Neuromuscular blocking agents
Reading File
Finding Sources
Searching PubMed
"neuromuscular blocking agents"[MeSH Terms] AND "anesthesia"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed response.
Neuromuscular Blocking Agents (NMBAs)
Overview
NMBAs are highly water-soluble quaternary ammonium compounds that mimic the quaternary ammonium group on the acetylcholine (ACh) molecule. Their water solubility prevents them from crossing the blood-brain barrier or placenta. They are divided into two main classes: depolarizing and nondepolarizing agents.
Normal Neuromuscular Junction Physiology
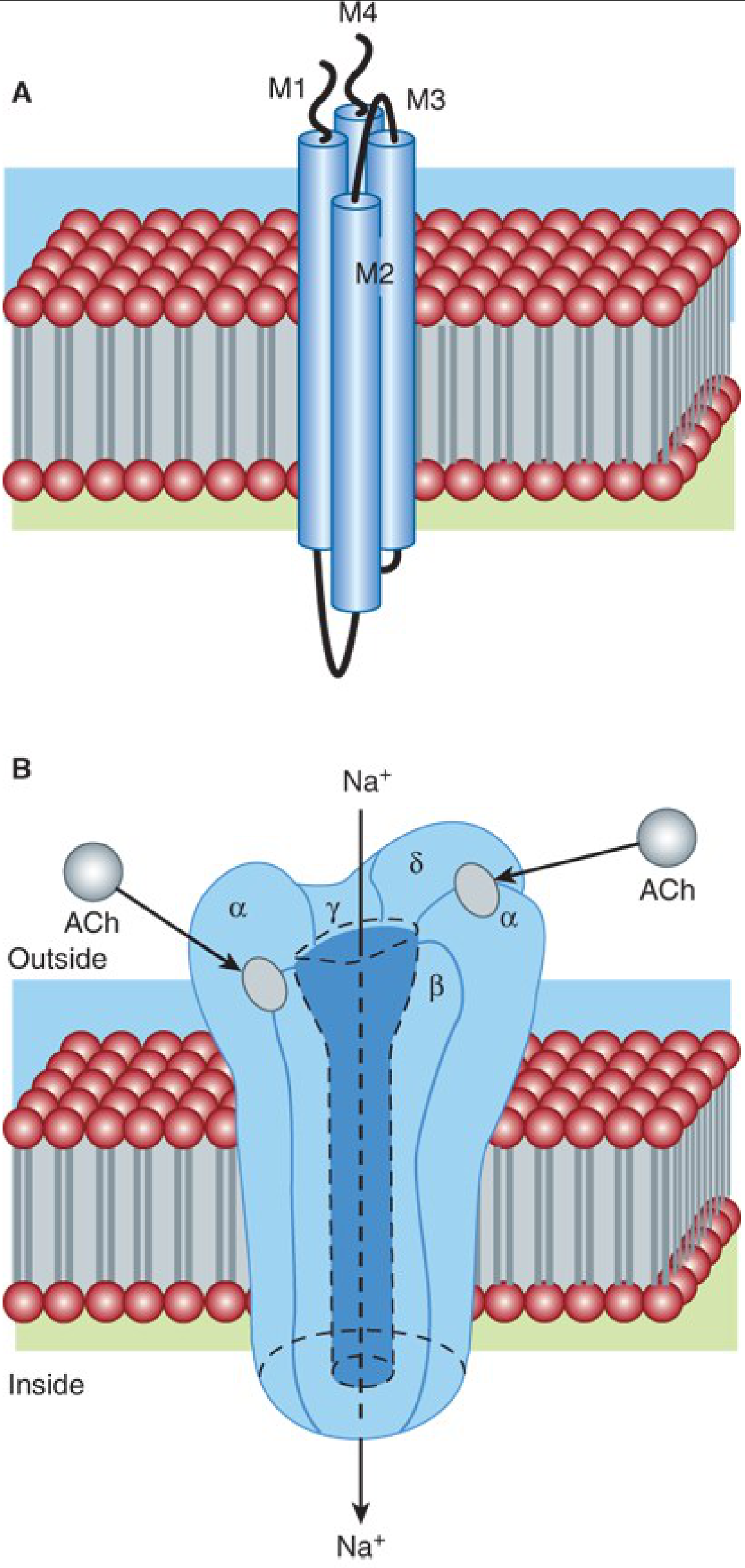
An action potential arriving at the motor nerve terminal triggers calcium influx and ACh release. ACh diffuses across the synaptic cleft and binds to nicotinic receptors (nAChR) on the motor end plate. The adult nAChR is a pentameric protein with two α subunits, one β, one δ, and one γ (fetal: α2βγδ). Two ACh molecules must bind (at the α-β and δ-α subunit interfaces) to open the ion channel, allowing Na⁺/K⁺ flux and generating an end plate potential. If large enough, this propagates an action potential along the entire muscle fiber. ACh is rapidly cleared by acetylcholinesterase.
- Postsynaptic (muscular) nAChR: α2βδε (adult) or α2βγδ (fetal/immature)
- Presynaptic (neuronal) nAChR: α2β2 pentameric complex
- Train-of-four (TOF) fade in nondepolarizing block results mainly from block of presynaptic nicotinic receptors
Classification
I. Depolarizing Agents
| Drug | Onset | Duration | Elimination |
|---|---|---|---|
| Succinylcholine | < 45 sec | 6-10 min (clinical); full recovery 15 min | Plasma pseudocholinesterase (butyrylcholinesterase) |
II. Nondepolarizing Agents
By Chemical Class:
A. Aminosteroids (Steroidal compounds)
| Drug | Duration | Notes |
|---|---|---|
| Rocuronium | Intermediate (30-60 min); at 1.2 mg/kg: 1-2 hours | Fastest onset of nondepolarizers; reversible with sugammadex |
| Vecuronium | Intermediate | No cardiovascular effects; metabolized by liver |
| Pancuronium | Long (>35 min) | Vagolytic tachycardia; primarily renal excretion |
| Pipecuronium | Long | Minimal cardiovascular effects |
B. Benzylisoquinolines
| Drug | Duration | Notes |
|---|---|---|
| Atracurium | Intermediate | Hoffman elimination + ester hydrolysis; slight histamine release |
| Cisatracurium | Intermediate | Stereoisomer of atracurium; no histamine release; no cardiovascular effects |
| Mivacurium | Short | Rapid hydrolysis by pseudocholinesterase |
| Tubocurarine (d-TC) | Long | Historical; ganglionic blockade + histamine release |
Note: Only aminosteroid compounds are typically used in the emergency department. Benzylisoquinolines are more common in the OR. - Rosen's Emergency Medicine, 10e
Mechanisms of Action
Depolarizing Block (Succinylcholine - Phase I Block)
Succinylcholine is structurally two ACh molecules linked together. It binds to nAChRs and causes sustained depolarization of the end plate, preventing repolarization. This produces:
- Initial muscle fasciculations (visible twitching)
- Followed by flaccid paralysis (sodium channels become inactivated)
- Resistance to further ACh stimulation
Phase II Block: With large or repeated doses, the character changes to resemble nondepolarizing block (fade on TOF, posttetanic potentiation).
Nondepolarizing Block
These agents competitively antagonize ACh at the postsynaptic α subunits of the nAChR, preventing ACh binding without causing depolarization. There are:
- No fasciculations
- TOF fade (ratio < 1.0)
- Posttetanic potentiation present
- Block can be reversed by acetylcholinesterase inhibitors
Key principle: Speed of onset is inversely proportional to potency among nondepolarizing agents. Rocuronium has ~13% the molar potency of vecuronium and 9% that of cisatracurium - this is why it has faster onset. - Miller's Anesthesia, 10e
Comparison: Depolarizing vs. Nondepolarizing Block
| Feature | Nondepolarizing | Succinylcholine Phase I | Succinylcholine Phase II |
|---|---|---|---|
| Train-of-four | Fade (TOF-R ~0.4) | No fade (TOF-R = 1.0) | Fade (TOF-R ~0.4) |
| Double burst | Fade | No fade | Fade |
| Posttetanic potentiation | Present | Absent | Present |
| Fasciculations | No | Yes | No |
| Effect of tubocurarine | Additive | Antagonistic | Augmented |
| Effect of neostigmine | Reversed | Augmented | Reversed |
Pharmacokinetics
- All NMBAs are highly polar, inactive orally; must be given parenterally
- Volume of distribution: 80-140 mL/kg (slightly larger than blood volume)
- Long-acting agents (e.g., pancuronium): primarily renal excretion; longer t½ (>35 min)
- Intermediate-acting agents (rocuronium, vecuronium, atracurium): multiple pathways (hepatic metabolism, Hofmann elimination, ester hydrolysis)
- Short-acting (mivacurium): almost exclusively pseudocholinesterase hydrolysis
- Steroidal NMBDs are metabolized in the liver to 3-hydroxy, 17-hydroxy, or 3,17-dihydroxy metabolites. The 3-hydroxy metabolites retain ~40-80% of parent drug activity (clinically relevant in ICU with prolonged infusions)
- Neuromuscular block develops faster and recovers faster in centrally located units (larynx, diaphragm, masseter) than in peripheral muscles (adductor pollicis)
Succinylcholine - Detailed Profile
Dosing: 1.5 mg/kg IV (based on total body weight even in obesity, as pseudocholinesterase activity increases with body habitus). The ED95 is 0.3 mg/kg but this dose is too slow for emergency use.
Hydrolysis: Plasma pseudocholinesterase hydrolyzes succinylcholine → succinylmonocholine (weak NMBA) → succinic acid + choline (inactive). Pseudocholinesterase is not present at the motor end plate; the drug is cleared systemically before most of it reaches the end plate.
Pseudocholinesterase deficiency: Can prolong block, but typically only to ~23 minutes at the extreme - rarely clinically significant in emergency settings.
Adverse Effects of Succinylcholine
1. Hyperkalemia (most dangerous)
- Expected K⁺ rise: 0.5-1.0 mEq/L (normal response)
- Dangerous rise (>5 mEq/L) in patients with:
- Burns
- Muscle pathology from trauma, denervation (spinal cord injury), immobilization
- Closed head injury
- Neuromuscular disease
- Proliferation of extrajunctional ACh receptors
- Safe in first 24 hours after acute burns/SCI - receptor upregulation takes time
- Patients at risk: those with pre-existing pathology OR weeks-to-months after injury
- Mechanism: fasciculation-related K⁺ release; extrajunctional receptor upregulation allows massive K⁺ efflux
2. Cardiovascular Effects
- As an ACh analogue, binds receptors throughout the body
- Stimulates both autonomic ganglia (positive chronotropy/inotropy) and cardiac muscarinic receptors (bradycardia)
- Bradycardia is especially common with a second dose given < 5 minutes after the first
- Prevention: atropine, thiopental, small dose of nondepolarizing NMBA, or ganglionic blockers
- With large doses: positive chronotropic/inotropic effects predominate
3. Increased Intraocular Pressure (IOP)
- Onset ~60 seconds, peaks 2-4 minutes, subsides by 5 minutes
- Mechanism: tonic myofibril contraction or choroidal vessel dilation
- Contraindicated in open globe injury (penetrating ocular trauma)
- Not contraindicated for routine ophthalmologic procedures with intact globe
4. Increased Intragastric Pressure
- Fasciculations can raise intragastric pressure 5-40 cmH₂O
- Increases aspiration risk - especially in diabetes, obesity, trauma, esophageal dysfunction
5. Muscle Pain (Myalgias)
- Post-op myalgias in 1-20% of cases; more common in ambulatory patients and heavily muscled individuals
- Caused by unsynchronized muscle fiber contractions during fasciculations
6. Increased ICP
- Succinylcholine may transiently raise ICP - controversial in head trauma
- If succinylcholine enables faster intubation, benefit may outweigh the transient ICP rise
7. Malignant Hyperthermia (rare)
- A rare but life-threatening interaction with volatile anesthetics
- Triggered by abnormal calcium release from skeletal muscle sarcoplasmic reticulum
- Absolute contraindication in susceptible individuals
Cardiovascular Effects of Nondepolarizing Agents
| Drug | Autonomic Ganglia | Cardiac Muscarinic | Histamine Release |
|---|---|---|---|
| Cisatracurium | None | None | None |
| Atracurium | None | None | Slight |
| Tubocurarine | Weak block | None | Moderate |
| Pancuronium | None | Moderate block (vagolytic → tachycardia) | None |
| Rocuronium | None | Slight | None |
| Vecuronium | None | None | None |
| Succinylcholine | Stimulation | Stimulation | Slight |
Clinically: Vecuronium, cisatracurium, and rocuronium have minimal cardiovascular effects - preferred in hemodynamically unstable patients. Pancuronium causes moderate tachycardia via vagolysis + norepinephrine release.
Drug Interactions
| Interaction | Effect |
|---|---|
| Volatile anesthetics (isoflurane > sevoflurane > desflurane > halothane > N₂O) | Potentiate nondepolarizing block (dose-dependent) |
| Aminoglycosides, tetracyclines | Enhance neuromuscular block |
| Calcium channel blockers | Enhance block |
| Magnesium | Enhances block (inhibits ACh release + reduces end plate sensitivity) |
| Cholinesterase inhibitors | Reverse nondepolarizing; augment succinylcholine Phase I |
| Repeated succinylcholine dosing | Phase II block develops |
Monitoring of Neuromuscular Block
Train-of-Four (TOF) stimulation (4 pulses at 2 Hz) is the standard monitor:
- TOF ratio (TOF-R) = 4th twitch / 1st twitch
- TOF-R ≥ 0.9 is required to exclude residual block (TOF-R ≥ 0.9 by quantitative/objective monitoring)
- Residual neuromuscular paralysis (TOF-R < 0.9 in PACU) reduces upper esophageal tone, coordination during swallowing, and hypoxic ventilatory drive - increases morbidity, mortality, and hospital length of stay
Other monitoring patterns:
- Double burst stimulation (DBS): two 3-stimulus 50Hz bursts; detects fade at lighter blocks
- Post-tetanic count (PTC): quantifies deep/profound block when TOF is absent
Reversal of Neuromuscular Block
1. Anticholinesterases (Classic Reversal)
- Neostigmine, edrophonium, pyridostigmine
- Inhibit acetylcholinesterase → ACh accumulates → competes out nondepolarizing agents
- Must co-administer anticholinergic (atropine or glycopyrrolate) to blunt muscarinic side effects (bradycardia, secretions, bronchospasm)
- Work best at shallow-to-moderate block (TOF count ≥ 2)
- Cannot reliably reverse deep block
- Do not reverse succinylcholine (augments Phase I block)
2. Sugammadex (Modern Reversal - Steroidal NMBDs Only)
Mechanism: Sugammadex is a modified γ-cyclodextrin - the first selective relaxant-binding agent. It forms a tight 1:1 "host-guest" encapsulation complex with steroidal NMBDs (primarily rocuronium > vecuronium; weak affinity for pancuronium):
- Stability of rocuronium-sugammadex complex: association:dissociation ratio = 25,000,000:1
- Affinity for vecuronium is 2.5x lower but still clinically adequate
- Rapid binding creates a plasma concentration gradient → draws rocuronium from the NMJ back into plasma → reversal of block
- No anticholinergic needed (no cholinergic mechanism involved)
- Not effective against benzylisoquinoline agents (cisatracurium, atracurium)
Pharmacokinetics: Volume of distribution 18L; elimination t½ ~100 min; up to 80% excreted unchanged in urine.
Dosing:
- Moderate block (TOF count ≥ 2): 2 mg/kg
- Deep block / post-tetanic count ≥ 1: 4 mg/kg
- Immediate reversal (e.g., "can't intubate, can't oxygenate" after high-dose rocuronium): 16 mg/kg
Important caveat: After sugammadex, subsequent steroidal NMBD block may be difficult to re-establish for hours due to residual encapsulated drug. Benzylisoquinolines (e.g., cisatracurium) can be used in this situation.
Rocuronium for RSI
Rocuronium (0.9-1.2 mg/kg) is the primary alternative to succinylcholine for rapid sequence intubation (RSI):
- At 1.2 mg/kg: intubating conditions in 1 minute; duration 1-2 hours
- No cardiovascular toxicity allows safe high-dose administration
- 2015 Cochrane review: succinylcholine superior at lower rocuronium doses, but at 1.2 mg/kg no difference in intubating conditions between the two agents
- Strongly preferred in succinylcholine contraindications (hyperkalemia risk, open globe, malignant hyperthermia susceptibility)
- Can be immediately reversed with sugammadex 16 mg/kg if airway is lost
Succinylcholine Contraindications (Summary)
| Contraindication | Reason |
|---|---|
| Open globe injury | IOP elevation → extrusion of ocular contents |
| Hyperkalemia or risk of massive K⁺ release | Burns (after 24h), SCI/denervation, prolonged immobility, crush injuries |
| Personal/family history of malignant hyperthermia | Trigger agent |
| Myopathies (especially Duchenne's, Becker's) | Rhabdomyolysis, hyperkalemia |
| Pseudocholinesterase deficiency | Prolonged paralysis |
Clinical Applications Summary
| Situation | Preferred Agent | Rationale |
|---|---|---|
| Standard RSI | Succinylcholine 1.5 mg/kg OR Rocuronium 1.2 mg/kg | Fastest onset, reliability |
| RSI with hyperkalemia risk | Rocuronium 1.2 mg/kg | Avoid succinylcholine |
| RSI with open globe | Rocuronium 1.2 mg/kg | Avoid IOP rise |
| "Cannot intubate, cannot oxygenate" post-RSI | Sugammadex 16 mg/kg (if rocuronium used) | Immediate reversal possible |
| Long surgical relaxation | Vecuronium, rocuronium, cisatracurium | Intermediate duration, no CV effects |
| Renal failure | Atracurium or cisatracurium | Hoffman elimination; organ-independent |
| ICU prolonged paralysis | Cisatracurium preferred | Organ-independent elimination; fewer active metabolites |
| Reversal after rocuronium/vecuronium | Sugammadex 2-4 mg/kg | Faster, more complete than neostigmine |
Recent Evidence (2025-2026)
- A 2025 systematic review and meta-analysis (PMID: 40186115) found that NMBA reversal agents have a measurable effect on perioperative neurocognitive function after general anaesthesia.
- A 2025 meta-analysis (PMID: 41039224) comparing rocuronium vs. succinylcholine in caesarean sections found comparable intubation conditions and neonatal outcomes.
- A 2026 systematic review (PMID: 41630605) in pediatrics found that avoiding NMBAs for tracheal intubation in children/infants had mixed outcomes - NMBAs generally still facilitate better intubating conditions.
Sources: Miller's Anesthesia 10e | Katzung's Basic & Clinical Pharmacology 16e | Rosen's Emergency Medicine 10e | Morgan & Mikhail's Clinical Anesthesiology 7e | Roberts & Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.