Hemothorax surgery theory mbbs final year university exam answer 20 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive 20-mark MBBS exam answer. Let me compose it.
HEMOTHORAX - Surgery Theory Answer (20 Marks)
Definition
Hemothorax is defined as the accumulation of blood within the pleural space. The diagnosis is confirmed when the hematocrit of pleural fluid is greater than 50% of the patient's peripheral blood hematocrit. It must be distinguished from a simple effusion because even a small volume of blood produces significant color change in pleural fluid, making laboratory confirmation essential.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 2368
Classification / Etiology
Hemothorax is broadly classified into three types:
1. Traumatic Hemothorax (Most Common)
Trauma accounts for nearly 300,000 cases annually. Sources of bleeding include:
- Blunt trauma: Motor vehicle accidents, falls - injuring intercostal vessels, lung parenchyma, diaphragm, great vessels, or mediastinal structures
- Penetrating trauma: Stab wounds, gunshot wounds (83% of penetrating chest injuries have associated pneumothorax)
- Rib fractures: A positive correlation exists between the number of rib fractures and hemothorax incidence. Patients with >5 rib fractures have a ≥48% likelihood of hemothorax
2. Nontraumatic (Spontaneous) Hemothorax
- Spontaneous pneumothorax - the most common nontraumatic cause; occurs in 2-7% of cases, from torn pleuropleural adhesions or rupture of vascularized bullae
- Vascular pathology: Aortic dissection (usually left-sided), rupture of pulmonary AVM (associated with hereditary hemorrhagic telangiectasia)
- Neoplasms: Schwannoma, pleural metastases, neurofibromatosis type 1
- Catamenial/Endometriosis: Thoracic endometrial implants, typically right-sided, in young women (14% of thoracic endometriosis syndrome)
- Coagulopathy, anticoagulant therapy
3. Iatrogenic Hemothorax
-
Thoracentesis
-
Central venous catheter placement (incidence 1.3-1.5%; reduced with ultrasound guidance)
-
Thoracic surgical procedures, pleural biopsy, pacemaker/AICD placement
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 2408-2429
Pathophysiology
Blood accumulates in the pleural space, compressing the lung and reducing pulmonary capacity. Three key mechanisms limit bleeding from torn lung parenchyma:
- The compressing effect of accumulated blood itself (tamponade)
- High concentration of lung thromboplastin
- Low pulmonary arterial pressure
Bleeding from systemic arteries (intercostal, internal mammary) or major pulmonary vessels does NOT self-tamponade and almost always requires invasive management.
The pleural space can accommodate up to 3 liters of blood. Massive hemothorax (>1500 mL) can produce tension physiology similar to tension pneumothorax, causing hemodynamic compromise from both:
-
Decreased cardiac preload (tension effect)
-
Hypovolemia from massive blood loss
-
Current Surgical Therapy 14e, p. 3728-3731; Tintinalli's Emergency Medicine, p. 4042
Classification by Volume
| Category | Volume | Significance |
|---|---|---|
| Small | <300 mL | May be observed |
| Moderate | 300-1500 mL | Tube thoracostomy indicated |
| Massive | >1500 mL | Operative exploration indicated |
Clinical Features
Symptoms
- Chest pain (pleuritic or constant)
- Dyspnea, tachypnea
- Hemoptysis (if lung parenchyma involved)
- Features of hypovolemic shock in massive hemothorax: hypotension, tachycardia, cold clammy extremities
Signs
- Asymmetric chest expansion
- Diminished/absent breath sounds on the affected side
- Stony dullness to percussion (vs. hyperresonance in pneumothorax)
- Mediastinal shift away from the effusion (in massive hemothorax)
- Tracheal deviation away from the side of lesion
- Features of tension physiology: hypotension, distended neck veins, tracheal deviation
The sensitivity of clinical examination increases with the size of the effusion.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 2373
Investigations
1. Chest X-Ray (CXR)
The initial and most widely used imaging modality:
- Upright/erect PA view: Blunting of the costophrenic angle requires approximately 200 mL of fluid
- The hemidiaphragm is obscured with 500-650 mL
- Supine film: May miss even large volumes (>1000 mL) - blood layers posteriorly, producing only diffuse haziness
- Lateral decubitus view: Most sensitive plain film; can detect as little as 10 mL
- Other findings: blunting of cardiophrenic angle, mediastinal shift, loss of diaphragm silhouette
CXR of massive hemothorax with tension component - note complete opacification of hemithorax and tracheal/mediastinal deviation:

Massive hemothorax: Complete opacification of left hemithorax with tracheal deviation to the right (Current Surgical Therapy 14e, Fig. 5)
2. CT Scan of Chest (Gold Standard)
- Most sensitive and specific for detecting and quantifying hemothorax
- Detects "hematocrit effect" - a fluid-fluid level (denser sedimented red cells below, serum above), pathognomonic of hemothorax
CT scan showing hematocrit effect in hemothorax (arrowheads indicate fluid-fluid level):
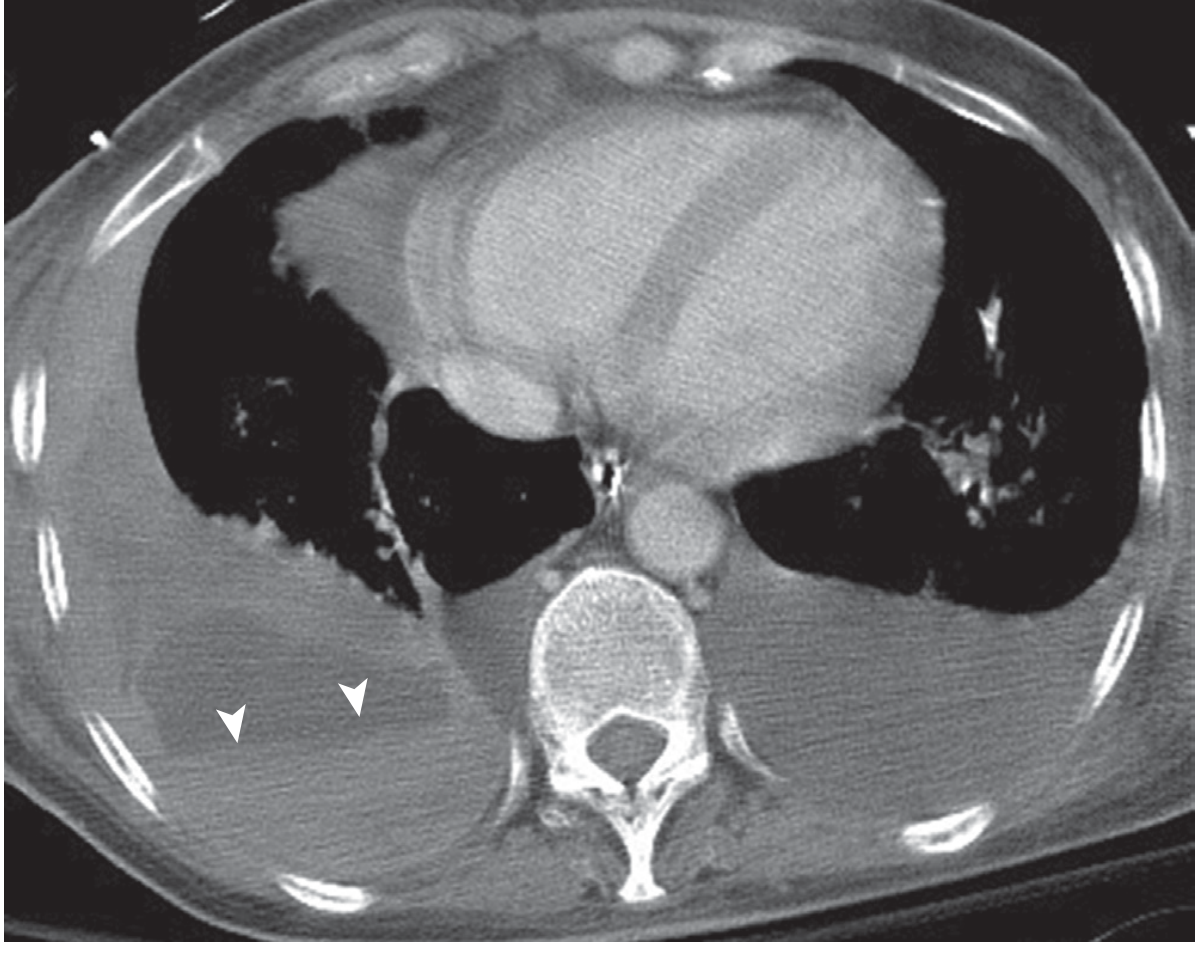
CT chest: "Hematocrit effect" - fluid-fluid level (arrowheads) pathognomonic of hemothorax (Murray & Nadel, Fig. 113.2)
- Best for diagnosing retained hemothorax and guiding intervention
3. Ultrasonography (POCUS/FAST)
- Rapidly performed at bedside - ideal in trauma and unstable patients
- Detects pleural fluid superior to the diaphragm; sensitivity comparable to CT for detecting significant hemothorax
- Can differentiate hemothorax from other pleural effusions based on echogenicity
4. Pleural Fluid Analysis
- Confirms diagnosis: pleural hematocrit >50% of peripheral hematocrit
- Helps exclude exudative effusion, empyema, chylothorax
5. Other Investigations
- FBC, coagulation profile, cross-match and group
- Serum LDH, protein
- ABG (assess respiratory failure)
Management
A. Resuscitation (Simultaneous with Diagnosis)
- Airway: Secure and maintain
- Breathing: High-flow oxygen
- Circulation: Two large-bore IV lines, fluid resuscitation, blood transfusion if hemodynamically unstable
- Analgesia
B. Tube Thoracostomy (Intercostal Chest Drain - ICD) - First Line Treatment
Indications (EAST guidelines recommend drainage of ALL hemothoraces irrespective of volume):
- Any hemothorax judged large enough to drain (>200-300 mL)
- Haemodynamically significant hemothorax
Technique:
- Large-bore chest tube (28-36 Fr / 32-36 Fr preferred in trauma)
- Site: 5th intercostal space, anterior axillary line (safe triangle)
- Pass tube over the superior border of the rib (to avoid the intercostal neurovascular bundle running along the inferior border)
- Connect to an underwater sealed drain
Outcome: In approximately 85% of cases, bleeding stops as the lung re-expands due to the low pressure in the pulmonary circulation.
Note: Shed blood should be collected in a sterile fashion to allow autotransfusion (cell salvage).
- Current Surgical Therapy 14e, p. 3729; Tintinalli's Emergency Medicine, p. 4044
C. Indications for Operative Exploration (Thoracotomy)
Emergency/urgent thoracotomy is indicated when:
- Massive hemothorax: Initial drainage of >1500 mL of blood
- Ongoing blood loss: >200 mL/hour for 4 consecutive hours
- Hemodynamic instability despite resuscitation and tube thoracostomy
- Massive continuous air leak suggesting major parenchymal injury or injury to a major airway
- Suspected injury to heart, great vessels, or thoracic esophagus
- Clotted/retained hemothorax not amenable to less invasive measures
D. Surgical Approaches
1. Video-Assisted Thoracoscopic Surgery (VATS)
- Preferred minimally invasive approach for:
- Retained hemothorax (especially within 3-5 days of chest tube placement - "early VATS")
- Clotted hemothorax not resolved by fibrinolytics
- Persistent bleeding from controllable sources
- Advantages: Less postoperative pain, shorter hospital stay, faster recovery, lower morbidity than open thoracotomy
- AAST data: VATS successful when hemothorax volume up to 900 mL; used in 33.5% of retained hemothorax cases
2. Open Thoracotomy
- Standard posterolateral thoracotomy (5th intercostal space) or anterolateral thoracotomy for emergencies
- Required for: massive uncontrolled hemorrhage, cardiac/great vessel injury, injuries requiring complex repair
- Necessary in 20.4% of retained hemothorax cases (AAST data)
- Allows: vessel ligation, lung repair/resection, decortication, pericardiotomy
3. Emergency Room Thoracotomy (ERT)
- For patients in extremis with penetrating chest trauma and loss of vital signs
- Allows: open cardiac massage, clamping of descending aorta, control of hilar bleeding
E. Intrapleural Fibrinolytics
- Streptokinase or tPA instilled via chest tube
- Used for retained/clotted hemothorax when VATS not immediately available
- Dissolves fibrin and clot to aid drainage
Complications
| Complication | Notes |
|---|---|
| Retained hemothorax | 10-15% of cases treated by tube thoracostomy |
| Empyema (post-traumatic) | 26.8% risk with retained hemothorax vs. 2% with complete evacuation |
| Fibrothorax | Organization of clot → fibrous peel → trapped lung; requires decortication |
| Lung entrapment | Encased lung unable to expand |
| Pneumonia/Atelectasis | From lung compression and immobility |
| Re-expansion pulmonary edema | After rapid drainage of large hemothorax |
| Shock | Hypovolemia from ongoing blood loss |
Independent risk factors for empyema: retained hemothorax, rib fractures, Injury Severity Score ≥25, need for additional procedures.
- Current Surgical Therapy 14e, p. 3747-3754; Murray & Nadel, p. 2480
Retained Hemothorax
Defined as persistence of blood in the pleural space despite chest tube drainage. Detected on CT chest.
Management (stepwise, least to most invasive):
- Observation - if volume <300 mL
- Image-guided drainage - CT or US-guided pleural aspiration/pigtail catheter
- Intrapleural fibrinolytics - streptokinase/tPA instilled via chest tube
- VATS (preferred; ideally 3-5 days post-chest tube) - removes clot, lyses adhesions, treats early fibrothorax
- Open thoracotomy with decortication - for organized fibrothorax, failed VATS
Summary Table
| Feature | Details |
|---|---|
| Definition | Blood in pleural space; pleural hematocrit >50% peripheral hematocrit |
| Most common cause | Blunt/penetrating chest trauma |
| Most common nontraumatic cause | Spontaneous pneumothorax |
| Minimum volume on erect CXR | 200 mL (costophrenic blunting) |
| Gold standard imaging | CT chest (shows hematocrit effect) |
| First line treatment | Tube thoracostomy (ICD) |
| Massive hemothorax definition | >1500 mL initial drainage |
| Indication for thoracotomy | >1500 mL initial OR >200 mL/hr x 4 hrs |
| ICD stops bleeding in | ~85% of cases |
| Most common complication | Retained hemothorax → empyema/fibrothorax |
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Current Surgical Therapy 14e | Tintinalli's Emergency Medicine | Fischer's Mastery of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.