Edema
Reading File
Finding Sources
Searching PubMed
edema pathophysiology AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent! I now have comprehensive material. Let me compose the full answer.
Edema
Edema is the abnormal accumulation of fluid in the interstitial spaces of tissues (or body cavities). About 60% of lean body weight is water; only ~5% circulates as plasma, and 15% exists as interstitial fluid. When fluid shifts out of the vasculature and exceeds lymphatic drainage capacity, edema results.
Body Fluid Compartments (Normal)
| Compartment | % Body Weight |
|---|---|
| Intracellular fluid | ~40% |
| Extracellular fluid | ~20% |
| - Plasma | ~5% |
| - Interstitial fluid | ~15% |
Pathophysiology - The Starling Forces
Fluid movement across capillary walls is governed by opposing forces:
- Capillary hydrostatic pressure - pushes fluid out of vessels
- Plasma colloid osmotic pressure (mainly albumin) - pulls fluid into vessels
Normally, net outflow at the arteriolar end is nearly balanced by reabsorption at the venular end. The small residual filtrate is returned to circulation via lymphatics. Edema occurs when this balance is disturbed:
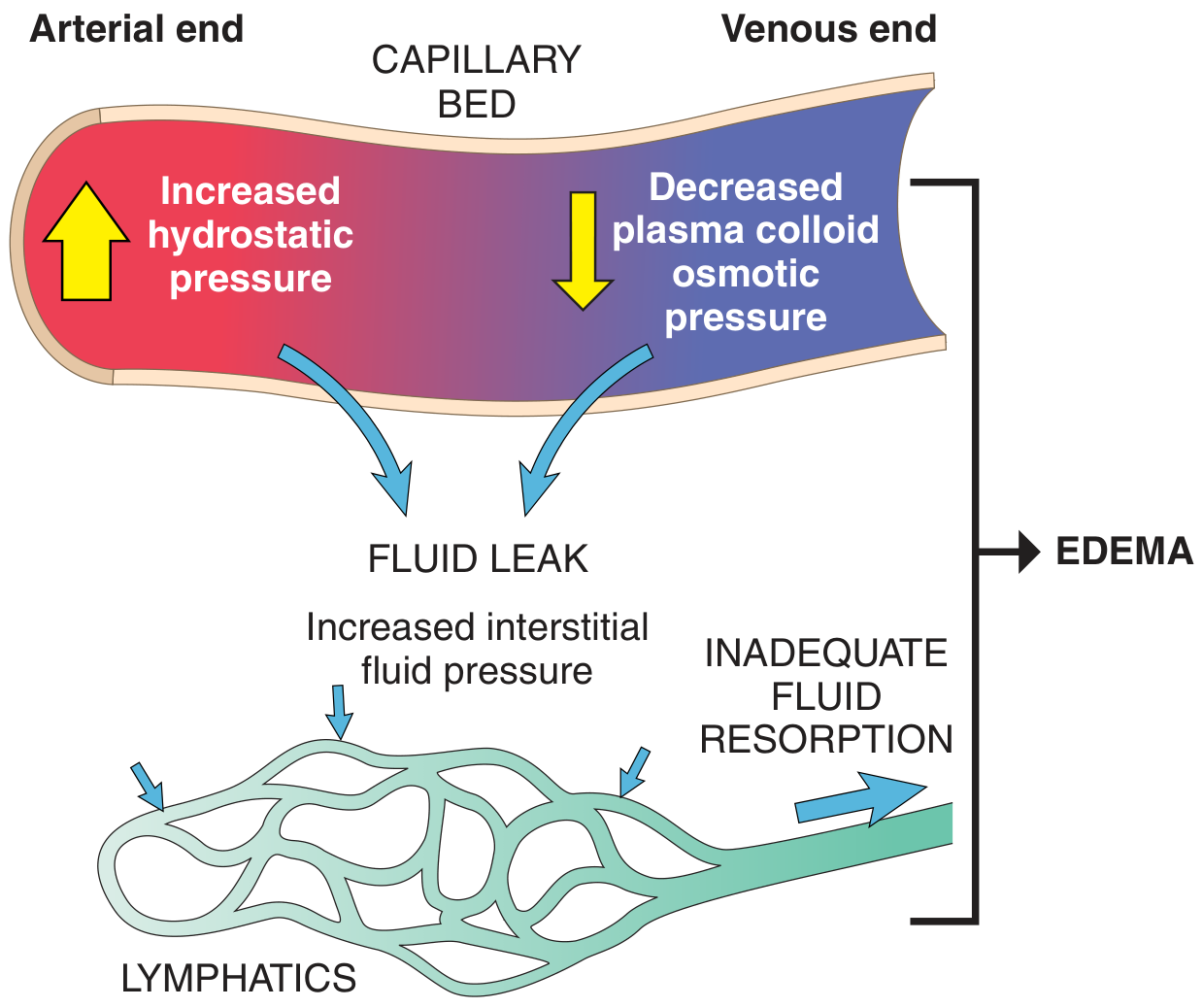
FIG. 3.2 - Robbins & Kumar Basic Pathology
Causes of Edema
1. Increased Hydrostatic Pressure
Impaired venous return raises capillary hydrostatic pressure, forcing fluid into the interstitium.
Examples:
- Congestive heart failure (CHF) - systemic venous hypertension; triggers secondary hyperaldosteronism via RAAS, worsening Na+/H2O retention
- Deep venous thrombosis - localized to affected limb
- Constrictive pericarditis, hepatic cirrhosis (portal hypertension)
- Venous obstruction by external compression or mass
- Prolonged dependency of limbs with inactivity
2. Reduced Plasma Osmotic Pressure (Hypoproteinemia)
Albumin provides ~50% of plasma colloid osmotic pressure. A fall in albumin below ~2.5 g/dL significantly impairs fluid resorption.
Causes of low albumin:
- Nephrotic syndrome - urinary albumin loss; most important cause of albuminuria
- Cirrhosis - reduced hepatic synthesis
- Protein malnutrition (e.g., kwashiorkor)
- Protein-losing enteropathy
Low albumin → reduced intravascular volume → renal hypoperfusion → secondary hyperaldosteronism → more Na+/H2O retention → worsens edema (a vicious cycle)
3. Lymphatic Obstruction (Lymphedema)
Blockage of lymphatic drainage prevents removal of normal interstitial filtrate, causing protein-rich edema (lymphedema).
Examples:
- Filariasis (Wuchereria bancrofti) - fibrosis of inguinal lymphatics causing "elephantiasis" of lower limb/genitalia
- Breast cancer - lymphatic invasion causes peau d'orange (orange peel) skin
- Post-mastectomy/radiation - axillary lymph node disruption causes arm lymphedema
4. Increased Vascular Permeability
Inflammatory mediators (histamine, bradykinin, cytokines) damage endothelium, allowing protein-rich fluid to leak out (exudate).
Examples: Acute inflammation, burns, sepsis, anaphylaxis
5. Sodium and Water Retention
Primary renal sodium retention expands intravascular volume and raises hydrostatic pressure.
Examples: Acute renal failure, post-streptococcal glomerulonephritis
Systemic Edema Pathways
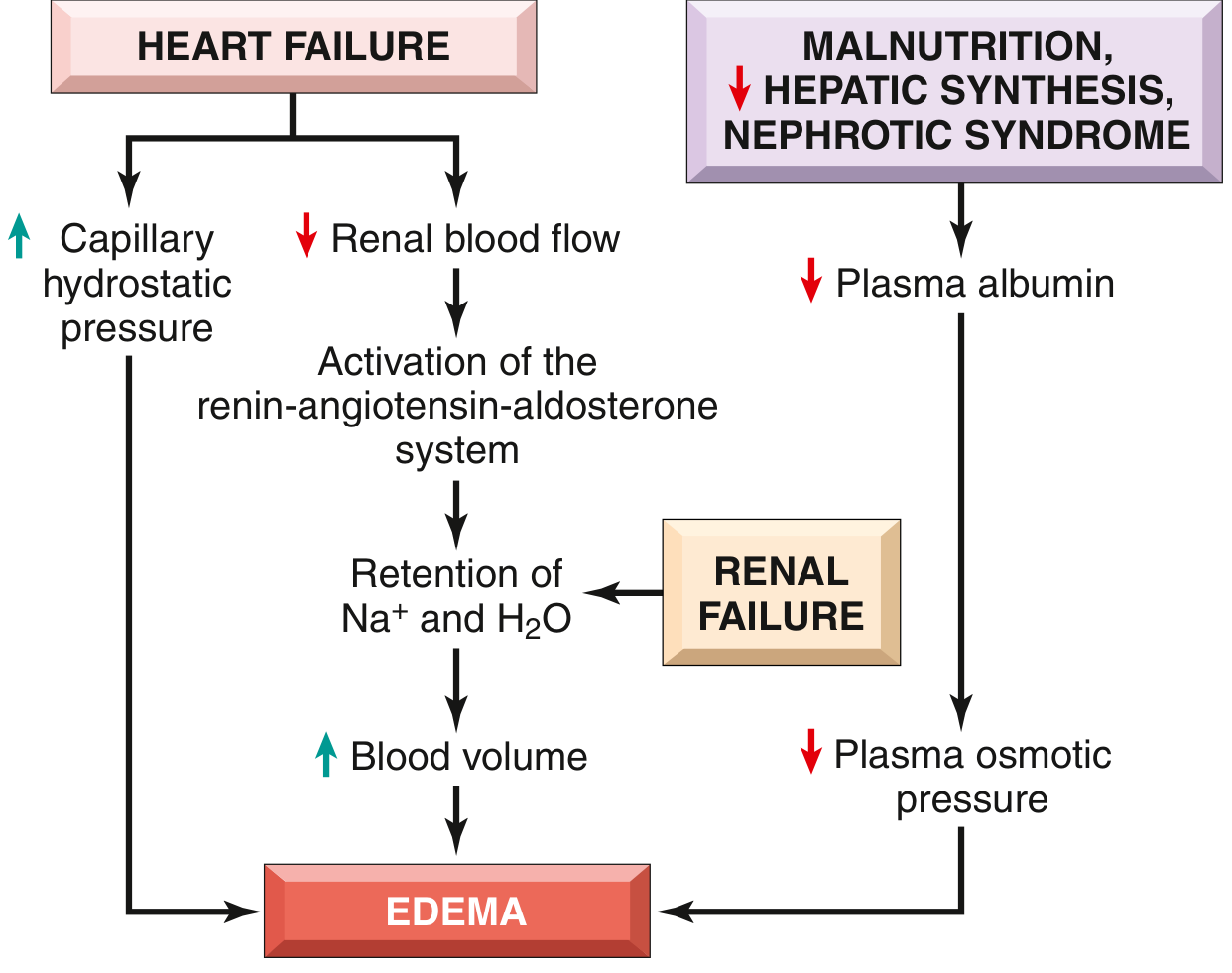
FIG. 3.3 - Robbins & Kumar Basic Pathology
Fluid Type: Transudate vs. Exudate
| Feature | Transudate | Exudate |
|---|---|---|
| Mechanism | ↑ hydrostatic pressure or ↓ osmotic pressure | ↑ vascular permeability |
| Protein content | Low (protein-poor) | High (protein-rich) |
| Causes | CHF, nephrotic syndrome, cirrhosis | Inflammation, infection, malignancy |
| Specific gravity | <1.012 | >1.020 |
Special Forms of Edema
| Term | Definition |
|---|---|
| Anasarca | Severe, generalized edema with profound subcutaneous swelling and fluid in body cavities |
| Hydrothorax | Fluid in the pleural cavity |
| Hydropericardium | Fluid in the pericardial cavity |
| Ascites / Hydroperitoneum | Fluid in the peritoneal cavity |
| Pulmonary edema | Fluid in lung interstitium/alveoli; causes dyspnea, orthopnea |
| Cerebral edema | Dangerous - increases intracranial pressure; vasogenic (BBB disruption) or cytotoxic (cell swelling) |
| Pitting edema | Subcutaneous edema that retains an indentation when pressed; typical in cardiac/renal edema |
| Non-pitting edema | Lymphedema or myxedema (hypothyroidism); does not pit because of high protein/mucopolysaccharide content |
Morphology
Edema is recognized grossly as tissue swelling. Microscopically, it appears as clearing and separation of extracellular matrix elements. The most clinically significant sites:
- Subcutaneous edema - pitting in dependent areas (ankles in ambulatory patients, sacrum in bedridden patients)
- Pulmonary edema - frothy pink fluid, heavy lungs; impairs gas exchange
- Cerebral edema - brain herniates through foramen magnum; life-threatening
Clinical Approach (Harrison's Framework)
-
Localized or generalized?
- Localized → identify local cause (DVT, inflammation, lymphatic obstruction)
- Generalized → proceed below
-
Hypoalbuminemia present? (albumin <3.0 g/dL)?
- Yes → evaluate for cirrhosis, malnutrition, nephrotic syndrome
-
Evidence of heart failure?
- Assess for elevated JVP, S3 gallop, pulmonary rales, leg edema
-
Urine output?
- Oliguria/anuria → renal failure
Treatment Principles
The primary goal is treating the underlying disorder. General measures:
- Dietary sodium restriction - limits fluid retention
- Diuretics (loop diuretics like furosemide; thiazides) - promote renal Na+/water excretion
- Aldosterone antagonists (spironolactone) - particularly useful in CHF and cirrhosis with secondary hyperaldosteronism
- Leg elevation - reduces gravitational hydrostatic pressure
- Compression stockings - for lymphedema and venous insufficiency
- Treat underlying cause - optimize cardiac function, correct hypoalbuminemia, treat infections causing lymphedema
Sources:
- Robbins & Kumar Basic Pathology, pp. 79-81 (Edema - causes, mechanisms, morphology)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 43 (Edema summary)
- Harrison's Principles of Internal Medicine 22E, p. 326 (Clinical approach)
- Ganong's Review of Medical Physiology, p. 16 (Fluid compartments and edema)
This is a shared conversation. Sign in to Orris to start your own chat.