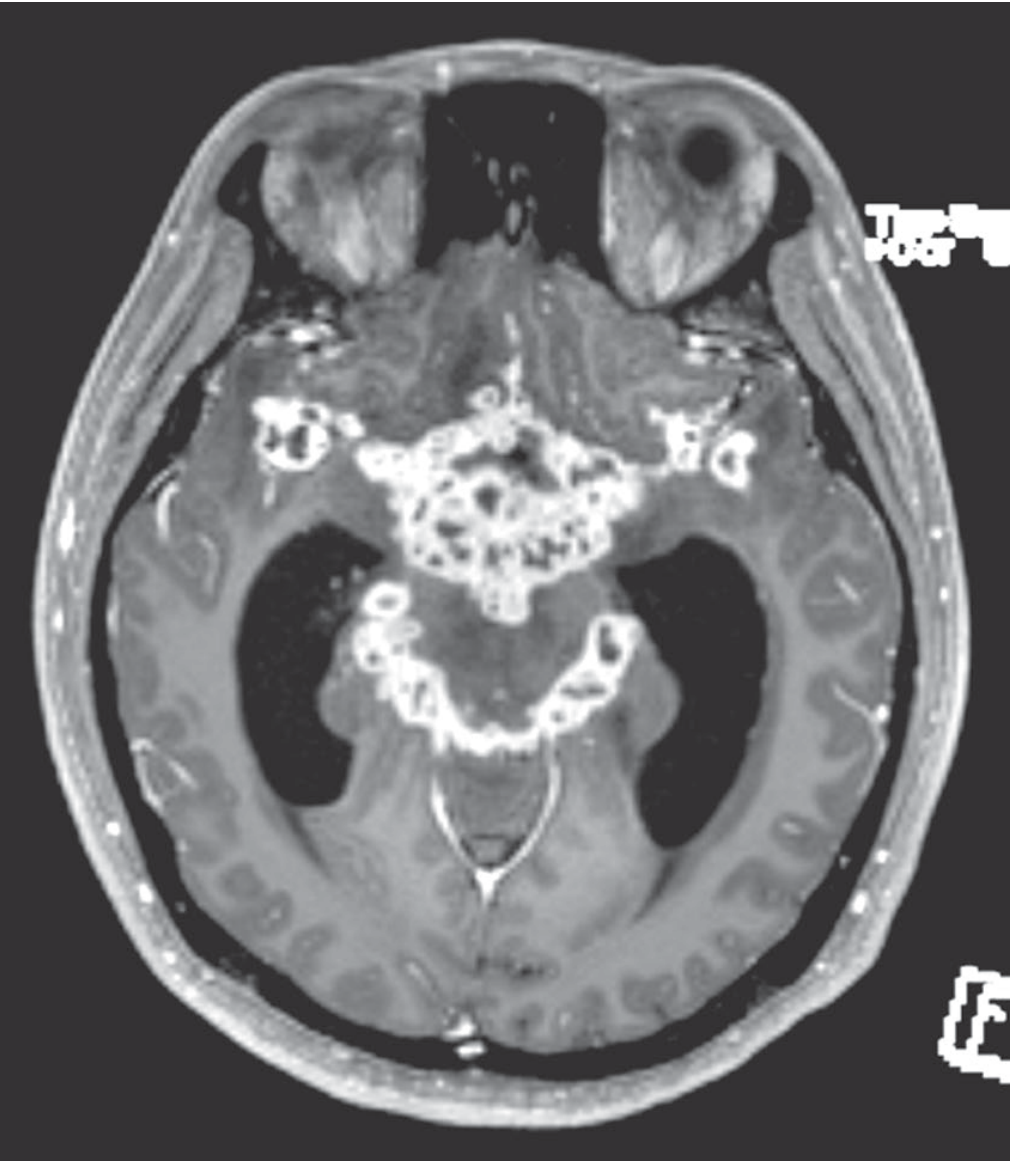
A 27-year-old man presents with gradually progressive headache, low-grade fever, vomiting and altered sensorium for the past 3 weeks. Neurological examination reveals neck stiffness and multiple cranial nerve palsies. Magnetic resonance imaging of the brain demonstrates dense basal meningeal exudates associated with hydrocephalus and multiple cerebral infarcts involving the basal ganglia region. What is the most likely diagnosis? A.Viral meningitis B.Tuberculous meningitis C.Herpes simplex encephalitis D.Cerebral malaria
Answer: B - Tuberculous Meningitis
Why This Presentation Is Classic for TBM
| Clinical Feature | Explanation in TBM |
|---|---|
| Gradual onset over 3 weeks | TBM is a subacute/chronic meningitis - progression over weeks is characteristic, unlike viral meningitis (days) or HSV encephalitis (acute) |
| Low-grade fever + headache + vomiting | The classic prodrome of TBM |
| Altered sensorium | Reflects raised ICP and parenchymal involvement |
| Neck stiffness | Meningeal irritation from the basal exudate |
| Multiple cranial nerve palsies | Directly caused by the thick gelatinous basal exudate compressing cranial nerves at the base of the brain |
| Dense basal meningeal exudates on MRI | The pathological hallmark of TBM - "the brunt of the process falls on the basal meninges, where a thick, gelatinous exudate accumulates, obliterating the pontine and interpeduncular cisterns" |
| Hydrocephalus | Classic complication; the basal exudate obstructs CSF drainage through the basal cisterns |
| Cerebral infarcts in basal ganglia | TBM causes endarteritis/vasculitis of perforating vessels supplying the basal ganglia - a well-recognized complication |
Pathological Basis (from Adams and Victor's Principles of Neurology, 12th Ed.)
- Encases cranial nerves III, IV, VI, VII at the base of the brain - causing the cranial nerve palsies
- Obstructs CSF flow - causing hydrocephalus
- Causes vasculitis of penetrating arteries - causing basal ganglia infarcts
Why the Other Options Are Wrong
- A. Viral meningitis - Acute onset (hours-days), NOT subacute over 3 weeks. Basal exudates, cranial nerve palsies, and basal ganglia infarcts are NOT typical. CSF is lymphocytic but without thick exudates.
- C. Herpes simplex encephalitis - Presents acutely with fever, seizures, and focal neurological deficits. Characteristically involves the temporal lobes and limbic system, NOT basal meninges. No cranial nerve palsies or basal exudates.
- D. Cerebral malaria - Caused by Plasmodium falciparum; presents with fever, seizures, and diffuse encephalopathy. Does NOT cause basal meningeal exudates, cranial nerve palsies, or subacute progression over weeks. Requires travel to endemic region.
A 27-year-old man presents with gradually progressive headache, low-grade fever, vomiting and altered sensorium for the past 3 weeks. Neurological examination reveals neck stiffness and multiple cranial nerve palsies. Magnetic resonance imaging of the brain demonstrates dense basal meningeal exudates associated with hydrocephalus and multiple cerebral infarcts involving the basal ganglia region. What is the most likely diagnosis? A.Viral meningitis B.Tuberculous meningitis C.Herpes simplex encephalitis D.Cerebral malaria
Answer: B - Tuberculous Meningitis
Why Every Clue Points to TBM
"The brunt of the pathologic process falls on the basal meninges, where a thick, gelatinous exudate accumulates, obliterating the pontine and interpeduncular cisterns and extending to the meninges around the medulla, the floor of the third ventricle and subthalamic region, the optic chiasm, and the undersurfaces of the temporal lobes."
Why the Other Options Are Wrong
| Option | Why It Doesn't Fit |
|---|---|
| A. Viral meningitis | Acute onset (hours to days), self-limiting; no basal exudates, no cranial nerve palsies, no infarcts |
| C. HSV encephalitis | Acute onset; preferentially involves the temporal lobes and limbic system (not basal meninges); presents with seizures and behavioral change, not cranial nerve palsies |
| D. Cerebral malaria | Diffuse encephalopathy from P. falciparum sequestration in microvasculature; no basal exudates; no cranial nerve palsies; requires travel to endemic area |