's Operative Orthopaedics 15e, "
"Rosen's Emergency Medicine, Goldman-Cecil Medicine",
FOOTER))
# ── Build ─────────────────────────────────────────────────────────────────────
doc.build(story)
print("PDF generated:", OUTPUT)
cd /home/daytona/workspace/compartment-syndrome-qr && python3 generate_pdf.py
ls -lh /home/daytona/workspace/compartment-syndrome-qr/
Compartment Syndrome Quick Reference
PDF Document · PDF
| Section | Content |
|---|---|
| Definition | Concise clinical definition in a highlighted banner |
| Causes & Common Sites | Side-by-side table - fractures (70%), crush injuries, tight casts, burns, reperfusion; all 6 anatomic compartment regions |
| 6 P's Recognition Table | All six signs with descriptions, colour-coded EARLY / MID / LATE timing - Pain and Paresthesia highlighted as earliest, Pulselessness flagged as extremely late |
| Pain with Passive Stretch callout | Red alert box emphasising this is the most actionable early sign |
| Pressure Thresholds | ≥30 mmHg absolute OR delta pressure ≤30 mmHg → fasciotomy |
| Emergency Response | 6 colour-coded step-by-step nursing actions in order (notify → remove cast → position at heart level → O2 → prepare fasciotomy → continuous monitoring) |
| Post-Fasciotomy Care | 3-column table: neurovascular assessment, wound care (VAC, leave open), systemic monitoring (rhabdomyolysis, urine output, CPK) |
| Consequences if Missed | Volkmann's contracture through death - in order of progression |
| Special Populations | Unconscious patients, paediatric, open fractures, post-op, cast patients |
| Memory Aid | Yellow banner with the 6 P's in sequence |
Create a visual flowchart PDF for fracture classification and immediate management
ls /home/daytona/workspace/ && mkdir -p /home/daytona/workspace/fracture-flowchart
~/fracture-flowchart/generate_flowchart.py
"""
Fracture Classification & Immediate Management — Visual Flowchart PDF
Uses ReportLab canvas (low-level) for precise positioned drawing.
Layout: A4 landscape for maximum width; all elements drawn with absolute coords.
"""
from reportlab.lib.pagesizes import A4, landscape
from reportlab.lib.units import cm, mm
from reportlab.lib.colors import HexColor, white, black
from reportlab.pdfgen import canvas
import math
OUTPUT = "/home/daytona/workspace/fracture-flowchart/Fracture_Classification_Management_Flowchart.pdf"
PW, PH = landscape(A4) # 841.89 x 595.28 pt
M = 0.45 * cm # margin
# ── Palette ────────────────────────────────────────────────────────────────
NAVY = HexColor("#1A3A5C")
NAVY_LT = HexColor("#D6E4F0")
SKY = HexColor("#2E86C1")
SKY_LT = HexColor("#AED6F1")
RED = HexColor("#C0392B")
RED_LT = HexColor("#FADBD8")
ORANGE = HexColor("#D35400")
ORG_LT = HexColor("#FAE5D3")
GREEN = HexColor("#1E8449")
GRN_LT = HexColor("#D5F5E3")
PURPLE = HexColor("#6C3483")
PUR_LT = HexColor("#E8DAEF")
TEAL = HexColor("#148F77")
TEA_LT = HexColor("#D1F2EB")
GOLD = HexColor("#B7950B")
GOLD_LT = HexColor("#FCF3CF")
GRAY_D = HexColor("#5D6D7E")
GRAY_L = HexColor("#F2F3F4")
BORDER = HexColor("#BDC3C7")
c = canvas.Canvas(OUTPUT, pagesize=landscape(A4))
c.setTitle("Fracture Classification & Immediate Management Flowchart")
# ── Utility helpers ────────────────────────────────────────────────────────
def rect_fill(x, y, w, h, fill, stroke=None, radius=4):
c.saveState()
c.setFillColor(fill)
if stroke:
c.setStrokeColor(stroke)
c.setLineWidth(1.2)
else:
c.setStrokeColor(fill)
c.setLineWidth(0)
c.roundRect(x, y, w, h, radius, fill=1, stroke=1 if stroke else 0)
c.restoreState()
def text_center(x, y, w, txt, font="Helvetica", size=8, color=black, leading=10):
c.saveState()
c.setFillColor(color)
c.setFont(font, size)
lines = txt.split("\n")
total_h = len(lines) * leading
start_y = y + total_h / 2 - leading * 0.3
for i, line in enumerate(lines):
c.drawCentredString(x + w / 2, start_y - i * leading, line)
c.restoreState()
def text_left(x, y, txt, font="Helvetica", size=8, color=black, leading=10):
c.saveState()
c.setFillColor(color)
c.setFont(font, size)
lines = txt.split("\n")
for i, line in enumerate(lines):
c.drawString(x, y - i * leading, line)
c.restoreState()
def arrow_down(x, y, length=14, color=GRAY_D, width=1.5):
c.saveState()
c.setStrokeColor(color)
c.setFillColor(color)
c.setLineWidth(width)
c.line(x, y, x, y - length + 5)
# arrowhead
p = c.beginPath()
p.moveTo(x, y - length)
p.lineTo(x - 4, y - length + 6)
p.lineTo(x + 4, y - length + 6)
p.close()
c.drawPath(p, fill=1, stroke=0)
c.restoreState()
def arrow_right(x, y, length=14, color=GRAY_D, width=1.5):
c.saveState()
c.setStrokeColor(color)
c.setFillColor(color)
c.setLineWidth(width)
c.line(x, y, x + length - 5, y)
p = c.beginPath()
p.moveTo(x + length, y)
p.lineTo(x + length - 6, y + 4)
p.lineTo(x + length - 6, y - 4)
p.close()
c.drawPath(p, fill=1, stroke=0)
c.restoreState()
def arrow_left(x, y, length=14, color=GRAY_D, width=1.5):
c.saveState()
c.setStrokeColor(color)
c.setFillColor(color)
c.setLineWidth(width)
c.line(x, y, x - length + 5, y)
p = c.beginPath()
p.moveTo(x - length, y)
p.lineTo(x - length + 6, y + 4)
p.lineTo(x - length + 6, y - 4)
p.close()
c.drawPath(p, fill=1, stroke=0)
c.restoreState()
def diamond(cx, cy, hw, hh, fill, stroke):
"""Draw a diamond centred at cx,cy with half-widths hw, hh."""
c.saveState()
c.setFillColor(fill)
c.setStrokeColor(stroke)
c.setLineWidth(1.2)
p = c.beginPath()
p.moveTo(cx, cy + hh)
p.lineTo(cx + hw, cy)
p.lineTo(cx, cy - hh)
p.lineTo(cx - hw, cy)
p.close()
c.drawPath(p, fill=1, stroke=1)
c.restoreState()
def connector_line(x1, y1, x2, y2, color=GRAY_D, width=1.5, arrow_end=True):
"""Straight or L-shaped connector with arrowhead at end."""
c.saveState()
c.setStrokeColor(color)
c.setFillColor(color)
c.setLineWidth(width)
c.line(x1, y1, x2, y2)
if arrow_end:
# determine direction
dx, dy = x2 - x1, y2 - y1
angle = math.atan2(dy, dx)
arr_len = 7
p = c.beginPath()
p.moveTo(x2, y2)
p.lineTo(x2 - arr_len * math.cos(angle - 0.4),
y2 - arr_len * math.sin(angle - 0.4))
p.lineTo(x2 - arr_len * math.cos(angle + 0.4),
y2 - arr_len * math.sin(angle + 0.4))
p.close()
c.drawPath(p, fill=1, stroke=0)
c.restoreState()
def bent_connector(x1, y1, x2, y2, bend_x=None, color=GRAY_D, width=1.5):
"""Horizontal then vertical connector (or vertical then horizontal)."""
c.saveState()
c.setStrokeColor(color)
c.setFillColor(color)
c.setLineWidth(width)
if bend_x is not None:
c.line(x1, y1, bend_x, y1)
c.line(bend_x, y1, bend_x, y2)
c.line(bend_x, y2, x2, y2)
else:
mid_y = (y1 + y2) / 2
c.line(x1, y1, x1, mid_y)
c.line(x1, mid_y, x2, mid_y)
c.line(x2, mid_y, x2, y2)
# arrowhead at end
arr_len = 7
dx, dy = x2 - (bend_x if bend_x else x1), 0
angle = math.atan2(y2 - (y2), x2 - (bend_x if bend_x else x1))
# simplified: always points toward x2,y2
if x2 > (bend_x if bend_x else x1):
px, py = x2, y2
p = c.beginPath()
p.moveTo(px, py)
p.lineTo(px - arr_len, py + 4)
p.lineTo(px - arr_len, py - 4)
p.close()
else:
px, py = x2, y2
p = c.beginPath()
p.moveTo(px, py)
p.lineTo(px + arr_len, py + 4)
p.lineTo(px + arr_len, py - 4)
p.close()
c.drawPath(p, fill=1, stroke=0)
c.restoreState()
# ══════════════════════════════════════════════════════════════════════════════
# PAGE 1 — FRACTURE CLASSIFICATION FLOWCHART
# ══════════════════════════════════════════════════════════════════════════════
# ── Title Banner ──────────────────────────────────────────────────────────
rect_fill(M, PH - 1.6*cm, PW - 2*M, 1.5*cm, NAVY)
text_center(M, PH - 1.1*cm, PW - 2*M,
"FRACTURE CLASSIFICATION & IMMEDIATE MANAGEMENT FLOWCHART",
"Helvetica-Bold", 15, white)
text_center(M, PH - 1.5*cm, PW - 2*M,
"Page 1 of 2 — Classification System",
"Helvetica", 8.5, HexColor("#AED6F1"))
# ── Start node ────────────────────────────────────────────────────────────
TOP_Y = PH - 2.3*cm
SN_W, SN_H = 3.6*cm, 0.85*cm
SN_X = (PW - SN_W) / 2
rect_fill(SN_X, TOP_Y - SN_H, SN_W, SN_H, NAVY, NAVY, radius=20)
text_center(SN_X, TOP_Y - SN_H/2 - 0.05*cm, SN_W,
"SUSPECTED FRACTURE", "Helvetica-Bold", 9.5, white)
# Arrow down
arrow_down(PW/2, TOP_Y - SN_H - 1, 14, NAVY, 2)
# ── Diamond: Skin Intact? ─────────────────────────────────────────────────
D1_CX, D1_CY = PW/2, TOP_Y - SN_H - 1.6*cm
D1_HW, D1_HH = 2.6*cm, 0.85*cm
diamond(D1_CX, D1_CY, D1_HW, D1_HH, GOLD_LT, GOLD)
text_center(D1_CX - D1_HW, D1_CY - 0.15*cm, D1_HW*2,
"Is skin\nINTACT?", "Helvetica-Bold", 8.5, GOLD)
# YES label + arrow down left
connector_line(D1_CX - D1_HW, D1_CY,
D1_CX - D1_HW - 2.9*cm, D1_CY, GOLD, 1.5, True)
text_left(D1_CX - D1_HW - 1.6*cm, D1_CY + 5, "YES", "Helvetica-Bold", 7.5, GREEN)
# NO label + arrow right
connector_line(D1_CX + D1_HW, D1_CY,
D1_CX + D1_HW + 2.9*cm, D1_CY, RED, 1.5, True)
text_left(D1_CX + D1_HW + 0.3*cm, D1_CY + 5, "NO", "Helvetica-Bold", 7.5, RED)
# ── CLOSED box ────────────────────────────────────────────────────────────
CL_W, CL_H = 3.4*cm, 1.0*cm
CL_X = D1_CX - D1_HW - 2.9*cm - CL_W
CL_Y = D1_CY - CL_H / 2
rect_fill(CL_X, CL_Y, CL_W, CL_H, GRN_LT, GREEN, radius=5)
text_center(CL_X, CL_Y + CL_H/2, CL_W,
"CLOSED\nFRACTURE", "Helvetica-Bold", 9, GREEN)
# ── OPEN box ──────────────────────────────────────────────────────────────
OP_W, OP_H = 3.4*cm, 1.0*cm
OP_X = D1_CX + D1_HW + 2.9*cm
OP_Y = D1_CY - OP_H / 2
rect_fill(OP_X, OP_Y, OP_W, OP_H, RED_LT, RED, radius=5)
text_center(OP_X, OP_Y + OP_H/2, OP_W,
"OPEN (COMPOUND)\nFRACTURE", "Helvetica-Bold", 9, RED)
# Arrow down from CLOSED
arrow_down(CL_X + CL_W/2, CL_Y - 1, 13, GREEN, 1.8)
# Arrow down from OPEN
arrow_down(OP_X + OP_W/2, OP_Y - 1, 13, RED, 1.8)
# ── FRACTURE TYPE grid (closed types) ─────────────────────────────────────
# 6 fracture types arranged in 2 rows of 3 under closed
FTYPE_Y_TOP = CL_Y - 1.5*cm
FT_W, FT_H = 3.1*cm, 1.8*cm
GAP = 0.3*cm
COLS_X_START = CL_X + CL_W/2 - (3*FT_W + 2*GAP)/2
ftypes = [
("TRANSVERSE", "Clean perpendicular break\nacross bone shaft", SKY, SKY_LT),
("OBLIQUE", "Diagonal break\nalong bone axis", TEAL, TEA_LT),
("SPIRAL", "Twisting force\nwraps around bone\n(abuse marker in kids)", PURPLE, PUR_LT),
("COMMINUTED", "Bone shattered into\n3+ fragments\n(harder to fix)", ORANGE, ORG_LT),
("GREENSTICK", "Partial break, one\ncortex intact\n(children only)", GREEN, GRN_LT),
("STRESS", "Hairline crack from\nrepetitive force\n(athletes, military)",NAVY, NAVY_LT),
]
for i, (name, desc, col, lite) in enumerate(ftypes):
row, col_idx = divmod(i, 3)
fx = COLS_X_START + col_idx * (FT_W + GAP)
fy = FTYPE_Y_TOP - row * (FT_H + 0.3*cm) - FT_H
rect_fill(fx, fy, FT_W, FT_H, lite, col, radius=4)
# name header strip
rect_fill(fx, fy + FT_H - 0.5*cm, FT_W, 0.5*cm, col, col, radius=3)
text_center(fx, fy + FT_H - 0.25*cm, FT_W, name, "Helvetica-Bold", 7.5, white)
text_center(fx, fy + (FT_H - 0.5*cm)/2, FT_W, desc, "Helvetica", 7, col)
# section label
rect_fill(COLS_X_START - 0.1*cm, FTYPE_Y_TOP + 0.1*cm, 3*FT_W + 2*GAP + 0.2*cm, 0.4*cm, GRAY_L, BORDER, 3)
text_center(COLS_X_START - 0.1*cm, FTYPE_Y_TOP + 0.25*cm, 3*FT_W + 2*GAP + 0.2*cm,
"CLOSED FRACTURE PATTERNS", "Helvetica-Bold", 7, GRAY_D)
# ── OPEN fracture Gustilo classification ─────────────────────────────────
GUST_Y_TOP = OP_Y - 1.5*cm
GT_W = 3.2*cm
GT_H = 1.9*cm
GUST_X = OP_X + OP_W/2 - GT_W/2
gust_types = [
("TYPE I",
"Wound < 1 cm\nClean\nMinimal soft-tissue\ndamage",
GRN_LT, GREEN),
("TYPE II",
"Wound 1–10 cm\nModerate contam.\nModerate soft-\ntissue damage",
GOLD_LT, GOLD),
("TYPE III-A",
"Wound > 10 cm\nHigh contamination\nAdequate soft-\ntissue coverage",
ORG_LT, ORANGE),
("TYPE III-B",
"Wound > 10 cm\nPeriosteal stripping\nRequires flap for\ncoverage",
RED_LT, RED),
("TYPE III-C",
"Any size wound\n+ Arterial injury\nrequiring repair\n(LIMB-THREATENING)",
HexColor("#F9EBEA"), HexColor("#922B21")),
]
GT_GAP = 0.25*cm
GUST_X_START = OP_X + OP_W/2 - (5*GT_W + 4*GT_GAP)/2
for i, (name, desc, lite, col) in enumerate(gust_types):
gx = GUST_X_START + i*(GT_W + GT_GAP)
gy = GUST_Y_TOP - GT_H
rect_fill(gx, gy, GT_W, GT_H, lite, col, radius=4)
rect_fill(gx, gy + GT_H - 0.5*cm, GT_W, 0.5*cm, col, col, radius=3)
text_center(gx, gy + GT_H - 0.25*cm, GT_W, name, "Helvetica-Bold", 7.5, white)
text_center(gx, gy + (GT_H - 0.5*cm)/2, GT_W, desc, "Helvetica", 6.8, col)
# Gustilo label
rect_fill(GUST_X_START - 0.1*cm, GUST_Y_TOP + 0.1*cm,
5*GT_W + 4*GT_GAP + 0.2*cm, 0.4*cm, GRAY_L, BORDER, 3)
text_center(GUST_X_START - 0.1*cm, GUST_Y_TOP + 0.25*cm,
5*GT_W + 4*GT_GAP + 0.2*cm,
"GUSTILO-ANDERSON OPEN FRACTURE CLASSIFICATION",
"Helvetica-Bold", 7, GRAY_D)
# ── SPECIAL FRACTURE TYPES bar (across bottom) ────────────────────────────
SFT_Y = 1.5*cm
SFT_TOTAL_W = PW - 2*M
SFT_H = 2.1*cm
special = [
("PATHOLOGIC", "Fracture through diseased bone\n(tumor, osteomyelitis,\nosteoporosis)\nMinimal or no trauma", PURPLE, PUR_LT),
("AVULSION", "Fragment pulled away\nby tendon or ligament\nforce at attachment\nsite", TEAL, TEA_LT),
("INTRA-ARTICULAR","Fracture line enters\na joint surface\nRisk: post-traumatic\narthritis + stiffness", ORANGE, ORG_LT),
("PERIPROSTHETIC","Fracture around\na joint implant\n(hip/knee replacement)\nComplex fixation", NAVY, NAVY_LT),
("COMPRESSION", "Vertebral body collapse\nfrom axial load\nCommon in osteoporosis\nDowager's hump risk", RED, RED_LT),
("IMPACTED", "Bone ends driven\ninto each other\nAppears stable but\nstill needs fixation", GREEN, GRN_LT),
]
SFT_W = (SFT_TOTAL_W - 5*0.25*cm) / 6
for i, (name, desc, col, lite) in enumerate(special):
sx = M + i*(SFT_W + 0.25*cm)
sy = SFT_Y
rect_fill(sx, sy, SFT_W, SFT_H, lite, col, radius=4)
rect_fill(sx, sy + SFT_H - 0.5*cm, SFT_W, 0.5*cm, col, col, radius=3)
text_center(sx, sy + SFT_H - 0.25*cm, SFT_W, name, "Helvetica-Bold", 7, white)
text_center(sx, sy + (SFT_H - 0.5*cm)/2, SFT_W, desc, "Helvetica", 6.5, col)
# Special label bar
rect_fill(M, SFT_Y + SFT_H, SFT_TOTAL_W, 0.4*cm, GRAY_D, GRAY_D, radius=2)
text_center(M, SFT_Y + SFT_H + 0.22*cm, SFT_TOTAL_W,
"ADDITIONAL / SPECIAL FRACTURE TYPES",
"Helvetica-Bold", 7.5, white)
# ── Footer page 1 ─────────────────────────────────────────────────────────
c.setFillColor(GRAY_D)
c.setFont("Helvetica-Oblique", 7)
c.drawCentredString(PW/2, 0.35*cm,
"Fracture Classification & Immediate Management | MS III Medical-Surgical Nursing | Page 1 of 2")
c.showPage()
# ══════════════════════════════════════════════════════════════════════════════
# PAGE 2 — IMMEDIATE MANAGEMENT FLOWCHART
# ══════════════════════════════════════════════════════════════════════════════
# ── Title Banner ──────────────────────────────────────────────────────────
rect_fill(M, PH - 1.6*cm, PW - 2*M, 1.5*cm, RED)
text_center(M, PH - 1.1*cm, PW - 2*M,
"FRACTURE IMMEDIATE MANAGEMENT FLOWCHART",
"Helvetica-Bold", 15, white)
text_center(M, PH - 1.5*cm, PW - 2*M,
"Page 2 of 2 — Emergency Response & Treatment Pathways",
"Helvetica", 8.5, HexColor("#FADBD8"))
# ── Start box ─────────────────────────────────────────────────────────────
TOP_Y2 = PH - 2.3*cm
SB_W, SB_H = 4.5*cm, 0.85*cm
SB_X = (PW - SB_W) / 2
rect_fill(SB_X, TOP_Y2 - SB_H, SB_W, SB_H, RED, RED, radius=20)
text_center(SB_X, TOP_Y2 - SB_H/2, SB_W,
"FRACTURE IDENTIFIED", "Helvetica-Bold", 10, white)
# ── Step 1: Primary survey ─────────────────────────────────────────────────
arrow_down(PW/2, TOP_Y2 - SB_H - 1, 14, RED, 2)
S1_Y = TOP_Y2 - SB_H - 1.8*cm
S1_W = PW - 2*M
S1_H = 1.9*cm
S1_X = M
rect_fill(S1_X, S1_Y - S1_H, S1_W, S1_H, NAVY_LT, NAVY, radius=5)
rect_fill(S1_X, S1_Y - 0.55*cm, S1_W, 0.55*cm, NAVY, NAVY, radius=4)
text_center(S1_X, S1_Y - 0.27*cm, S1_W,
"STEP 1: PRIMARY SURVEY & IMMEDIATE ASSESSMENT",
"Helvetica-Bold", 10, white)
# 5 sub-boxes in step 1
SUB1 = [
("ABCDE\nAssessment", "Airway, Breathing,\nCirculation,\nDisability, Exposure"),
("Control\nBleeding", "Direct pressure\nProximal tourniquet\nif arterial bleed"),
("Neurovascular\nCheck","Distal pulse\nCapillary refill\nSensation & motor"),
("Expose\nInjury", "Cut clothing\nVisual assessment\nDo NOT force limb"),
("Pain\nManagement", "IV access\nAnalgesics as ordered\nReassure patient"),
]
sub1_w = (S1_W - 4*0.2*cm) / 5
for i, (title, body) in enumerate(SUB1):
sx = S1_X + i*(sub1_w + 0.2*cm)
sy = S1_Y - S1_H
rect_fill(sx, sy, sub1_w, S1_H - 0.55*cm, white, NAVY, 3)
text_center(sx, sy + (S1_H - 0.55*cm)*0.72, sub1_w, title, "Helvetica-Bold", 7.5, NAVY)
text_center(sx, sy + (S1_H - 0.55*cm)*0.32, sub1_w, body, "Helvetica", 6.8, HexColor("#1A3A5C"))
# ── Arrow + Diamond: Open fracture? ──────────────────────────────────────
arrow_down(PW/2, S1_Y - S1_H - 1, 14, RED, 2)
D2_CX, D2_CY = PW/2, S1_Y - S1_H - 1.8*cm
D2_HW, D2_HH = 2.8*cm, 0.9*cm
diamond(D2_CX, D2_CY, D2_HW, D2_HH, GOLD_LT, GOLD)
text_center(D2_CX - D2_HW, D2_CY - 0.18*cm, D2_HW*2,
"OPEN\nFRACTURE?", "Helvetica-Bold", 9, GOLD)
# YES → left branch
connector_line(D2_CX - D2_HW, D2_CY,
D2_CX - D2_HW - 3.5*cm, D2_CY, RED, 1.5)
text_left(D2_CX - D2_HW - 2.0*cm, D2_CY + 6, "YES", "Helvetica-Bold", 7.5, RED)
# NO → right
connector_line(D2_CX + D2_HW, D2_CY,
D2_CX + D2_HW + 3.5*cm, D2_CY, GREEN, 1.5)
text_left(D2_CX + D2_HW + 0.3*cm, D2_CY + 6, "NO", "Helvetica-Bold", 7.5, GREEN)
# ── LEFT branch: OPEN FRACTURE management ────────────────────────────────
OP2_W = 4.2*cm
OP2_X = D2_CX - D2_HW - 3.5*cm - OP2_W
OP2_H = 3.5*cm
OP2_Y = D2_CY - OP2_H/2
rect_fill(OP2_X, OP2_Y, OP2_W, OP2_H, RED_LT, RED, 4)
rect_fill(OP2_X, OP2_Y + OP2_H - 0.5*cm, OP2_W, 0.5*cm, RED, RED, 3)
text_center(OP2_X, OP2_Y + OP2_H - 0.25*cm, OP2_W,
"OPEN FRACTURE PROTOCOL", "Helvetica-Bold", 8, white)
text_center(OP2_X, OP2_Y + (OP2_H - 0.5*cm)*0.5, OP2_W,
"1. Moist sterile dressing\n"
"2. Do NOT reduce / push bone in\n"
"3. IV antibiotics STAT\n"
" (within 1 hr of injury)\n"
"4. Tetanus prophylaxis\n"
"5. Urgent OR consult\n"
"6. Surgical debridement\n"
" within 6-8 hrs\n"
"7. Wound left OPEN",
"Helvetica", 6.8, RED)
# ── RIGHT branch: CLOSED FRACTURE management ─────────────────────────────
CL2_X = D2_CX + D2_HW + 3.5*cm
CL2_W = 4.0*cm
CL2_H = 3.2*cm
CL2_Y = D2_CY - CL2_H/2
rect_fill(CL2_X, CL2_Y, CL2_W, CL2_H, GRN_LT, GREEN, 4)
rect_fill(CL2_X, CL2_Y + CL2_H - 0.5*cm, CL2_W, 0.5*cm, GREEN, GREEN, 3)
text_center(CL2_X, CL2_Y + CL2_H - 0.25*cm, CL2_W,
"CLOSED FRACTURE PROTOCOL", "Helvetica-Bold", 8, white)
text_center(CL2_X, CL2_Y + (CL2_H - 0.5*cm)*0.5, CL2_W,
"1. Splint in position found\n"
" (joint above AND below)\n"
"2. Pad bony prominences\n"
"3. Neurovascular check\n"
" before AND after splint\n"
"4. Imaging (X-ray)\n"
"5. Analgesia\n"
"6. Elevate limb",
"Helvetica", 6.8, GREEN)
# ── Centre: REDUCTION diamond ─────────────────────────────────────────────
arrow_down(PW/2, D2_CY - D2_HH - 1, 14, NAVY, 2)
D3_CX, D3_CY = PW/2, D2_CY - D2_HH - 1.8*cm
D3_HW, D3_HH = 2.6*cm, 0.85*cm
diamond(D3_CX, D3_CY, D3_HW, D3_HH, NAVY_LT, NAVY)
text_center(D3_CX - D3_HW, D3_CY - 0.15*cm, D3_HW*2,
"NEEDS\nREDUCTION?", "Helvetica-Bold", 8.5, NAVY)
# YES arrow left
connector_line(D3_CX - D3_HW, D3_CY,
D3_CX - D3_HW - 2.8*cm, D3_CY, NAVY, 1.5)
text_left(D3_CX - D3_HW - 1.5*cm, D3_CY + 6, "YES", "Helvetica-Bold", 7.5, NAVY)
# NO arrow right
connector_line(D3_CX + D3_HW, D3_CY,
D3_CX + D3_HW + 2.8*cm, D3_CY, NAVY, 1.5)
text_left(D3_CX + D3_HW + 0.3*cm, D3_CY + 6, "NO", "Helvetica-Bold", 7.5, NAVY)
# ── Reduction types ───────────────────────────────────────────────────────
RED_TYP_W = 4.5*cm
RED_TYP_H = 2.5*cm
# Closed Reduction
CR_X = D3_CX - D3_HW - 2.8*cm - RED_TYP_W
CR_Y = D3_CY - RED_TYP_H/2
rect_fill(CR_X, CR_Y, RED_TYP_W, RED_TYP_H, SKY_LT, SKY, 4)
rect_fill(CR_X, CR_Y + RED_TYP_H - 0.5*cm, RED_TYP_W, 0.5*cm, SKY, SKY, 3)
text_center(CR_X, CR_Y + RED_TYP_H - 0.25*cm, RED_TYP_W,
"CLOSED REDUCTION", "Helvetica-Bold", 8, white)
text_center(CR_X, CR_Y + (RED_TYP_H-0.5*cm)/2, RED_TYP_W,
"Manual manipulation\nunder analgesia/sedation\nFracture too complex?\n→ Proceed to ORIF",
"Helvetica", 7, SKY)
# Open Reduction (ORIF)
OR_X = D3_CX + D3_HW + 2.8*cm
OR_Y = D3_CY - RED_TYP_H/2
rect_fill(OR_X, OR_Y, RED_TYP_W, RED_TYP_H, PUR_LT, PURPLE, 4)
rect_fill(OR_X, OR_Y + RED_TYP_H - 0.5*cm, RED_TYP_W, 0.5*cm, PURPLE, PURPLE, 3)
text_center(OR_X, OR_Y + RED_TYP_H - 0.25*cm, RED_TYP_W,
"DIRECT IMMOBILIZATION", "Helvetica-Bold", 8, white)
text_center(OR_X, OR_Y + (RED_TYP_H-0.5*cm)/2, RED_TYP_W,
"Stable undisplaced fracture\n→ Immobilize directly\nNo manipulation needed",
"Helvetica", 7, PURPLE)
# Both converge downward
arrow_down(CR_X + RED_TYP_W/2, CR_Y - 1, 12, NAVY, 1.5)
arrow_down(OR_X + RED_TYP_W/2, OR_Y - 1, 12, NAVY, 1.5)
arrow_down(D3_CX, D3_CY - D3_HH - 1, 12, NAVY, 1.5)
# ── IMMOBILIZATION OPTIONS ────────────────────────────────────────────────
IMM_Y_TOP = D3_CY - D3_HH - 1.6*cm
IMM_H = 2.8*cm
IMM_W = (PW - 2*M - 3*0.3*cm) / 4
IMM_ITEMS = [
("CAST / SPLINT",
"Most common\nNoninvasive\nSplint for acute\nswelling first\nCast when swelling\nresolves",
TEAL, TEA_LT),
("TRACTION",
"Skin or skeletal\nContinuous force\nWeights hang freely\nCommon: Buck's for\nhip/femur pre-op",
NAVY, NAVY_LT),
("EXTERNAL FIXATION",
"Open fractures\nSevere soft-tissue\nTemporary in\npolytrauma\n(damage control)",
ORANGE, ORG_LT),
("ORIF\n(Internal Fixation)",
"Plates, screws,\nIM nails, rods\nUnstable / displaced\nIntra-articular\nJoint replacement",
PURPLE, PUR_LT),
]
rect_fill(M, IMM_Y_TOP, PW - 2*M, 0.45*cm, NAVY, NAVY, 3)
text_center(M, IMM_Y_TOP + 0.25*cm, PW-2*M,
"IMMOBILIZATION OPTIONS", "Helvetica-Bold", 9, white)
for i, (name, desc, col, lite) in enumerate(IMM_ITEMS):
ix = M + i*(IMM_W + 0.3*cm)
iy = IMM_Y_TOP - IMM_H
rect_fill(ix, iy, IMM_W, IMM_H, lite, col, 4)
rect_fill(ix, iy + IMM_H - 0.5*cm, IMM_W, 0.5*cm, col, col, 3)
text_center(ix, iy + IMM_H - 0.25*cm, IMM_W, name, "Helvetica-Bold", 8, white)
text_center(ix, iy + (IMM_H-0.5*cm)/2, IMM_W, desc, "Helvetica", 6.8, col)
# ── ONGOING NURSING MONITORING strip ─────────────────────────────────────
MON_Y = IMM_Y_TOP - IMM_H - 0.5*cm
MON_H = 2.3*cm
MON_W = PW - 2*M
rect_fill(M, MON_Y - MON_H, MON_W, MON_H, GRAY_L, BORDER, 4)
rect_fill(M, MON_Y - 0.48*cm, MON_W, 0.48*cm, GRAY_D, GRAY_D, 3)
text_center(M, MON_Y - 0.24*cm, MON_W,
"ONGOING NURSING MONITORING (ALL FRACTURES)",
"Helvetica-Bold", 9, white)
MON_ITEMS = [
("Neurovascular\nChecks",
"6 P's q1-2h\nDistal pulse\nCapillary refill\nSensation & motor"),
("Compartment\nSyndrome Watch",
"Pain out of\nproportion\nPain w/ passive\nstretch → ACT NOW"),
("Immobilization\nIntegrity",
"Cast/splint not\ntoo tight\nNo wrinkles\nElevation maintained"),
("Complication\nPrevention",
"DVT prophylaxis\nTurn & reposition\nIncentive spirometry\nSkin assessment"),
("Wound / Pin\nSite Care",
"External fixator:\nassess pin sites\nAseptic technique\nWatch for infection"),
("Patient\nEducation",
"6 P's warning signs\nActivity restrictions\nFollow-up compliance\nMedication teaching"),
]
mon_w = (MON_W - 5*0.2*cm) / 6
for i, (title, desc) in enumerate(MON_ITEMS):
mx = M + i*(mon_w + 0.2*cm)
my = MON_Y - MON_H
rect_fill(mx, my, mon_w, MON_H - 0.48*cm, white, BORDER, 3)
text_center(mx, my + (MON_H-0.48*cm)*0.72, mon_w, title, "Helvetica-Bold", 7, GRAY_D)
text_center(mx, my + (MON_H-0.48*cm)*0.3, mon_w, desc, "Helvetica", 6.5, HexColor("#424949"))
# ── Key Nursing Rules bar ─────────────────────────────────────────────────
RULES_Y = MON_Y - MON_H - 0.4*cm
RULES_H = 1.15*cm
rect_fill(M, RULES_Y - RULES_H, PW-2*M, RULES_H, GOLD_LT, GOLD, 4)
rules_txt = (
"KEY RULES: Splint ABOVE & BELOW fracture | "
"Check neuro-vascular BEFORE & AFTER splinting | "
"Open fracture = contaminated = IV antibiotics NOW | "
"NEVER intentionally elicit crepitation | "
"Do NOT force a fractured limb into position | "
"Fat embolism watch: onset 24-72 hrs, respiratory + confusion + petechiae"
)
text_center(M, RULES_Y - RULES_H/2, PW-2*M, rules_txt, "Helvetica-Bold", 7.2, GOLD)
# ── Footer page 2 ─────────────────────────────────────────────────────────
c.setFillColor(GRAY_D)
c.setFont("Helvetica-Oblique", 7)
c.drawCentredString(
PW/2, 0.35*cm,
"Fracture Classification & Immediate Management | "
"MS III Medical-Surgical Nursing | Page 2 of 2 | "
"Sources: Campbell's Operative Orthopaedics 15e, Rosen's Emergency Medicine, Bailey & Love 28e"
)
c.save()
print("PDF saved:", OUTPUT)
cd /home/daytona/workspace/fracture-flowchart && python3 generate_flowchart.py
ls -lh /home/daytona/workspace/fracture-flowchart/
Fracture Classification Management Flowchart
PDF Document · PDF
Page 1 - Classification Flowchart (A4 Landscape)
- Start node → decision diamond: "Is skin intact?"
- LEFT branch (YES - Closed): 6 fracture pattern cards in 2 rows - Transverse, Oblique, Spiral, Comminuted, Greenstick, Stress - each with description and colour coding
- RIGHT branch (NO - Open): Full Gustilo-Anderson 5-tier classification (Type I → III-C) with wound size, contamination, and soft tissue criteria for each type
- Bottom strip: 6 additional/special fracture types - Pathologic, Avulsion, Intra-articular, Periprosthetic, Compression, Impacted
Page 2 - Immediate Management Flowchart (A4 Landscape)
- Start node → Step 1: 5-box primary survey strip (ABCDE, Bleeding control, Neurovascular check, Expose injury, Pain management)
- Decision diamond: "Open fracture?" → YES/NO branching
- Open protocol: Sterile dressing, IV antibiotics STAT, tetanus, urgent OR, debridement within 6-8 hrs, wound left open
- Closed protocol: Splint (joint above AND below), neuro check before/after, imaging, elevate
- Decision diamond: "Needs reduction?" → Closed reduction vs Direct immobilization
- 4 immobilization option cards: Cast/Splint, Traction, External Fixation, ORIF
- Ongoing monitoring strip: 6 panels - neurovascular checks, compartment syndrome watch, immobilization integrity, complication prevention, wound/pin site care, patient education
- Key nursing rules banner (gold) with all critical rules including fat embolism timing
“Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Also, synthesis additional information from other sources pertinent to this chapter that are important for me to know as a nurse. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_48__ASSESSMENT_AND_MANAGEMENT_OF_PATIENTS_WITH_OBESITY.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
- Obesity as a disease, BMI classification, multifactorial causes, associated diseases
- Lifestyle modification, pharmacotherapy, nonsurgical interventions
- The 4 bariatric procedures, pre/post-op nursing management, nursing process
- Exact BMI thresholds table with AHA/ACC/TOS guideline values
- Waist circumference cutoffs (clinically more important than BMI alone)
- Metabolic syndrome full criteria with all 5 components and insulin resistance as the core
- OSA deep dive - prevalence, cardiovascular consequences, comorbidity statistics, nursing screening role
- GLP-1 agonists (semaglutide/Ozempic) - the current pharmacotherapy revolution, including surgical aspiration risk that nurses must communicate to teams
- Dumping syndrome - early vs. late, mechanisms, dietary management, octreotide for refractory cases
- Calcium citrate vs. carbonate distinction - a commonly tested post-bariatric nursing detail
- Specific nutritional deficiency consequences for each supplement type
- Weight stigma in healthcare - evidence-based framing for person-first, nonjudgmental care
Generate a reference card on post-bariatric nursing complications and interventions
mkdir -p /home/daytona/workspace/bariatric-refcard
~/bariatric-refcard/generate_refcard.py
"""
Post-Bariatric Surgery Nursing Complications & Interventions — Reference Card PDF
Two-sided A4 landscape: Page 1 = Early/Acute complications, Page 2 = Late/Chronic + Diet + Supplements
"""
from reportlab.lib.pagesizes import A4, landscape
from reportlab.lib.units import cm, mm
from reportlab.lib.colors import HexColor, white, black
from reportlab.pdfgen import canvas as rl_canvas
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether, PageBreak
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.lib.colors import HexColor
OUTPUT = "/home/daytona/workspace/bariatric-refcard/Post_Bariatric_Nursing_Reference_Card.pdf"
PW, PH = landscape(A4)
LM = RM = 0.5 * cm
TM = BM = 0.45 * cm
UW = PW - LM - RM # usable width
# ── Palette ──────────────────────────────────────────────────────────────────
NAVY = HexColor("#1A3A5C")
NAVY_LT = HexColor("#D6E4F0")
RED = HexColor("#C0392B")
RED_LT = HexColor("#FADBD8")
ORANGE = HexColor("#D35400")
ORG_LT = HexColor("#FAE5D3")
GREEN = HexColor("#1E8449")
GRN_LT = HexColor("#D5F5E3")
TEAL = HexColor("#148F77")
TEA_LT = HexColor("#D1F2EB")
PURPLE = HexColor("#6C3483")
PUR_LT = HexColor("#E8DAEF")
GOLD = HexColor("#B7950B")
GOLD_LT = HexColor("#FCF3CF")
GRAY_D = HexColor("#5D6D7E")
GRAY_L = HexColor("#F2F3F4")
BORDER = HexColor("#BDC3C7")
CRIMSON = HexColor("#922B21")
TEAL2 = HexColor("#0E6655")
SKY = HexColor("#2E86C1")
SKY_LT = HexColor("#AED6F1")
# ── Style helpers ─────────────────────────────────────────────────────────────
def S(name, **kw):
return ParagraphStyle(name, **kw)
TITLE = S("T", fontName="Helvetica-Bold", fontSize=16, textColor=white,
alignment=TA_CENTER, leading=20)
SUB = S("SU", fontName="Helvetica", fontSize=9, textColor=HexColor("#AED6F1"),
alignment=TA_CENTER, leading=12)
SH = S("SH", fontName="Helvetica-Bold", fontSize=9.5, textColor=white,
alignment=TA_LEFT, leading=12)
BODY = S("B", fontName="Helvetica", fontSize=8.5, textColor=black, leading=11)
BODYB = S("BB", fontName="Helvetica-Bold", fontSize=8.5, textColor=black, leading=11)
SMALL = S("SM", fontName="Helvetica", fontSize=7.8, textColor=black, leading=10.5)
SMALLB = S("SMB", fontName="Helvetica-Bold", fontSize=7.8, textColor=black, leading=10.5)
TINY = S("TI", fontName="Helvetica", fontSize=7, textColor=GRAY_D, leading=9.5)
TINYB = S("TIB", fontName="Helvetica-Bold", fontSize=7, textColor=black, leading=9.5)
FOOT = S("FO", fontName="Helvetica-Oblique", fontSize=6.8, textColor=GRAY_D,
alignment=TA_CENTER)
def spacer(h=4):
return Spacer(1, h)
# ── Layout helpers ────────────────────────────────────────────────────────────
def banner(text, subtext, bg, UW):
data = [
[Paragraph(text, TITLE)],
[Paragraph(subtext, SUB)],
]
t = Table(data, colWidths=[UW])
t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), bg),
("TOPPADDING", (0,0),(-1,0), 10),
("BOTTOMPADDING",(0,1),(-1,1), 8),
("ROWPADDING", (0,0),(-1,-1), 3),
]))
return t
def sec_hdr(text, bg, UW):
t = Table([[Paragraph(text, SH)]], colWidths=[UW])
t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), bg),
("ROWPADDING", (0,0),(-1,-1), 5),
("LEFTPADDING",(0,0),(-1,-1), 8),
]))
return t
def comp_table(rows, col_widths, hdr_bg):
"""rows[0] = header row (strings), rows[1:] = data rows (Paragraphs or strings)."""
t = Table(rows, colWidths=col_widths)
n = len(rows)
style = [
# Header
("BACKGROUND", (0,0),(-1,0), hdr_bg),
("TEXTCOLOR", (0,0),(-1,0), white),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0),(-1,0), 8),
("ALIGN", (0,0),(-1,0), "CENTER"),
# Body
("FONTSIZE", (0,1),(-1,-1), 7.8),
("ROWPADDING", (0,0),(-1,-1), 4),
("LEFTPADDING", (0,0),(-1,-1), 5),
("RIGHTPADDING",(0,0),(-1,-1), 4),
("VALIGN", (0,0),(-1,-1), "TOP"),
("GRID", (0,0),(-1,-1), 0.4, BORDER),
]
for i in range(1, n):
bg = GRAY_L if i % 2 == 0 else white
style.append(("BACKGROUND", (0,i),(-1,i), bg))
t.setStyle(TableStyle(style))
return t
def highlight_box(text_para, bg, border_color, UW):
t = Table([[text_para]], colWidths=[UW])
t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), bg),
("BOX", (0,0),(-1,-1), 1.5, border_color),
("ROWPADDING", (0,0),(-1,-1), 7),
("LEFTPADDING", (0,0),(-1,-1), 10),
("RIGHTPADDING",(0,0),(-1,-1), 10),
]))
return t
# ═══════════════════════════════════════════════════════════════════════════════
# BUILD DOCUMENT
# ═══════════════════════════════════════════════════════════════════════════════
doc = SimpleDocTemplate(
OUTPUT,
pagesize=landscape(A4),
leftMargin=LM, rightMargin=RM,
topMargin=TM, bottomMargin=BM,
)
story = []
# ════════════════════════════════════════════════════════════════
# PAGE 1 — EARLY / ACUTE COMPLICATIONS
# ════════════════════════════════════════════════════════════════
story.append(banner(
"POST-BARIATRIC SURGERY: NURSING COMPLICATIONS & INTERVENTIONS",
"Page 1 of 2 — Early & Acute Complications | MS III Medical-Surgical Nursing | Unit 11 Metabolic & Endocrine",
NAVY, UW
))
story.append(spacer(6))
# ── Procedure reminder strip ──────────────────────────────────
proc_data = [
["PROCEDURE", "TYPE", "MECHANISM", "KEY RISK"],
[Paragraph("<b>Roux-en-Y Gastric Bypass (RYGB)</b>", SMALLB),
Paragraph("Restrictive + Malabsorptive", SMALL),
Paragraph("Small pouch + bypasses jejunum", SMALL),
Paragraph("<font color='#C0392B'><b>Dumping, anastomotic leak, nutritional deficiencies</b></font>", SMALL)],
[Paragraph("<b>Sleeve Gastrectomy</b>", SMALLB),
Paragraph("Restrictive only", SMALL),
Paragraph("75-80% stomach removed; lowers ghrelin", SMALL),
Paragraph("<font color='#D35400'><b>Staple line leak, worsening GERD</b></font>", SMALL)],
[Paragraph("<b>Adjustable Gastric Band</b>", SMALLB),
Paragraph("Restrictive only", SMALL),
Paragraph("Adjustable band limits intake", SMALL),
Paragraph("<font color='#148F77'><b>Band slippage, erosion, port infection</b></font>", SMALL)],
[Paragraph("<b>BPD with Duodenal Switch</b>", SMALLB),
Paragraph("Restrictive + Malabsorptive", SMALL),
Paragraph("Most aggressive restriction + malabsorption", SMALL),
Paragraph("<font color='#922B21'><b>HIGHEST nutritional deficiency risk</b></font>", SMALL)],
]
proc_w = [UW*0.25, UW*0.17, UW*0.28, UW*0.30]
proc_t = comp_table(proc_data, proc_w, NAVY)
story += [proc_t, spacer(6)]
# ── Early complications section header ───────────────────────
story.append(sec_hdr("EARLY / ACUTE COMPLICATIONS (hours to days post-op)", RED, UW))
story.append(spacer(4))
# Table: early complications
E_HDR = ["COMPLICATION", "TIMING", "SIGNS & SYMPTOMS", "NURSING ASSESSMENT", "INTERVENTIONS", "ESCALATE IF"]
early_comps = [
[
Paragraph("<b>Anastomotic / Staple\nLine LEAK</b>", SMALLB),
Paragraph("24 hrs – 5 days", SMALL),
Paragraph("Tachycardia (HR >120) is EARLIEST sign\nFever, severe abdominal pain\nLeft shoulder pain (diaphragm irritation)\nDiaphoresis, restlessness, anxiety", SMALL),
Paragraph("Vital signs q1-2h\nPain intensity & location\nDrain output (character, volume)\nO2 saturation", SMALL),
Paragraph("Keep NPO\nNotify surgeon STAT\nIV fluids; O2 therapy\nPrepare for CT / return to OR\nDocument drain output", SMALL),
Paragraph("<font color='#C0392B'><b>HR >120 bpm\nT >38.5°C\nSudden pain increase\nDrain output change</b></font>", SMALL),
],
[
Paragraph("<b>Pulmonary\nComplications</b>\n(Atelectasis, Pneumonia,\nRespiratory Failure)", SMALLB),
Paragraph("24–72 hrs", SMALL),
Paragraph("Hypoxia (SpO2 <94%)\nIncreased RR, dyspnea\nFever 24-48 hrs post-op\nDecreased breath sounds\nInability to use incentive spirometer", SMALL),
Paragraph("SpO2 & RR monitoring\nLung auscultation q4-8h\nIncentive spirometry use\nAmbulation progress\nCPAP compliance (OSA patients)", SMALL),
Paragraph("HOB 30-45° at all times\nIncentive spirometry q1-2h\nDeep breathing exercises\nEnsure CPAP for OSA patients\nEarly ambulation\nAdequate pain control (enables breathing)", SMALL),
Paragraph("<font color='#C0392B'><b>SpO2 <92%\nRR >24\nAccessory muscle use\nCyanosis</b></font>", SMALL),
],
[
Paragraph("<b>Venous\nThromboembolism\n(DVT / PE)</b>", SMALLB),
Paragraph("Days 1-30\n(peak Days 3-7)", SMALL),
Paragraph("DVT: calf pain, swelling, Homan's sign (unreliable)\nPE: sudden dyspnea, pleuritic chest pain,\ntachycardia, hypoxia, hemoptysis\nSudden collapse / cardiovascular collapse (massive PE)", SMALL),
Paragraph("Calf assessment daily\nVital signs trend\nLeg pain / swelling comparison\nMonitor anticoagulation levels\nNote immobility duration", SMALL),
Paragraph("SCDs on lower extremities\nAnticoagulation as ordered\nEarly ambulation (Day 1 if possible)\nAdequate hydration\nTeach patient to report leg pain / dyspnea\nDo NOT massage calf if DVT suspected", SMALL),
Paragraph("<font color='#C0392B'><b>Sudden dyspnea\nChest pain\nDesaturation\nSyncope</b></font>", SMALL),
],
[
Paragraph("<b>Bleeding /\nHemorrhage</b>", SMALLB),
Paragraph("Intraoperative\n– 48 hrs", SMALL),
Paragraph("Tachycardia, hypotension\nDecreased urine output\nPale, diaphoretic skin\nDrain: bright red / large volume\nDecreasing Hgb/Hct", SMALL),
Paragraph("VS trend (MAP, HR)\nDrain output color & volume\nSerial Hgb/Hct\nUrine output (>0.5 mL/kg/hr)\nAbdominal girth", SMALL),
Paragraph("IV access x2 large bore\nFluid resuscitation as ordered\nBlood products if ordered\nTransfusion preparation\nNotify surgeon immediately", SMALL),
Paragraph("<font color='#C0392B'><b>SBP <90\nHR >110\nUO <30 mL/hr\nBright red drain\nHgb drop</b></font>", SMALL),
],
[
Paragraph("<b>Wound\nInfection /\nDehiscence</b>", SMALLB),
Paragraph("Days 3-10", SMALL),
Paragraph("Redness, warmth, swelling at incision\nPurulent or malodorous drainage\nFever, elevated WBC\nWound edges separating\nIncreasing pain at wound site", SMALL),
Paragraph("Inspect incisions each shift\nAssess drainage: amount, character\nTemperature & WBC trend\nBlood glucose (hyperglycemia impairs healing)\nSkin fold assessment", SMALL),
Paragraph("Aseptic wound care\nMoisture management\nHyperglycemia correction\nAntibiotics as ordered\nNutritional support\nWound care team consult PRN", SMALL),
Paragraph("<font color='#C0392B'><b>Fever >38.5°C\nFascia visible\nWound dehiscence\nRapidly expanding\nerythema</b></font>", SMALL),
],
]
E_W = [UW*0.13, UW*0.085, UW*0.19, UW*0.165, UW*0.195, UW*0.135]
hdr_row = [Paragraph(h, S(f"EH{i}", fontName="Helvetica-Bold", fontSize=7.8, textColor=white,
alignment=TA_CENTER, leading=10))
for i, h in enumerate(E_HDR)]
e_rows = [hdr_row] + early_comps
e_tbl = Table(e_rows, colWidths=E_W)
e_style = [
("BACKGROUND", (0,0),(-1,0), RED),
("TEXTCOLOR", (0,0),(-1,0), white),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("ALIGN", (0,0),(-1,0), "CENTER"),
("ROWPADDING", (0,0),(-1,-1), 4),
("LEFTPADDING", (0,0),(-1,-1), 5),
("RIGHTPADDING",(0,0),(-1,-1), 4),
("VALIGN", (0,0),(-1,-1), "TOP"),
("GRID", (0,0),(-1,-1), 0.4, BORDER),
("BACKGROUND", (0,1),(-1,1), RED_LT),
("BACKGROUND", (0,2),(-1,2), white),
("BACKGROUND", (0,3),(-1,3), RED_LT),
("BACKGROUND", (0,4),(-1,4), white),
("BACKGROUND", (0,5),(-1,5), RED_LT),
("FONTNAME", (0,1),(0,-1), "Helvetica-Bold"),
]
e_tbl.setStyle(TableStyle(e_style))
story += [e_tbl, spacer(5)]
# ── Dumping syndrome highlight ────────────────────────────────
story.append(sec_hdr("DUMPING SYNDROME — Most Common Post-Bariatric Complication", ORANGE, UW))
story.append(spacer(4))
dump_data = [
["", "EARLY DUMPING", "LATE DUMPING"],
[Paragraph("<b>Timing</b>", SMALLB),
Paragraph("15–30 minutes after eating", SMALL),
Paragraph("1–3 hours after eating", SMALL)],
[Paragraph("<b>Mechanism</b>", SMALLB),
Paragraph("Rapid gastric emptying → hyperosmolar chyme\nin jejunum → massive fluid shift into gut\n+ vagal stimulation", SMALL),
Paragraph("Rapid glucose absorption → excessive insulin\nrelease → REACTIVE HYPOGLYCEMIA", SMALL)],
[Paragraph("<b>Symptoms</b>", SMALLB),
Paragraph("Nausea, vomiting, cramping, explosive diarrhea\nFlushing, diaphoresis, palpitations\nDizziness, near-syncope", SMALL),
Paragraph("Weakness, diaphoresis, tremor, anxiety\nPalpitations, confusion, blurred vision\nSyncope (severe)", SMALL)],
[Paragraph("<b>Triggers</b>", SMALLB),
Paragraph("High-sugar foods, high-fat foods\nHigh-calorie liquids", SMALL),
Paragraph("Simple carbohydrates, sugar\nHigh glycaemic index foods", SMALL)],
[Paragraph("<b>Nursing\nInterventions</b>", SMALLB),
Paragraph("Teach: no sugar/high-fat foods\nSeparate liquids from solids (30 min)\nSmall frequent meals\nLie down 30 min after meals\nMonitor VS during episode", SMALL),
Paragraph("Check blood glucose during symptoms\nTeach to recognize hypoglycemia\nGive 15g fast carb if glucose <70\nAcarbose (if ordered) slows absorption\nDietary consult", SMALL)],
[Paragraph("<b>Medical\nTreatment</b>", SMALLB),
Paragraph("Dietary modification (first-line)\nOctreotide 25–100 mcg SC pre-meals\n(retards intestinal transit)", SMALL),
Paragraph("Dietary modification (first-line)\nAcarbose (slows carb absorption)\nOctreotide for refractory cases", SMALL)],
]
dump_w = [UW*0.12, UW*0.44, UW*0.44]
dump_t = Table(dump_data, colWidths=dump_w)
dump_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,0), ORANGE),
("TEXTCOLOR", (0,0),(-1,0), white),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("ALIGN", (0,0),(-1,0), "CENTER"),
("FONTSIZE", (0,0),(-1,0), 8.5),
("BACKGROUND", (1,0),(1,0), HexColor("#B7390A")),
("BACKGROUND", (2,0),(2,0), HexColor("#D35400")),
("ROWPADDING", (0,0),(-1,-1), 4),
("LEFTPADDING", (0,0),(-1,-1), 5),
("GRID", (0,0),(-1,-1), 0.4, BORDER),
("VALIGN", (0,0),(-1,-1), "TOP"),
("BACKGROUND", (0,1),(-1,1), ORG_LT),
("BACKGROUND", (0,2),(-1,2), white),
("BACKGROUND", (0,3),(-1,3), ORG_LT),
("BACKGROUND", (0,4),(-1,4), white),
("BACKGROUND", (0,5),(-1,5), ORG_LT),
("BACKGROUND", (0,6),(-1,6), white),
("FONTNAME", (0,1),(0,-1), "Helvetica-Bold"),
]))
story += [dump_t, spacer(5)]
# ── Footer page 1 ─────────────────────────────────────────────
story.append(HRFlowable(width=UW, thickness=0.4, color=GRAY_D))
story.append(spacer(2))
story.append(Paragraph(
"Post-Bariatric Surgery Nursing Reference Card | Page 1 of 2 | "
"Sources: Goldman-Cecil Medicine, Sleisenger & Fordtran GI Disease, "
"Miller's Anesthesia 10e, Harrison's Principles 22e",
FOOT))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════
# PAGE 2 — LATE / CHRONIC COMPLICATIONS + DIET + SUPPLEMENTS
# ════════════════════════════════════════════════════════════════
story.append(banner(
"POST-BARIATRIC SURGERY: LATE COMPLICATIONS, DIET PROGRESSION & SUPPLEMENTATION",
"Page 2 of 2 — Late/Chronic Complications | Dietary Phases | Lifelong Supplementation | Patient Education",
TEAL, UW
))
story.append(spacer(6))
# ── Late complications ────────────────────────────────────────
story.append(sec_hdr("LATE / CHRONIC COMPLICATIONS (weeks to years post-op)", TEAL, UW))
story.append(spacer(4))
L_HDR = ["COMPLICATION", "TIME FRAME", "SIGNS & SYMPTOMS", "NURSING ASSESSMENT", "INTERVENTIONS"]
late_comps = [
[
Paragraph("<b>Nutritional\nDeficiencies</b>", SMALLB),
Paragraph("Months to years\n(lifelong risk)", SMALL),
Paragraph("B12: fatigue, glossitis, peripheral neuropathy, macrocytic anemia\n"
"Iron: fatigue, pallor, brittle nails, hair loss, microcytic anemia\n"
"Calcium/Vit D: bone pain, muscle cramps, tetany, osteoporosis\n"
"Folate: anemia, neural tube defects (pregnancy)\n"
"Thiamine (B1): Wernicke encephalopathy (confusion, ataxia, nystagmus)", SMALL),
Paragraph("Annual CBC, iron studies, B12, folate\nCalcium, Vit D, PTH levels\nThiamine if vomiting present\nBone density (DEXA) per protocol\nNeuro exam (B12 deficiency)\nHair, nail, skin assessment", SMALL),
Paragraph("Reinforce LIFELONG supplementation\nCalcium CITRATE (not carbonate) — requires no acid\nB12 sublingually or IM if needed (bypassed intrinsic factor)\nReferral to dietitian\nTeach: supplement with meals vs. separate from iron", SMALL),
],
[
Paragraph("<b>Weight Regain</b>", SMALLB),
Paragraph("Years 2-5+\n(common without\nbehavior change)", SMALL),
Paragraph("Progressive weight gain after initial loss\nReturn of obesity-related comorbidities\nResuming old eating patterns\nPsychological distress, self-blame", SMALL),
Paragraph("Track weight at every visit\nDietary recall assessment\nActivity level evaluation\nPsychological wellbeing screen\nSupport system assessment", SMALL),
Paragraph("Nonjudgmental approach — weight regain is common\nReinforce behavioral strategies\nDietitian / behavioral health referral\nConsider medication adjunct\nRevisional surgery in selected cases\nAddress psychological factors (depression, binge eating)", SMALL),
],
[
Paragraph("<b>Marginal Ulcer\n(Anastomotic ulcer)</b>", SMALLB),
Paragraph("Months to years\n(RYGB specific)", SMALL),
Paragraph("Epigastric or abdominal pain\nNausea, vomiting\nGI bleeding (hematemesis, melena)\nIron-deficiency anemia", SMALL),
Paragraph("Pain assessment (type, location)\nStool for occult blood\nHgb/Hct trend\nNSAID and smoking use history\n(major risk factors)", SMALL),
Paragraph("Strict: NO NSAIDs (use acetaminophen only)\nStop smoking (vasoconstiction impairs healing)\nPPI therapy as prescribed\nEndoscopy referral if suspected\nMucosa-protecting medications", SMALL),
],
[
Paragraph("<b>GERD / Reflux\nWorsening</b>", SMALLB),
Paragraph("Months to years\n(Sleeve gastrectomy\nspecific risk)", SMALL),
Paragraph("Heartburn, regurgitation\nChest pain, chronic cough\nBarrett's esophagus risk long-term\nWorstening after sleeve gastrectomy\n(RYGB often improves GERD)", SMALL),
Paragraph("Symptom severity screening\nMedication effectiveness\nHOB elevation at night\nDietary triggers review\n(caffeine, alcohol, fatty foods)", SMALL),
Paragraph("PPI therapy as ordered\nDietary modification: avoid triggers\nElevate HOB 30-45° for sleep\nAvoid eating 3 hrs before bed\nEndoscopy if symptoms persist\nConversion from sleeve to RYGB (selected patients)", SMALL),
],
[
Paragraph("<b>Dumping Syndrome\n(Chronic)</b>", SMALLB),
Paragraph("Can persist long-term\n(most improve\nwith diet changes)", SMALL),
Paragraph("See Page 1 — Dumping Syndrome\nChronic: reactive hypoglycemia\nmay be dominant presentation\nWeight loss plateau or worsening", SMALL),
Paragraph("Blood glucose diary\nFood-symptom diary\nWeight trend\nNutritional adequacy\nQuality of life assessment", SMALL),
Paragraph("Continuous dietary counseling\nAvoid simple sugars lifelong\nOctreotide PRN or scheduled\nEndocrinology referral for refractory hypoglycemia\nAcarbose for late dumping", SMALL),
],
[
Paragraph("<b>Psychological\nAdjustment /\nBody Image", SMALLB),
Paragraph("Ongoing\n(months to years)", SMALL),
Paragraph("Depression, anxiety (common post-op)\nBody image dissatisfaction\nSubstance use (alcohol transfer addiction)\nRelationship changes\nUnrealistic weight expectations", SMALL),
Paragraph("PHQ-9 depression screening\nAnxiety screening\nAlcohol/substance use screen\nBody image and self-esteem\nSocial support assessment", SMALL),
Paragraph("Normalize psychological adjustment\nReferral to behavioral health\nSupport group recommendation\nScreen for alcohol use disorder\n(alcohol absorbed faster post-RYGB)\nAddress body dysmorphia", SMALL),
],
[
Paragraph("<b>Gallstone\nFormation</b>", SMALLB),
Paragraph("First 6-12 months\n(rapid weight loss\nperiod)", SMALL),
Paragraph("Right upper quadrant pain\nNausea after fatty meals\nFever if cholecystitis\nJaundice if CBD obstruction", SMALL),
Paragraph("RUQ pain assessment\nPain with fatty food intake\nFever and jaundice monitoring\nLFT trend", SMALL),
Paragraph("Prophylactic ursodiol 300mg BID\n(for 6 months, standard of care)\nDietary fat modification\nUltrasound if symptoms present\nSurgery if symptomatic stones", SMALL),
],
]
L_W = [UW*0.14, UW*0.10, UW*0.22, UW*0.18, UW*0.26]
hdr_row_l = [Paragraph(h, S(f"LH{i}", fontName="Helvetica-Bold", fontSize=8,
textColor=white, alignment=TA_CENTER, leading=10))
for i, h in enumerate(L_HDR)]
l_rows = [hdr_row_l] + late_comps
l_tbl = Table(l_rows, colWidths=L_W)
l_style = [
("BACKGROUND", (0,0),(-1,0), TEAL),
("TEXTCOLOR", (0,0),(-1,0), white),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("ALIGN", (0,0),(-1,0), "CENTER"),
("ROWPADDING", (0,0),(-1,-1), 4),
("LEFTPADDING", (0,0),(-1,-1), 5),
("RIGHTPADDING",(0,0),(-1,-1), 4),
("VALIGN", (0,0),(-1,-1), "TOP"),
("GRID", (0,0),(-1,-1), 0.4, BORDER),
("FONTNAME", (0,1),(0,-1), "Helvetica-Bold"),
]
for i in range(1, len(l_rows)):
bg = TEA_LT if i % 2 != 0 else white
l_style.append(("BACKGROUND", (0,i),(-1,i), bg))
l_tbl.setStyle(TableStyle(l_style))
story += [l_tbl, spacer(6)]
# ── Bottom two-column: Diet progression + Supplements ────────
COL_W = UW * 0.48
GAP_W = UW * 0.04
# ── LEFT: Dietary progression ────────────────────────────────
diet_phases = [
["PHASE", "TIMING", "ALLOWED FOODS", "KEY RULES"],
[Paragraph("<b>1\nClear\nLiquids</b>", TINYB),
Paragraph("Days 1–2", TINY),
Paragraph("Water, broth, sugar-free\npopsicles, clear juice,\ndiluted herbal tea", TINY),
Paragraph("Sip slowly (1–2 oz at a time)\nNo carbonation EVER\nStay hydrated: 48–64 oz/day", TINY)],
[Paragraph("<b>2\nFull Liquids /\nProtein Shakes</b>", TINYB),
Paragraph("Weeks 1–3", TINY),
Paragraph("Protein shakes, milk,\nyogurt (smooth), cream\nsoups (strained)", TINY),
Paragraph("60–80g protein/day target\nSeparate eating & drinking\nNo sugar-added shakes", TINY)],
[Paragraph("<b>3\nPureed</b>", TINYB),
Paragraph("Weeks 3–5", TINY),
Paragraph("Blended protein (eggs,\ncottage cheese, fish)\nSmooth pureed vegetables", TINY),
Paragraph("2–4 oz per meal\nChew thoroughly\nProtein FIRST at every meal", TINY)],
[Paragraph("<b>4\nSoft Foods</b>", TINYB),
Paragraph("Weeks 5–8", TINY),
Paragraph("Soft cooked chicken, fish,\ncanned tuna, soft fruit,\ncooked vegetables", TINY),
Paragraph("Introduce one new food\nat a time\nStop if pain or vomiting", TINY)],
[Paragraph("<b>5\nRegular\nTexture</b>", TINYB),
Paragraph("After\n2 months", TINY),
Paragraph("Most foods allowed\n(portion-controlled forever)\nAvoid: tough meat, bread,\npasta, rice, carbonation", TINY),
Paragraph("Pouch = 4–8 oz capacity\nEat 5–6 small meals/day\nNO sugar, NO carbonation\nAlcohol absorbed faster: CAUTION", TINY)],
]
diet_col_w = [COL_W*0.10, COL_W*0.14, COL_W*0.40, COL_W*0.46]
diet_t = Table(diet_phases, colWidths=diet_col_w)
diet_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,0), PURPLE),
("TEXTCOLOR", (0,0),(-1,0), white),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0),(-1,0), 7.5),
("ALIGN", (0,0),(-1,0), "CENTER"),
("ROWPADDING", (0,0),(-1,-1), 3),
("LEFTPADDING", (0,0),(-1,-1), 4),
("GRID", (0,0),(-1,-1), 0.4, BORDER),
("VALIGN", (0,0),(-1,-1), "TOP"),
("BACKGROUND", (0,1),(-1,1), PUR_LT),
("BACKGROUND", (0,2),(-1,2), white),
("BACKGROUND", (0,3),(-1,3), PUR_LT),
("BACKGROUND", (0,4),(-1,4), white),
("BACKGROUND", (0,5),(-1,5), PUR_LT),
("FONTNAME", (0,1),(0,-1), "Helvetica-Bold"),
]))
diet_section = [
sec_hdr("DIETARY PROGRESSION PHASES", PURPLE, COL_W),
spacer(3),
diet_t,
]
# ── RIGHT: Lifelong supplements ───────────────────────────────
supp_data = [
["SUPPLEMENT", "FORM / DOSE", "DEFICIENCY CONSEQUENCE", "NURSING PEARL"],
[Paragraph("<b>Multivitamin</b>", TINYB),
Paragraph("Chewable or liquid\n2x/day (bypass)\n1x/day (sleeve)", TINY),
Paragraph("Multiple micronutrient\ndeficiencies", TINY),
Paragraph("Must be chewable or\nliquid — tablets not\nabsorbed post-RYGB", TINY)],
[Paragraph("<b>Calcium\nCITRATE</b>", TINYB),
Paragraph("1200–1500 mg/day\nin 500mg doses\n(not all at once)", TINY),
Paragraph("Osteoporosis\nTetany, muscle cramps\nFracture risk", TINY),
Paragraph("<b>CITRATE only</b> — carbonate\nrequires stomach acid\nwhich is reduced post-op\nSeparate from iron by 2h", TINY)],
[Paragraph("<b>Vitamin D</b>", TINYB),
Paragraph("3000 IU/day\n(D3 preferred)", TINY),
Paragraph("Osteomalacia\nHypocalcemia\nBone disease", TINY),
Paragraph("Taken with calcium\nMonitor 25-OH Vit D\nlevel annually", TINY)],
[Paragraph("<b>Vitamin B12</b>", TINYB),
Paragraph("350–500 mcg/day\nSublingual or IM\nif severe", TINY),
Paragraph("Pernicious anemia\nPeripheral neuropathy\nWernicke's (rare)", TINY),
Paragraph("Intrinsic factor\nreduced after bypass\nSublingual bypasses\nGI absorption issue", TINY)],
[Paragraph("<b>Iron</b>", TINYB),
Paragraph("45–60 mg elemental\niron/day\n(menstruating women\nneed more)", TINY),
Paragraph("Iron-deficiency anemia\nFatigue, pallor\nHair loss, brittle nails", TINY),
Paragraph("Take with vitamin C\n(enhances absorption)\nSeparate from calcium\nby at least 2 hours", TINY)],
[Paragraph("<b>Folate</b>", TINYB),
Paragraph("400–800 mcg/day\n(higher in pregnancy)", TINY),
Paragraph("Megaloblastic anemia\nNeural tube defects\n(critical in pregnancy)", TINY),
Paragraph("All women of\nchildbearing age need\nadequate folate\nMonitor in pregnancy", TINY)],
[Paragraph("<b>Thiamine (B1)</b>", TINYB),
Paragraph("12 mg/day in multi\nSupplement if vomiting\nor neurologic Sx", TINY),
Paragraph("Wernicke encephalopathy\nConfusion, ataxia\nNystagmus", TINY),
Paragraph("At-risk: prolonged\nvomiting post-op\nIV thiamine if\nWernicke suspected", TINY)],
]
supp_col_w = [COL_W*0.18, COL_W*0.22, COL_W*0.28, COL_W*0.32]
supp_t = Table(supp_data, colWidths=supp_col_w)
supp_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,0), GOLD),
("TEXTCOLOR", (0,0),(-1,0), white),
("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0),(-1,0), 7.5),
("ALIGN", (0,0),(-1,0), "CENTER"),
("ROWPADDING", (0,0),(-1,-1), 3),
("LEFTPADDING", (0,0),(-1,-1), 4),
("GRID", (0,0),(-1,-1), 0.4, BORDER),
("VALIGN", (0,0),(-1,-1), "TOP"),
("BACKGROUND", (0,1),(-1,1), GOLD_LT),
("BACKGROUND", (0,2),(-1,2), white),
("BACKGROUND", (0,3),(-1,3), GOLD_LT),
("BACKGROUND", (0,4),(-1,4), white),
("BACKGROUND", (0,5),(-1,5), GOLD_LT),
("BACKGROUND", (0,6),(-1,6), white),
("BACKGROUND", (0,7),(-1,7), GOLD_LT),
("FONTNAME", (0,1),(0,-1), "Helvetica-Bold"),
# Highlight calcium citrate row
("BACKGROUND", (0,2),(-1,2), HexColor("#FEF9C3")),
("FONTNAME", (0,2),(-1,2), "Helvetica-Bold"),
]))
supp_section = [
sec_hdr("LIFELONG SUPPLEMENTATION (ALL BARIATRIC PATIENTS FOREVER)", GOLD, COL_W),
spacer(3),
supp_t,
]
# ── Arrange left and right columns ───────────────────────────
two_col = Table(
[[diet_section, Spacer(GAP_W, 1), supp_section]],
colWidths=[COL_W, GAP_W, COL_W],
)
two_col.setStyle(TableStyle([
("VALIGN", (0,0),(-1,-1), "TOP"),
("ROWPADDING", (0,0),(-1,-1), 0),
("LEFTPADDING",(0,0),(-1,-1), 0),
("RIGHTPADDING",(0,0),(-1,-1), 0),
]))
story.append(two_col)
story.append(spacer(5))
# ── Patient education strip ───────────────────────────────────
story.append(sec_hdr("KEY PATIENT EDUCATION POINTS — TEACH BEFORE DISCHARGE", NAVY, UW))
story.append(spacer(3))
edu_items = [
("WARNING SIGNS\n(Return to ER)",
"Severe abdominal pain\nHR >100 + sweating\nFever >38.5°C\nVomiting > 24 hrs\nChest pain / dyspnea\nWound opening or pus"),
("DIET RULES\n(Lifelong)",
"NO carbonated beverages\nNO sugar or high-calorie drinks\nSeparate liquids from meals\nProtein first at every meal\nChew thoroughly, eat slowly\nSmall portions always"),
("SUPPLEMENTS\n(Lifelong)",
"Take every day — forever\nCalcium CITRATE (not carbonate)\nB12 sublingual or injection\nTake iron with Vitamin C\nSeparate iron & calcium by 2+ hrs\nReport neuropathy / weakness"),
("ALCOHOL\n(High-Risk Post-op)",
"Absorbed FASTER post-RYGB\n(lower peak blood level needed)\nHigher addiction risk post-op\n('transfer addiction')\nAvoid for 1 yr post-op minimum\nOne drink = higher impairment"),
("MEDICATIONS\n(Post-Bariatric)",
"NO NSAIDs (marginal ulcer risk)\nUse acetaminophen for pain\nMedication absorption changes\nExtended-release may not work\nTell ALL providers about surgery\nCrush or liquid meds when possible"),
("FOLLOW-UP\n(Lifelong)",
"Labs at 3, 6, 12 months, then yearly\nDEXA scan (bone density)\nRegular dietitian visits\nMental health follow-up\nGynecology if planning pregnancy\nWait ≥18 months before pregnancy"),
]
edu_col_w = [(UW - 5*0.2*cm) / 6] * 6
edu_rows = [[Paragraph(f"<b>{title}</b>", S("ET", fontName="Helvetica-Bold", fontSize=7.5,
textColor=white, alignment=TA_CENTER, leading=10)),
*[None]*0]
for title, _ in edu_items]
# Build as a 2-row table (title row + content row)
edu_title_cells = []
edu_body_cells = []
for title, body in edu_items:
edu_title_cells.append(
Paragraph(title, S(f"ET{title}", fontName="Helvetica-Bold", fontSize=7.5,
textColor=white, alignment=TA_CENTER, leading=10)))
edu_body_cells.append(
Paragraph(body, S(f"EB{title}", fontName="Helvetica", fontSize=7,
textColor=black, leading=10)))
edu_t = Table(
[edu_title_cells, edu_body_cells],
colWidths=edu_col_w
)
edu_bg_colors = [NAVY, RED, GOLD, ORANGE, TEAL, PURPLE]
edu_style = [
("ROWPADDING", (0,0),(-1,-1), 4),
("LEFTPADDING", (0,0),(-1,-1), 5),
("RIGHTPADDING",(0,0),(-1,-1), 4),
("GRID", (0,0),(-1,-1), 0.4, BORDER),
("VALIGN", (0,0),(-1,-1), "TOP"),
("BACKGROUND", (0,1),(-1,1), GRAY_L),
]
for col, bg in enumerate(edu_bg_colors):
edu_style.append(("BACKGROUND", (col,0),(col,0), bg))
edu_style.append(("TEXTCOLOR", (col,0),(col,0), white))
edu_t.setStyle(TableStyle(edu_style))
story += [edu_t, spacer(4)]
# ── Footer page 2 ─────────────────────────────────────────────
story.append(HRFlowable(width=UW, thickness=0.4, color=GRAY_D))
story.append(spacer(2))
story.append(Paragraph(
"Post-Bariatric Surgery Nursing Reference Card | Page 2 of 2 | "
"MS III Medical-Surgical Nursing — Unit 11 Metabolic & Endocrine | "
"Sources: Goldman-Cecil Medicine, Harrison's Principles 22e, Sleisenger & Fordtran GI Disease, "
"Miller's Anesthesia 10e, Fuster & Hurst's The Heart 15e",
FOOT))
# ── Build ─────────────────────────────────────────────────────
doc.build(story)
print("PDF saved:", OUTPUT)
cd /home/daytona/workspace/bariatric-refcard && python3 generate_refcard.py 2>&1
~/bariatric-refcard/generate_refcard.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/bariatric-refcard/generate_refcard.py'
cd /home/daytona/workspace/bariatric-refcard && python3 generate_refcard.py 2>&1
ls -lh /home/daytona/workspace/bariatric-refcard/
Post Bariatric Nursing Reference Card
PDF Document · PDF
Page 1 — Early & Acute Complications (A4 Landscape)
| Complication | Timing | Signs & Symptoms | Nursing Assessment | Interventions | Escalate If |
|---|---|---|---|---|---|
| Anastomotic/Staple Line Leak | 24h–5 days | Tachycardia HR>120 (EARLIEST sign), fever, left shoulder pain | q1-2h VS, drain output | NPO, notify surgeon STAT | HR >120, fever, sudden pain |
| Pulmonary complications | 24–72h | Hypoxia, decreased breath sounds | SpO2, lung auscultation, CPAP compliance | HOB 30-45°, incentive spirometry q1-2h | SpO2 <92%, RR >24 |
| VTE (DVT/PE) | Days 1–30 | Calf pain, sudden dyspnea, tachycardia | Daily calf assessment, anticoagulation levels | SCDs, early ambulation Day 1 | Sudden dyspnea, chest pain |
| Bleeding/Hemorrhage | Intraop–48h | Tachycardia, hypotension, decreased UO | VS trend, drain color/volume, Hgb/Hct | IV access ×2, fluid resuscitation | SBP <90, UO <30 mL/hr |
| Wound Infection/Dehiscence | Days 3–10 | Redness, purulent drainage, fever | Inspect each shift, glucose monitoring | Aseptic wound care, hyperglycemia correction | Fascia visible, rapidly expanding erythema |
Page 2 — Late Complications, Diet Progression & Supplementation (A4 Landscape)
- LEFT - Dietary Progression Phases: All 5 phases (clear liquids → full liquids → pureed → soft → regular) with timing, allowed foods, and key rules per phase
- RIGHT - Lifelong Supplementation: All 7 supplements (multivitamin, calcium CITRATE, vitamin D, B12, iron, folate, thiamine) with form/dose, deficiency consequence, and nursing pearl — calcium citrate row highlighted in yellow
“Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Also synthesis additional information from other sources pertinent to this chapter that are important for me to know as a nurse. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_49__ASSESSMENT_AND_MANAGEMENT_OF_PATIENTS_WITH_HEPATIC_DISORDERS_.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
What Was Taught (10 Full Sections)
- Jaundice - 3 types (pre-hepatic, hepatocellular, obstructive) with stool/urine color differences
- Portal hypertension - the clogged highway analogy; what backs up and where
- Ascites - SAAG explained, SBP diagnostic criterion (PMN ≥250), treatment with albumin to prevent hepatorenal syndrome
- Esophageal varices - the full emergency cascade: octreotide → endoscopy → TIPS, and why TIPS worsens encephalopathy
- Hepatic encephalopathy - all 5 grades, asterixis testing, lactulose dosing targets, why ammonia level is unreliable
“Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Also synthesis additional information from other sources pertinent to this chapter that are important for me to know as a nurse. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_50__ASSESSMENT_AND_MANAGEMENT_OF_PATIENTS_WITH_BILIARY_DISORDERS.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
What Was Taught
“Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Also synthesis additional information from other sources pertinent to this chapter that are important for me to know as a nurse. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_51__ASSESSMENT_AND_MANAGEMENT_OF_PATIENTS_WITH_DIABETES.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
What Was Taught
“Act as a world-class educator and teach me this chapter from absolute basics to complete mastery. First give me a simple overview of the chapter, then break it into small sections and explain each concept in easy language with examples. Also synthesis additional information from other sources pertinent to this chapter that are important for me to know as a nurse. Connect all topics together and create a final summary that helps me revise the entire chapter quickly before exams.”
cd /home/daytona/workspace/attachments/08d90756-434c-4004-9a60-02bd5a701dbd/ && python3 -c " import pdfplumber with pdfplumber.open('CHAPTER_52__ASSESSMENT_AND_MANAGEMENT_OF_PATIENTS_WITH_ENDOCRINE_DISORDERS.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text) print() "
What Was Taught
UNIT 16/ CHAPTER 65: ASSESSMENT OF NEUROLOGIC FUNCTION Learning Objectives By the end of this module, students should be able to: 1. Describe the structures and functions of the central and peripheral nervous systems. 2. Differentiate between pathologic changes affecting motor control and those affecting sensory pathways. 3. Compare and contrast the functions of the sympathetic and parasympathetic nervous systems. 4. Explain the importance of physical assessment in the diagnosis of neurologic dysfunction. 5. Identify age-related changes in neurologic function and their effects on neurologic assessment findings. 6. Discuss diagnostic tests used in the evaluation of suspected neurologic disorders and the associated nursing implications. Lesson Content I. OVERVIEW OF NEUROLOGIC FUNCTION · The nervous system is the body’s primary control and communication system. · It coordinates: o Sensory input o Motor responses o Cognitive processes o Autonomic regulation · Neurologic assessment is essential because: o Many neurologic disorders progress rapidly o Early changes may be subtle o Delayed recognition can lead to irreversible damage II. STRUCTURES AND FUNCTIONS OF THE CENTRAL AND PERIPHERAL NERVOUS SYSTEMS A. CENTRAL NERVOUS SYSTEM 1. Central nervous system · The central nervous system consists of the brain and spinal cord. · It is responsible for: o Processing sensory information o Initiating motor activity o Regulating consciousness, thought, memory, and emotion B. BRAIN 1. Cerebrum · The cerebrum is the largest portion of the brain. · It is divided into two hemispheres, each containing distinct lobes. a. Frontal lobe · Responsible for: o Voluntary motor activity o Speech production o Judgment, reasoning, and behavior · Damage may result in: o Motor weakness o Personality changes o Impaired speech (expressive aphasia) b. Parietal lobe · Responsible for: o Sensory perception o Spatial orientation · Damage may cause: o Loss of sensation o Inability to recognize objects by touch c. Temporal lobe · Responsible for: o Hearing o Memory o Language comprehension · Damage may cause: o Memory deficits o Receptive aphasia d. Occipital lobe · Responsible for: o Visual processing · Damage may result in: o Visual field defects o Cortical blindness 2. Diencephalon · Includes the thalamus and hypothalamus. · Thalamus: o Acts as a relay station for sensory impulses. · Hypothalamus: o Regulates temperature, hunger, thirst, and endocrine function. 3. Brainstem · Includes the midbrain, pons, and medulla oblongata. · Controls: o Respiratory and cardiac function o Level of consciousness · Damage can be life-threatening. 4. Cerebellum · Coordinates: o Balance o Posture o Fine motor movement · Cerebellar dysfunction causes: o Ataxia o Tremors o Poor coordination C. SPINAL CORD · The spinal cord conducts impulses between the brain and peripheral nerves. · It also mediates reflex activity. · Injury may result in: o Motor paralysis o Sensory loss o Autonomic dysfunction D. PERIPHERAL NERVOUS SYSTEM 1. Peripheral nervous system · Composed of: o Cranial nerves o Spinal nerves · Divided into: o Somatic nervous system o Autonomic nervous system 2. Somatic nervous system · Controls voluntary muscle movement. · Damage results in: o Weakness o Paralysis o Loss of reflexes III. MOTOR AND SENSORY PATHWAYS A. MOTOR PATHWAYS Motor pathways · Carry impulses from the brain to muscles. · Lesions affecting motor pathways cause: o Weakness o Paralysis o Abnormal muscle tone Pathologic changes affecting motor control: · Upper motor neuron lesions o Cause spasticity, hyperreflexia, and loss of voluntary movement. · Lower motor neuron lesions o Cause flaccid paralysis, muscle atrophy, and absent reflexes. B. SENSORY PATHWAYS Sensory pathways · Transmit sensations such as: o Pain o Temperature o Touch o Proprioception Pathologic changes affecting sensory pathways: · Cause: o Numbness o Tingling o Loss of sensation o Abnormal sensations (paresthesia) IV. AUTONOMIC NERVOUS SYSTEM A. Autonomic nervous system · Regulates involuntary body functions. · Divided into: o Sympathetic nervous system o Parasympathetic nervous system B. Sympathetic nervous system · Known as the fight-or-flight system. · Effects include: o Increased heart rate o Dilated pupils o Bronchodilation o Increased blood glucose C. Parasympathetic nervous system · Known as the rest-and-digest system. · Effects include: o Decreased heart rate o Constricted pupils o Increased gastrointestinal activity D. Comparison · These systems act in opposition to maintain homeostasis. · Dysfunction results in: o Blood pressure instability o Abnormal heart rate o Impaired temperature regulation V. SIGNIFICANCE OF PHYSICAL ASSESSMENT IN NEUROLOGIC DIAGNOSIS A. Purpose of Neurologic Assessment · Detect early neurologic dysfunction. · Establish baseline data. · Monitor progression or improvement. B. Components of Neurologic Assessment 1. Level of consciousness · Reflects cerebral function. · Altered consciousness may indicate: o Brain injury o Infection o Metabolic disturbances 2. Cognitive function · Assesses: o Orientation o Memory o Attention o Language 3. Motor function · Muscle strength · Coordination · Gait · Reflexes 4. Sensory function · Pain · Temperature · Touch · Vibration · Position sense VI. AGE-RELATED CHANGES IN NEUROLOGIC FUNCTION A. Normal Aging Changes · Slower nerve conduction · Decreased reflexes · Mild memory decline · Reduced sensory perception B. Impact on Assessment · Findings must be differentiated from disease. · Older adults may: o Respond more slowly o Have diminished vibration and position sense · Increased risk for: o Falls o Delirium o Stroke VII. DIAGNOSTIC TESTS FOR NEUROLOGIC DISORDERS A. Imaging Studies Computed tomography · Identifies hemorrhage, tumors, and structural abnormalities. Magnetic resonance imaging · Provides detailed images of brain and spinal cord tissue. B. Electrical Studies Electroencephalography · Measures electrical activity of the brain. · Used to diagnose seizure disorders. Electromyography · Evaluates muscle and nerve function. C. Cerebrospinal Fluid Analysis Lumbar puncture · Assesses cerebrospinal fluid for: o Infection o Hemorrhage o Inflammatory disorders · Nursing implications: o Monitor for headache o Maintain hydration o Observe neurologic status VIII. NEUROLOGIC ABNORMALITIES: CLINICAL SIGNIFICANCE Aphasia · Language impairment due to cerebral damage. · May be expressive, receptive, or global. Ataxia · Incoordination due to cerebellar dysfunction. Hemiparesis · Weakness on one side of the body. Coma · Prolonged unconsciousness indicating severe brain dysfunction.
What Was Taught
- Why neurologic assessment is urgent (4-6 min window, baseline every shift)
- Nervous system architecture (CNS/PNS/ANS overview)
- Brain anatomy with clinical damage correlations - lobes, diencephalon, brainstem (Cushing's triad, herniation, pupillary patterns, breathing patterns), cerebellum (DANISH)
- Spinal cord - dermatomes, tracts, Brown-Séquard vs. Anterior Cord syndrome
- Motor pathways - UMN vs. LMN with complete comparison table
- Sensory pathways - spinothalamic vs. dorsal columns (the two-pathway model)
- Autonomic NS - full sympathetic vs. parasympathetic table + autonomic dysreflexia + Horner's syndrome
- All 12 cranial nerves - assessment, clinical significance, Bell's vs. stroke CN VII distinction
- Neurologic physical assessment - LOC hierarchy, GCS (with full scale + decorticate/decerebrate), cognitive assessment (AVPU, orientation, delirium vs. dementia), pupillary patterns, motor grading (0-5 scale), pronator drift, sensory testing, DTR grading
- Age-related changes + clinical adaptations
- All diagnostic tests with complete nursing implications (CT, MRI, EEG, EMG/NCS, lumbar puncture with post-LP nursing priority table and full CSF comparison across meningitis/SAH)
- Neurologic abnormality localization table
- Integration framework with cross-chapter connections
- Chapter 66 - Management of Patients with Neurologic Dysfunction (seizures, ICP management, brain herniation, neurosurgical nursing)
- Chapter 67 - Stroke (ischemic vs. hemorrhagic, tPA, NIHSS, nursing care)
- Chapter 68 - Spinal Cord Injury and Degenerative Neurologic Disorders
Chapter 66 - Management of Patients with Neurologic Dysfunction (seizures, ICP management, brain herniation, neurosurgical nursing)
What Was Taught
-
Elevated ICP - Monroe-Kellie doctrine, CPP formula (MAP - ICP), normal values, causes, clinical signs (early vs. late vs. Cushing's triad), EVD nursing with full care priorities (leveling, clamping, CSF assessment), the complete 9-tier management ladder (positioning → mannitol/hypertonic saline → sedation → CSF drainage → surgery)
-
Intracranial Hemorrhage - EDH (biconvex, lucid interval, middle meningeal artery - surgical emergency), SDH (crescent, elderly + anticoagulants, chronic vs. acute), SAH (thunderclap headache, Hunt-Hess grading, the three killers: rebleeding + vasospasm days 4-14 + hydrocephalus, nimodipine q4h × 21 days)
-
Seizures - 2017 ILAE classification (focal aware/impaired/to bilateral; generalized types), phases of tonic-clonic seizure, nursing during a seizure (PROTECT/TIME/POSITION), seizure precautions
-
Status Epilepticus - definition (treat at 5 min for convulsive), full pharmacologic ladder (Tier 1: lorazepam/midazolam → Tier 2: levetiracetam/valproate/fosphenytoin/phenytoin → Tier 3: barbiturate coma), phenytoin rules (NS only, 50 mg/min max, cardiac monitoring, purple glove syndrome), complete AED table
-
Coma Nursing - AEIOU TIPS mnemonic, unconscious patient care across all systems (airway, eyes, mouth, nutrition, skin, bladder/bowel, communication)
-
Neurosurgical Nursing - pre-op priorities, 8 post-craniotomy priority areas, post-op positioning rules (which side depends on procedure type), DI vs. SIADH vs. CSW (the three fluid/sodium disorders), pituitary surgery, VP shunt, complications table
-
Therapeutic Hypothermia - TTM indications, nursing management, shivering control, rewarming protocol
Yes, chapter 67
What Was Taught
-
Pathophysiology - ischemic core vs. penumbra; "time is brain" (1.9 million neurons/min); 5 mechanisms of ischemic stroke (atherosclerosis, cardioembolic, lacunar, cryptogenic, other) and why mechanism determines secondary prevention choice
-
Stroke syndromes by artery territory - complete map with clinical correlations: MCA (face/arm, aphasia vs. neglect, malignant syndrome), ACA (leg > arm, incontinence), PCA (homonymous hemianopsia), Basilar (locked-in syndrome, crossed deficits), PICA/Wallenberg's (the "crossed" syndrome: ipsilateral face + Horner's, contralateral body pain/temp, PRESERVED motor), Lacunar (pure motor/sensory, no cortical signs)
-
TIA - medical emergency, not a minor event; ABCD2 score; 3-5% stroke risk within 48h; urgent workup requirements
-
ICH (hemorrhagic stroke) - causes (HTN #1), locations (putamen most common), clinical presentation, ICH Score, acute management (BP < 140 urgently, anticoagulation reversal chart, cerebellar ICH > 3 cm = surgery)
-
Acute ischemic stroke algorithm - door-to-needle targets, NIHSS full table, tPA complete profile (dose/window/absolute contraindications table), post-tPA nursing protocol, hemorrhagic transformation response
-
Mechanical thrombectomy - the 5 landmark 2015 trials, patient selection, up to 24h window with imaging mismatch, advantages over tPA, post-procedure care
-
BP management - permissive hypertension rationale (allow up to 220/120 for 24-48h in non-tPA patients); glucose management (140-180); temperature
-
Acute stroke nursing care - 8 major complications with nursing responses: dysphagia/aspiration (swallowing screen protocol), DVT, hemorrhagic transformation, cerebral edema/malignant MCA, ICP, seizures, urinary complications, psychological
-
Secondary prevention - antiplatelet vs. anticoagulation decision tree; CHA₂DS₂-VASc score; statin for ALL ischemic stroke; risk factor targets; CEA indications and post-op care
Yes, chapter 68
CHAPTER 69:
What Was Taught
- Bacterial meningitis - organisms by age group (S. pneumoniae adults; N. meningitidis adolescents; Listeria in >50/immunocompromised); CSF analysis master comparison table (bacterial vs. viral vs. TB vs. SAH); Kernig's and Brudzinski's; complete treatment protocol (blood cultures → ceftriaxone + vancomycin ± ampicillin → dexamethasone BEFORE antibiotics); full nursing priorities including droplet precautions; all complications (SIADH, Waterhouse-Friderichsen, DIC, hydrocephalus)
- Viral/aseptic meningitis - enteroviruses; self-limiting; CSF contrast with bacterial
- HSV encephalitis - temporal lobe tropism; behavioral change + temporal lobe seizures; MRI findings; CSF PCR; IV acyclovir 10 mg/kg q8h × 14-21 days; start empirically; acyclovir nursing (q8h timing + hydration for nephrotoxicity)
- Brain abscess - ring-enhancing lesion; LP contraindicated; sources; surgical drainage + 4-8 weeks antibiotics; seizure precautions
CHAPTER 70: MANAGEMENT OF PATIENTS WITH ONCOLOGIC OR DEGENERATIVE NEUROLOGIC DISORDERS Learning Objectives By the end of this module, students should be able to: 1. Describe brain and spinal cord tumors, including their classification, pathophysiology, clinical manifestations, diagnostic methods, and medical and nursing management. 2. Use the nursing process as a framework for caring for patients with primary brain tumors or nervous system metastases. 3. Explain the pathophysiologic mechanisms involved in various neurodegenerative disorders. 4. Apply the nursing process as a framework for providing care to patients with Parkinson disease. 5. Identify available resources for patients and families affected by oncologic and degenerative neurologic disorders. 6. Use the nursing process as a framework for caring for patients after a cervical discectomy. Lesson Content I. OVERVIEW OF ONCOLOGIC AND DEGENERATIVE NEUROLOGIC DISORDERS Oncologic neurologic disorders involve primary or metastatic tumors affecting the brain or spinal cord. Degenerative neurologic disorders involve progressive deterioration of neurons, leading to gradual loss of motor, sensory, or cognitive function. These disorders are often: Chronic and progressive Associated with significant disability Emotionally and physically challenging for patients and families Nursing care focuses on: Early recognition Prevention of complications Functional support Symptom control Psychosocial adaptation II. BRAIN AND SPINAL CORD TUMORS A. CLASSIFICATION OF BRAIN AND SPINAL CORD TUMORS Brain tumors Abnormal growths of cells within the cranial cavity. Classified as: Primary brain tumors – originate from brain tissue or surrounding structures Metastatic brain tumors – spread from cancers elsewhere in the body Spinal cord tumors Tumors located within or surrounding the spinal cord. Classified by location: Intramedullary tumors – arise within the spinal cord Intramedullary tumors – arise within the spinal cord Extramedullary tumors – arise outside the spinal cord but within the dura or vertebral column B. PATHOPHYSIOLOGY Tumors disrupt neurologic function by: Compressing neural tissue Increasing intracranial or intraspinal pressure Altering blood flow and oxygen delivery Tumor growth leads to: Cerebral edema Increased intracranial pressure Herniation risk in brain tumors Spinal cord tumors compress ascending and descending nerve tracts, causing motor and sensory deficits. C. CLINICAL MANIFESTATIONS Brain tumors Headache (often worse in the morning) Nausea and vomiting Altered level of consciousness Seizures Cognitive and personality changes Focal neurologic deficits depending on tumor location Spinal cord tumors Progressive back pain Motor weakness Sensory loss Bowel and bladder dysfunction Gait disturbances D. DIAGNOSTIC EVALUATION Magnetic resonance imaging is the primary diagnostic tool. Computed tomography scanning is useful for detecting hemorrhage and bone involvement. Biopsy confirms tumor type and malignancy. Neurologic assessment establishes baseline function. E. MEDICAL MANAGEMENT Surgical intervention Removal or debulking of tumor when possible Radiation therapy Used for tumor control or palliation Chemotherapy Used depending on tumor type and sensitivity Corticosteroids Reduce cerebral edema Antiseizure medications Prevent or treat seizures F. NURSING MANAGEMENT Monitor neurologic status and signs of increased intracranial pressure. Manage pain, nausea, and seizures. Provide emotional support. Educate patient and family about disease and treatment. Prevent complications related to immobility and therapy. III. NURSING PROCESS: PATIENT WITH PRIMARY BRAIN TUMOR OR NERVOUS SYSTEM METASTASES A. Nursing Assessment Level of consciousness and cognition Motor and sensory function Seizure activity Visual and speech changes Psychosocial response B. Nursing Diagnoses (Common) Impaired physical mobility Risk for injury Disturbed thought processes Acute or chronic pain Anxiety and ineffective coping C. Nursing Interventions Protect patient from injury. Maintain optimal cerebral perfusion. Support mobility and self-care. Provide clear communication and reassurance. Coordinate interdisciplinary care. D. Evaluation Stabilized neurologic status Effective symptom control Improved coping and quality of life IV. NEURODEGENERATIVE DISORDERS A. OVERVIEW OF NEURODEGENERATION Neurodegenerative disorders involve progressive loss of neurons. Damage is typically irreversible and worsens over time. Causes include: Genetic factors Abnormal protein accumulation Neurotransmitter imbalances B. Parkinson Disease Definition Parkinson disease is a chronic, progressive neurodegenerative disorder characterized by dopamine deficiency in the basal ganglia. Pathophysiology Degeneration of dopamine-producing neurons occurs. Dopamine deficiency disrupts balance between excitatory and inhibitory neurotransmitters. Motor control becomes impaired. Clinical Manifestations Resting tremor Bradykinesia (slowness of movement) Rigidity Postural instability Masklike facial expression Shuffling gait Speech and swallowing difficulties Cognitive changes in advanced disease Medical Management Medications that increase dopamine levels or mimic dopamine. Surgical interventions for advanced disease. Physical and occupational therapy. V. NURSING PROCESS: PATIENT WITH PARKINSON DISEASE A. Nursing Assessment Motor function and gait Ability to perform activities of daily living Swallowing and nutrition status Speech clarity Cognitive and emotional status B. Nursing Interventions Promote mobility and prevent falls. Schedule activities during peak medication effectiveness. Assist with feeding and swallowing safety. Encourage communication strategies. Support independence while ensuring safety. C. Evaluation Improved mobility and function Reduced complications Effective medication management Enhanced quality of life VI. RESOURCES FOR PATIENTS AND FAMILIES Community and national organizations supporting neurologic disorders. Rehabilitation services. Home health care. Support groups for patients and caregivers. Palliative and hospice care services when appropriate. Education resources for long-term disease management. VII. NURSING PROCESS: PATIENT FOLLOWING CERVICAL DISCECTOMY A. Cervical discectomy Definition Surgical removal of a damaged intervertebral disc in the cervical spine to relieve nerve compression. B. Postoperative Nursing Assessment Airway patency and respiratory status. Neurologic function of upper and lower extremities. Pain and incision site. Signs of hematoma or spinal cord compression. C. Nursing Interventions Maintain airway and proper neck alignment. Monitor neurologic status frequently. Administer pain medication. Encourage early ambulation as prescribed. Educate on activity restrictions and neck support. D. Evaluation Relief of neurologic symptoms. Stable neurologic function. Absence of complications. Patient understanding of postoperative care.
What Was Taught
- Brain tumor classification - complete WHO grading (I-IV); primary vs. metastatic; all major tumor types with clinical pearls: GBM (Stupp protocol, median survival ~14-16 months), meningioma (most common primary overall, extra-axial, benign, surgery = cure), PCNSL (NO steroids before biopsy), pituitary adenomas (bitemporal hemianopsia, bromocriptine for prolactinoma), acoustic neuroma, medulloblastoma; metastatic primaries ranked (lung > breast > melanoma)
- Pathophysiology and clinical manifestations - three mechanisms (invasion, mass effect, ICP); morning headache pattern explained; focal deficit table by lobe; seizures in 30-50% of primary tumors
- Treatment - surgery (maximal safe resection, awake craniotomy, 5-ALA fluorescence); radiation (fractionated EBRT vs. SRS vs. WBRT with cognitive consequences); complete chemotherapy table (temozolomide, bevacizumab, methotrexate, PCV); dexamethasone rationale and nursing (PPI, glucose, PCP prophylaxis, never stop abruptly)
- Spinal cord tumors - intramedullary/extramedullary/extradural classification; ESCC emergency (back pain in cancer patient = spinal met; dexamethasone IV immediately + urgent MRI + radiation/surgery)
- Nursing process - detailed assessment, 10 nursing diagnoses, 10 priority interventions (neuro monitoring → ICP precautions → seizures → falls → airway → pain → chemo support → communication → nutrition → psychosocial), evaluation criteria