CHANGES DUE TO MECHANICAL VENTILATION, along with exam ready viva points
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive data from multiple authoritative textbooks. Let me compile the complete answer.
Changes Due to Mechanical Ventilation
A. Cardiovascular Changes
Mechanical ventilation (MV) fundamentally reverses normal respiratory physiology: spontaneous breathing creates negative intrathoracic pressure; MV creates positive intrathoracic pressure. This reversal drives all cardiovascular effects.
1. Decreased Venous Return (Preload Reduction)
- Positive pressure during inspiration raises intrathoracic pressure, compressing the great veins and right atrium
- Venous return from the systemic circulation falls
- Right ventricular (RV) filling decreases -> RV stroke volume falls
- Left ventricular (LV) preload consequently falls after 1-2 beats (pulmonary transit time)
- Net result: Cardiac output (CO) falls
2. Increased Pulmonary Vascular Resistance (PVR)
- Lung inflation compresses alveolar capillaries
- PVR rises, increasing RV afterload
- Can cause acute RV strain or failure, especially at high PEEP
3. Hypotension
- Reduced CO + decreased left ventricle-to-aorta pressure gradient -> systemic hypotension
- Particularly dangerous in hypovolemic patients or those with vasodilatory states (e.g., sepsis, spinal anesthesia)
- Can occur immediately after initiation of MV
4. LV Afterload Effects (Unique Benefit)
- Increased intrathoracic pressure paradoxically reduces LV afterload (transmural pressure falls)
- This can actually benefit patients with LV failure - MV can improve CO in cardiogenic pulmonary edema by unloading the failing LV
5. Pulse Pressure Variation (PPV) and Stroke Volume Variation (SVV)
- These cyclic respiratory-induced changes in arterial waveform are exaggerated in hypovolemia
- PPV >13% during controlled MV predicts fluid responsiveness
- Used as a dynamic measure to guide fluid resuscitation
Viva Point: "Why can initiating MV cause cardiovascular collapse?" Answer: PPV reduces venous return and CO; if the patient is already hypovolemic or vasodilated (e.g., sepsis), this reduction unmasks haemodynamic instability. Always pre-load the patient before intubation if possible.
B. Pulmonary Changes / Ventilator-Induced Lung Injury (VILI)
VILI is additional lung damage caused by mechanical ventilation itself. Four mechanisms are classically described:
1. Barotrauma
- Definition: Injury from excessive airway pressure (high peak inspiratory pressure [PIP] or plateau pressure)
- Manifestations: Pneumothorax, pneumomediastinum, subcutaneous emphysema, pneumopericardium
- Key threshold: Plateau pressure >30 cmH₂O significantly increases risk
- Volume-limited ventilation (vs. pressure-limited) is associated with decreased barotrauma incidence
2. Volutrauma
- Definition: Injury from excessive tidal volume causing alveolar overdistension
- More closely linked to VILI than barotrauma alone
- ARDSNet trial showed 6 mL/kg predicted body weight (PBW) tidal volumes reduced mortality vs. 12 mL/kg PBW
3. Atelectrauma
- Definition: Injury from repeated opening and closing (recruitment-derecruitment) of unstable alveoli with each breath cycle
- Creates shear stress at the interface of open and collapsed lung units
- PEEP is the primary strategy to prevent atelectrauma by keeping alveoli open at end-expiration
- The safe "window" lies between the lower inflection point (above which alveoli stay open) and the upper inflection point (above which overdistension begins) on the pressure-volume curve
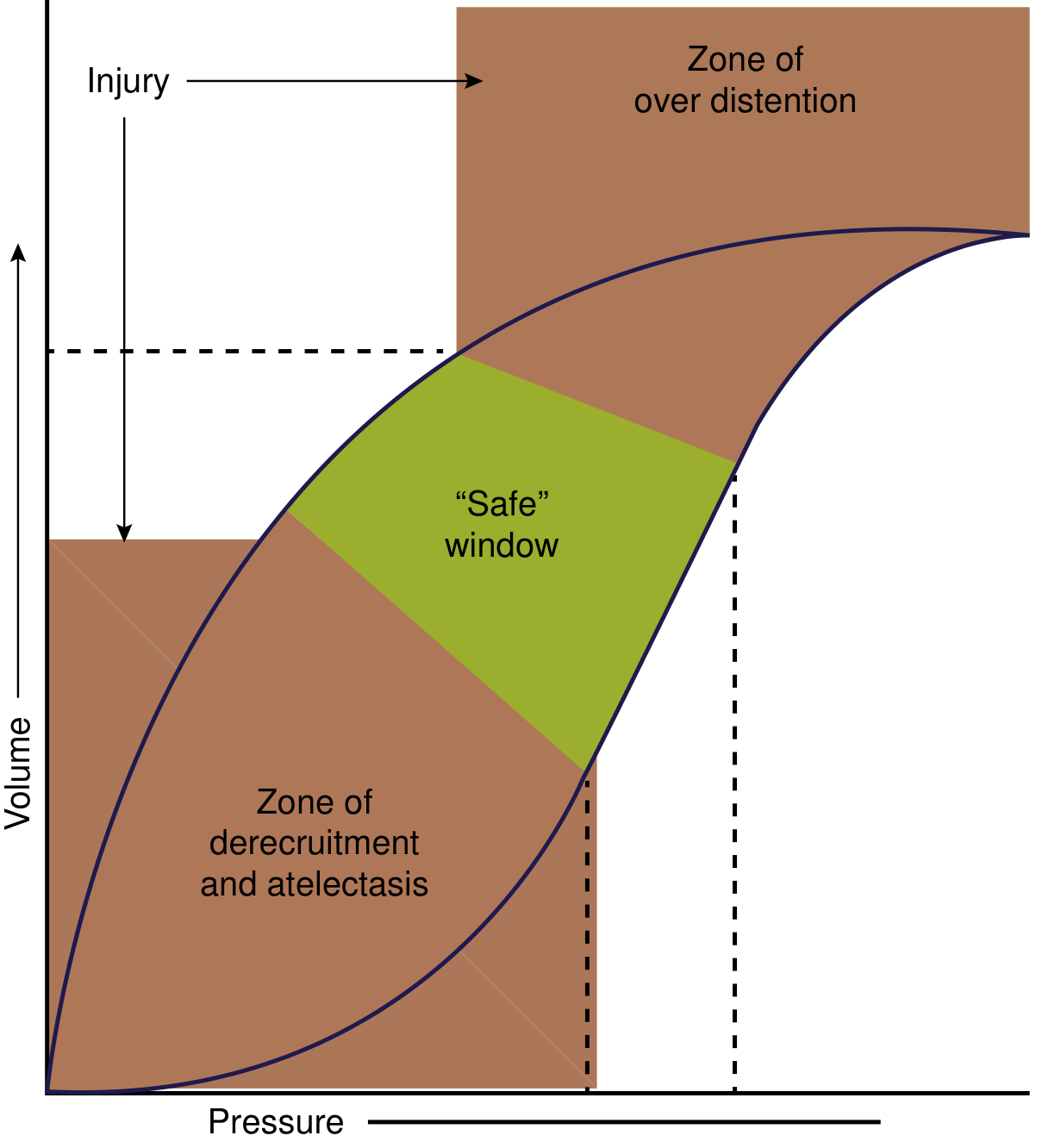
Pressure-volume curve: the green "safe window" lies between the zones of derecruitment/atelectasis (too low PEEP) and overdistension (too high pressure). - Current Surgical Therapy 14e
4. Biotrauma
- Cyclic stretching of lung parenchyma releases pro-inflammatory cytokines: IL-1, IL-6, IL-8, TNF-alpha, MIP-2
- Activates phospholipase A2 -> degrades surfactant
- Causes neutrophil accumulation in lung -> pulmonary edema, hyaline membrane formation, cellular infiltration
- Can lead to systemic inflammatory response (SIRS) and multiorgan failure
- Volatile anaesthetics (sevoflurane, isoflurane) attenuate VILI partly via anti-inflammatory effects
5. Oxygen Toxicity
- FiO2 >0.5-0.6 sustained over time -> reactive oxygen species (ROS) generation
- Causes alveolar injury indistinguishable from ARDS
- Also causes absorptive atelectasis: high FiO2 washes out nitrogen that normally acts as a "splint" for alveoli
Viva Point: "Name the 4 mechanisms of VILI." Answer: Barotrauma (pressure), Volutrauma (volume), Atelectrauma (shear from cycling), Biotrauma (cytokine release). Collectively these are avoided by lung-protective ventilation: tidal volume 6 mL/kg PBW, plateau pressure <30 cmH₂O, adequate PEEP.
C. Ventilator-Induced Diaphragm Dysfunction (VIDD)
Mechanism:
- Controlled MV suppresses diaphragm activity completely
- Within 12 hours of initiating controlled MV, diaphragm atrophy commences
- Reduced diaphragm activity -> reactive oxygen species (ROS) production -> mitochondrial dysfunction
- ROS activates proteolytic pathways: calcium-dependent enzymes, ubiquitin-proteasome pathway, autophagy
- Proteolysis exceeds protein synthesis -> progressive myofibrillar atrophy and disarray
- Diaphragm-specific atrophy (peripheral skeletal muscle is relatively spared in the early phase)
Clinical consequences:
- ~50% of patients develop at least 10% diaphragm atrophy within the first few days of MV
- These patients are at much higher risk of: prolonged MV, reintubation, tracheostomy, and ICU morbidity
- Creates a vicious cycle: acute respiratory failure -> MV -> VIDD -> diaphragm weakness -> prolonged ventilator dependence
Prevention:
- Maintaining some spontaneous respiratory effort (even partial) preserves diaphragm structure
- SIMV, pressure support modes preserve drive better than pure CMV/controlled modes
- Too much pressure support also causes atrophy - optimal level uncertain but must exceed a minimum activity threshold
Viva Point: "When does VIDD begin?" Answer: Within 12 hours of initiating controlled mechanical ventilation. This is why early spontaneous breathing trials and minimising over-sedation are emphasised in modern ICU care.
D. Renal Changes
Mediated primarily through hemodynamic and neurohumoral mechanisms:
| Mechanism | Effect |
|---|---|
| Increased intrathoracic/intrapleural pressure | Decreased venous return -> decreased cardiac output |
| Decreased CO + systemic BP | Carotid/aortic baroreceptor activation -> increased renal sympathetic tone -> renal vasoconstriction |
| Increased inferior vena caval pressure | Increased renal venous pressure -> increased peritubular capillary pressure -> increased tubular Na⁺ reabsorption |
| Decreased atrial filling | Reduced ANP secretion -> less natriuresis |
| RAAS activation | Renin -> angiotensin II -> aldosterone -> Na⁺ and water retention, oliguria |
| ADH (AVP) release | Volume receptors sense low atrial stretch -> increased ADH -> free water retention |
Net result: Decreased RBF, decreased GFR, oliguria, sodium retention, and increased risk of AKI - particularly with high PEEP levels.
Viva Point: "How does PEEP affect the kidneys?" Answer: PEEP reduces cardiac output and venous return, activates the RAAS and sympathetic nervous system, increases ADH, reduces ANP - resulting in oliguria, sodium retention, and reduced GFR. The extent depends on mean airway pressure.
E. Haemodynamic Monitoring Changes
- PEEP elevates measured central venous pressure (CVP) and pulmonary capillary wedge pressure (PCWP) artifactually - these readings must be corrected for intrathoracic pressure
- Pulse pressure variation (PPV) and stroke volume variation (SVV) are reliable dynamic preload indices only during controlled MV with regular tidal volumes
- During PPV, measurement of plateau pressure (a surrogate of transpulmonary pressure) is critical to guide lung-protective strategy
F. Other Systemic Changes
Intracranial Pressure (ICP)
- Positive pressure MV impedes cerebral venous drainage (raises jugular venous pressure)
- Can raise ICP, especially at high PEEP
- In head injury patients, brief hyperventilation (PaCO2 30-35 mmHg) remains a temporising measure to reduce ICP by cerebral vasoconstriction - but chronic hyperventilation is harmful
Gastrointestinal and Hepatic
- Reduced CO and splanchnic vasoconstriction impair gut perfusion
- Increased risk of stress ulcers -> stress ulcer prophylaxis is standard in ventilated ICU patients
- Hepatic venous congestion from raised right heart pressures
Ventilator-Associated Pneumonia (VAP)
- Defined as pneumonia developing >48 hours after intubation
- ETT bypasses upper airway defences; pooled secretions above cuff aspirate into lower airways
- Common organisms: Pseudomonas aeruginosa, Klebsiella, MRSA (late onset)
- Prevention bundle: head-of-bed elevation 30-45°, daily sedation holds, oral chlorhexidine, subglottic suctioning, early extubation
Summary Table - Exam Quick Reference
| System | Key Changes | Mechanism |
|---|---|---|
| CVS | ↓CO, ↓venous return, hypotension | ↑intrathoracic pressure compresses great veins |
| CVS (LV) | ↓afterload (beneficial in LVF) | ↑intrathoracic pressure reduces transmural LV pressure |
| Pulmonary (VILI) | Barotrauma, volutrauma, atelectrauma, biotrauma | Pressure/volume injury + cytokine release |
| Diaphragm (VIDD) | Atrophy within 12h; 50% lose >10% mass | Disuse -> ROS -> proteolysis (ubiquitin-proteasome) |
| Renal | ↓GFR, oliguria, Na⁺ retention, AKI | ↓CO -> RAAS + sympathetic activation + ↓ANP |
| ICP | ↑ICP (especially high PEEP) | Impaired cerebral venous drainage |
| Infectious | VAP | Aspiration of pooled secretions; ETT bypasses defences |
| GI | Stress ulcers | Splanchnic hypoperfusion |
High-Yield Viva Points (Master List)
-
Why does MV reduce cardiac output? PPV raises intrathoracic pressure -> compresses venae cavae -> reduces venous return -> reduces RV preload -> reduces CO (Frank-Starling). Also raises PVR, increasing RV afterload.
-
When is reduced CO from MV actually beneficial? In acute LV failure/cardiogenic pulmonary oedema - raised intrathoracic pressure unloads the LV (reduces afterload) and helps reverse the failure.
-
Define the 4 types of VILI: Barotrauma (pressure), Volutrauma (volume/overdistension), Atelectrauma (shear from cycling), Biotrauma (cytokine/inflammatory mediator release).
-
Target settings for lung-protective ventilation: Tidal volume 6 mL/kg PBW, plateau pressure ≤30 cmH₂O, titrated PEEP, permissive hypercapnia acceptable (pH >7.2).
-
When does VIDD begin? Within 12 hours. ~50% of patients lose >10% diaphragm mass in the first few days. Mechanism: disuse -> ROS -> ubiquitin-proteasome and autophagic proteolysis.
-
How does MV affect the kidneys? Via three routes: hemodynamic (↓CO -> ↓RBF), neurohumoral (RAAS, sympathetic, ADH), and direct venous congestion (↑renal venous pressure -> ↑Na reabsorption). Result: oliguria, Na retention, risk of AKI.
-
What is atelectrauma? Shear injury from repeated opening and closing of unstable alveoli with each breath - prevented by adequate PEEP above the lower inflection point of the P-V curve.
-
Define biotrauma: Release of cytokines (IL-1, IL-6, TNF-alpha) from mechanically stressed lung tissue causing systemic inflammation that can drive multi-organ failure.
-
What is VAP? How prevented? Pneumonia >48h post-intubation. Prevention: semi-recumbent positioning (30-45°), daily sedation breaks, subglottic suctioning, early weaning.
-
PPV effect on CVP/PCWP measurements: Both are artifactually elevated by positive intrathoracic pressure - must interpret with caution; end-expiratory values are most accurate.
Sources: Rosen's Emergency Medicine; Current Surgical Therapy 14e; Murray & Nadel's Textbook of Respiratory Medicine; Miller's Anesthesia 10e; Fishman's Pulmonary Diseases and Disorders
Increased intrathoracic pressure paradoxically reduces LV afterload (transmural pressure falls) How
Finding Sources
Finding Sources
Reading File
Reading File
All the textbook data I need is in hand. Here is a thorough but clear explanation:
How Does Increased Intrathoracic Pressure Reduce LV Afterload?
The Core Concept: Transmural Pressure
Afterload is not aortic pressure. Afterload is transmural pressure.
Transmural pressure = Intracavitary pressure - Surrounding (intrathoracic/pericardial) pressure
This is the pressure difference across the LV wall - the net outward force the myocardium must overcome to eject blood. This is what determines wall tension (by the Law of Laplace: T = P × r / 2h).
Step-by-Step Physiology
During Spontaneous Breathing (normal)
- Intrathoracic pressure is negative (e.g., -5 cmH₂O at rest, -20 to -30 during distress)
- LV sits inside this negative pressure environment
- To eject blood into the aorta (which is outside the thorax at atmospheric pressure), the LV must generate pressure from, say, -5 to +120 mmHg
- Transmural pressure the LV must overcome = Aortic pressure - Intrathoracic pressure = 120 - (-5) = 125 mmHg equivalent
- The more negative the intrathoracic pressure (e.g., laboured breathing in cardiogenic pulmonary oedema), the greater this gradient the LV must overcome
During Positive Pressure Ventilation
- Intrathoracic pressure becomes positive (e.g., +10 cmH₂O)
- The positive pressure transmits through the pleura into the pericardium, surrounding the LV
- The LV cavity pressure and the aortic pressure both see a rise in their surrounding reference pressure
- Transmural pressure = Aortic pressure - Intrathoracic pressure = 120 - (+10) = 110 mmHg
- The LV now has to generate less net wall tension to eject the same stroke volume
- This is the afterload reduction
Analogy to Understand It
Imagine squeezing a toothpaste tube (the LV) inside a pressurised chamber:
- Normally you squeeze against atmospheric pressure outside
- If the chamber is already pressurised, you need less effort to squeeze the same amount of paste out, because the external pressure is already "helping" push from outside
The LV is that toothpaste tube. Positive intrathoracic pressure "helps" push blood out by compressing the LV from the outside, reducing the net pressure gradient the myocardium itself must generate.
The Reverse is Also True (and Clinically Critical)
Large negative swings in intrathoracic pressure INCREASE LV afterload.
In cardiogenic pulmonary oedema (CPE) or severe obstructive breathing:
- The patient makes huge inspiratory effort against obstruction
- Intrathoracic pressure swings to -30 or -40 mmHg
- Transmural LV pressure rises dramatically: 120 - (-40) = 160 mmHg
- The failing LV must work much harder against this increased effective afterload
- This further impairs ejection, worsens pulmonary oedema, creating a vicious cycle
This is exactly why CPAP/BiPAP dramatically improves cardiogenic pulmonary oedema - it reverses this pathological afterload increase.
Summary Diagram (Conceptual)
SPONTANEOUS BREATHING (especially with distress):
Intrathoracic pressure = -20 mmHg
Aortic pressure = +120 mmHg
LV transmural pressure = 120 - (-20) = 140 mmHg ← HIGH afterload
POSITIVE PRESSURE VENTILATION:
Intrathoracic pressure = +10 mmHg
Aortic pressure = +120 mmHg
LV transmural pressure = 120 - (+10) = 110 mmHg ← LOWER afterload
Clinical Implications (Viva-Ready)
| Situation | Intrathoracic Pressure | LV Afterload | Clinical Effect |
|---|---|---|---|
| Normal spontaneous breathing | Slightly negative | Normal | - |
| Laboured breathing (CPE, severe asthma) | Very negative | Greatly increased | Worsens LV failure |
| CPAP / BiPAP / MV with PPV | Positive | Reduced | Improves LV ejection |
| Weaning from MV (removing PPV) | Returns to negative | Increases again | Can precipitate weaning-induced LV failure |
Viva Point: In patients with severe LV failure, removing positive pressure ventilation during weaning suddenly increases LV afterload. This is a recognised cause of weaning failure - the patient tolerates MV but decompensates when extubated. - Murray & Nadel's Textbook of Respiratory Medicine
Viva Point: The aorta exits the thorax. The LV sits inside the thorax. When intrathoracic pressure rises, the LV's surrounding pressure rises, but the aortic root's downstream (extrathoracic) pressure remains at atmospheric. The gradient the LV must overcome to eject blood decreases. This is the mechanism.
Sources: Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.