Classify antihypertensive drugs. Explain the mechanism, therapeutic uses, and adverse effects of Angiotensin receptor blockers / ACE Inhibitors
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a complete, well-illustrated answer. Here is the full response:
Classification of Antihypertensive Drugs
Antihypertensive agents are grouped by their primary mechanism of action:
| Class | Examples |
|---|---|
| Diuretics | Thiazides (hydrochlorothiazide, chlorthalidone), Loop (furosemide, torsemide), K+-sparing (spironolactone, triamterene) |
| ACE Inhibitors | Captopril, Enalapril, Lisinopril, Ramipril, Fosinopril, Quinapril, Perindopril |
| Angiotensin Receptor Blockers (ARBs) | Losartan, Valsartan, Candesartan, Irbesartan, Telmisartan, Olmesartan |
| Calcium Channel Blockers (CCBs) | Amlodipine, Nifedipine, Diltiazem, Verapamil, Nicardipine |
| Beta-blockers | Metoprolol, Atenolol, Bisoprolol, Carvedilol, Labetalol, Nebivolol, Propranolol |
| Alpha-1 blockers | Prazosin, Doxazosin, Terazosin |
| Centrally acting agents | Clonidine (alpha-2 agonist), Methyldopa |
| Direct vasodilators | Hydralazine, Minoxidil |
| Renin inhibitors | Aliskiren |
| ARNI | Sacubitril/Valsartan (Entresto) |
The Renin-Angiotensin-Aldosterone System (RAAS) - Drug Targets
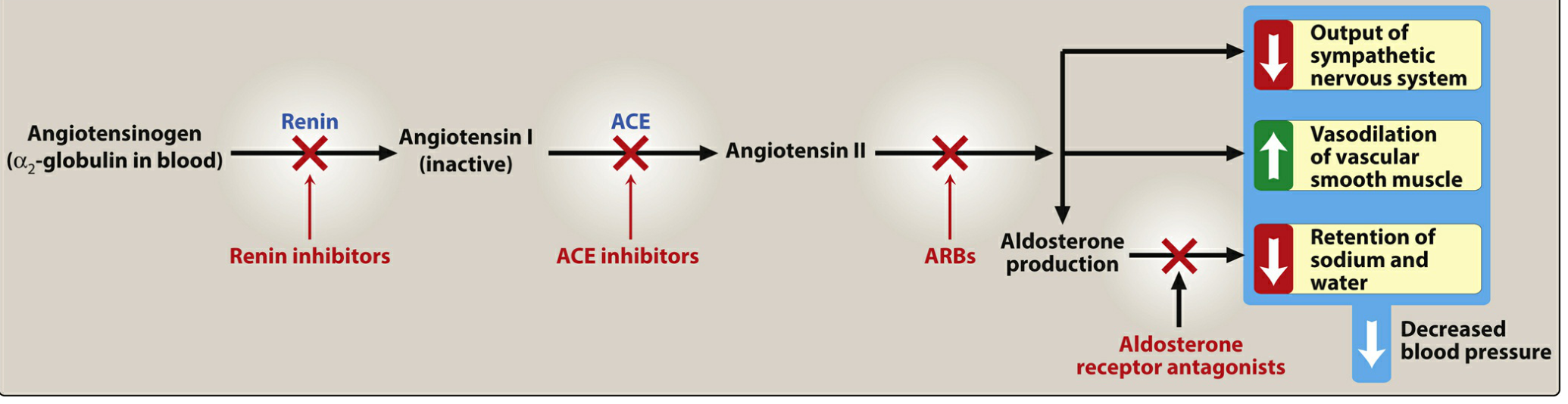
Fig. 8.10 - Effects of drug classes on the RAAS. Lippincott Illustrated Reviews: Pharmacology
ACE Inhibitors
Drugs
Captopril, Enalapril, Lisinopril, Ramipril, Fosinopril, Quinapril, Perindopril, Benazepril, Trandolapril, Moexipril
Mnemonic: "Can Every Large River Flow Quickly Past Big Talls?" (Captopril, Enalapril, Lisinopril, Ramipril, Fosinopril, Quinapril, Perindopril, Benazepril, Trandolapril)
Mechanism of Action
ACE (angiotensin-converting enzyme) is responsible for two key reactions:
- Converts Angiotensin I → Angiotensin II (the potent vasoconstrictor)
- Degrades bradykinin (a vasodilatory peptide)
ACE inhibitors block this enzyme, producing the following effects:
- ↓ Angiotensin II → reduced vasoconstriction → decreased afterload
- ↓ Aldosterone secretion → decreased Na+ and water retention → decreased preload
- ↑ Bradykinin → bradykinin stimulates nitric oxide and prostacyclin production → potent vasodilation of arterioles and veins
- Efferent arteriolar vasodilation → reduced intraglomerular pressure → renoprotection
- Block maladaptive cardiac remodeling (myocyte hypertrophy, fibrosis, sympathetic activation) mediated by AT1 receptors
In heart failure, excessive Ang II via AT1 receptors causes vasoconstriction (raises afterload), myocyte growth, sympathetic activation, prothrombotic effects, increased arginine vasopressin, and aldosterone-driven sodium retention - all of which are blocked by ACE inhibitors. - Goldman-Cecil Medicine, block5
Therapeutic Uses
| Indication | Notes |
|---|---|
| Hypertension | First-line; preferred with compelling indications |
| Heart failure (HFrEF) | Reduce mortality, improve EF, decrease hospitalizations |
| Post-MI | Reduce ventricular remodeling, improve survival |
| Diabetic nephropathy | Slow CKD progression independently of BP; reduce albuminuria |
| Chronic kidney disease | Reduce proteinuria (effect independent of BP lowering) |
| Asymptomatic LV systolic dysfunction | Benefit even in NYHA class I |
| Prevention of MI | Reduce risk of new coronary events |
| Left ventricular hypertrophy | Regression with chronic treatment |
ACE inhibitors slow the progression of diabetic nephropathy and decrease albuminuria. Chronic treatment achieves regression of left ventricular hypertrophy and improved ventricular remodeling after MI. - Lippincott Illustrated Reviews: Pharmacology
Pharmacokinetics
- All are orally bioavailable as drugs or prodrugs (most are prodrugs converted hepatically to active form, e.g., enalapril → enalaprilat)
- Captopril and lisinopril are not prodrugs - preferred in severe hepatic impairment
- Fosinopril is the only ACE inhibitor NOT eliminated primarily by kidneys - no renal dose adjustment needed
- Enalaprilat is the only IV formulation
Adverse Effects
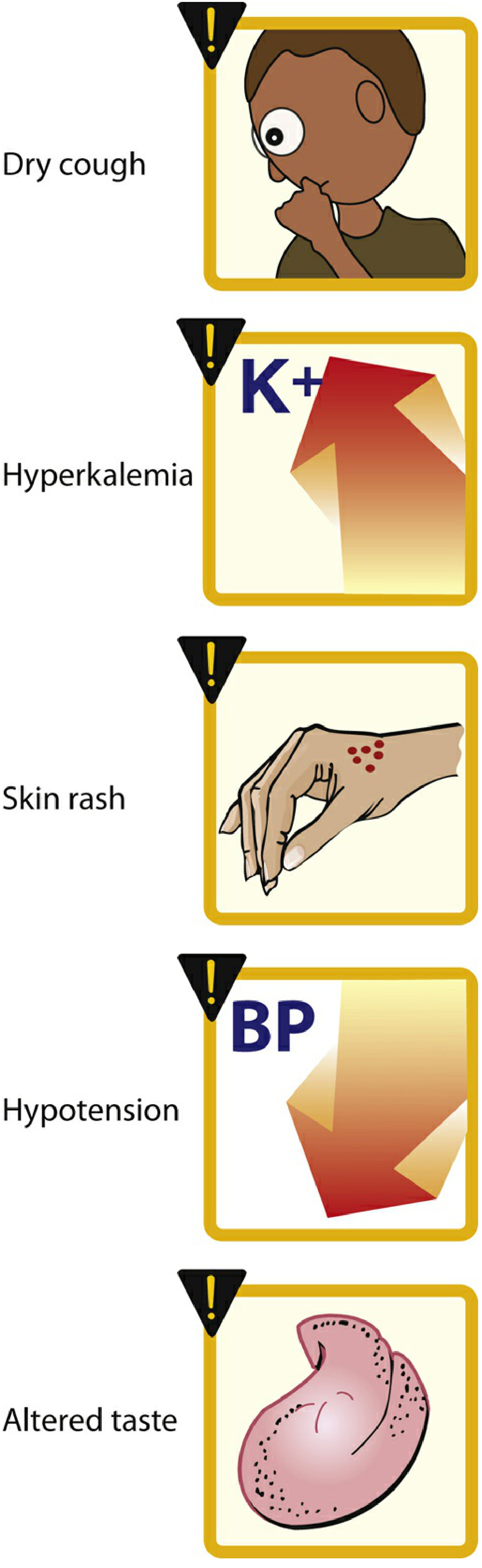
Fig. 8.11 - Common adverse effects of ACE inhibitors. Lippincott Illustrated Reviews: Pharmacology
| Adverse Effect | Mechanism | Notes |
|---|---|---|
| Dry cough | ↑ Bradykinin + substance P in pulmonary tree | Up to 10% of patients; more common in women; resolves on stopping drug |
| Angioedema | ↑ Bradykinin → swelling of lips, oral mucosa, throat | Rare but potentially life-threatening; absolute contraindication to re-use |
| Hyperkalemia | ↓ Aldosterone → ↓ K+ excretion | Monitor K+; use K+-sparing diuretics with caution |
| First-dose hypotension | Sudden loss of Ang II-mediated vascular tone | Especially in volume-depleted patients |
| Acute kidney injury / azotemia | ↓ Efferent arteriolar tone → ↓ GFR | Risk if bilateral renal artery stenosis; creatinine rise up to 30% above baseline is acceptable |
| Skin rash | Especially with captopril (sulfhydryl group) | |
| Dysgeusia (altered taste) | Especially captopril | |
| Teratogenicity | Fetal renal tubular dysplasia, oligohydramnios, limb contractures | Absolutely contraindicated in pregnancy (all trimesters) |
Contraindications
- History of angioedema (with any ACE inhibitor)
- Bilateral renal artery stenosis - risk of precipitous GFR loss
- Pregnancy
- Hyperkalemia (K+ > 5.0 mmol/L)
- Significant hypotension (SBP < 90 mmHg)
- Do not combine with ARB - increased side effects without benefit
- Do not combine with sacubitril/valsartan (ARNI) - high risk of angioedema
Angiotensin Receptor Blockers (ARBs)
Drugs
Losartan, Valsartan, Candesartan, Irbesartan, Telmisartan, Olmesartan, Azilsartan
All end in "-sartan"
Mechanism of Action
ARBs selectively block the AT1 receptor (angiotensin II type 1 receptor), preventing angiotensin II from binding regardless of its source of production (ACE-dependent or non-ACE pathways like chymase).
Key consequences:
- Block all AT1-mediated effects of Ang II: vasoconstriction, aldosterone secretion, sympathetic activation, myocyte hypertrophy, sodium/water retention
- Unlike ACE inhibitors, ARBs do NOT inhibit bradykinin breakdown (they do not block kinase II / ACE)
- Because AT1 receptors are blocked, Ang II accumulates and preferentially activates the AT2 receptor, which has beneficial cardiovascular effects (vasodilation, anti-proliferative, increased bradykinin) - though this effect is more modest than the bradykinin increase seen with ACE inhibitors
- More complete blockade of Ang II effects than ACE inhibitors (because non-ACE sources of Ang II production are also covered)
ARBs selectively block the action of angiotensin II at the AT1 receptor. Although pharmacologically distinct from ACE inhibitors, their clinical effects are similar. Because ACE inhibitors also reduce the breakdown of bradykinin, ACE inhibitors - not ARBs - cause cough and angioedema (which is bradykinin-related). - Goldman-Cecil Medicine
Therapeutic Uses
| Indication | Notes |
|---|---|
| Hypertension | First-line, especially in ACE inhibitor-intolerant patients |
| Heart failure (HFrEF) | Used when patients cannot tolerate ACE inhibitors (cough/angioedema) |
| Post-MI with LV dysfunction | Valsartan equivalent to captopril in reducing mortality |
| Diabetic nephropathy | Renoprotective (reduced albuminuria, slowed progression) |
| Chronic kidney disease | First-line with or without diabetes |
| LV hypertrophy | Regression of hypertrophy |
| Prevention of stroke | Losartan shown to reduce stroke risk |
| Atrial fibrillation prevention | Especially in patients with hypertension + LVH |
Candesartan reduces risk of cardiovascular death or HF hospitalization. Valsartan is as effective as captopril in reducing mortality following acute MI with LV dysfunction. - Goldman-Cecil Medicine, block5
Adverse Effects
ARBs have a more favorable side-effect profile than ACE inhibitors:
| Adverse Effect | Compared to ACE inhibitors |
|---|---|
| Hypotension | Similar |
| Hyperkalemia | Similar (same mechanism - ↓ aldosterone) |
| Renal dysfunction / azotemia | Similar |
| Dry cough | Rare / absent (no bradykinin accumulation) |
| Angioedema | Much less common, but can still occur (via AT2 → bradykinin) |
| Teratogenicity | Same - absolutely contraindicated in pregnancy |
| Dizziness | Occasional |
Both ACEIs and ARBs have similar effects on blood pressure, renal function, and potassium. Problems of symptomatic hypotension, azotemia, and hyperkalemia are similar for both agents. Although less frequent than with ACEIs, angioedema has also been reported in some patients who receive ARBs. - Braunwald's Heart Disease
Contraindications
- Pregnancy (teratogenic)
- Bilateral renal artery stenosis
- Significant hyperkalemia
- Do not combine with ACE inhibitor - increased adverse effects without added efficacy
- Do not combine with ARNI (sacubitril/valsartan) + ACE inhibitor simultaneously
Key Comparison: ACE Inhibitors vs ARBs
| Feature | ACE Inhibitors | ARBs |
|---|---|---|
| Site of action | Blocks ACE enzyme | Blocks AT1 receptor |
| Bradykinin | ↑ (inhibits breakdown) | Not affected |
| Dry cough | ~10% | Rare (< 1%) |
| Angioedema | Rare (~0.1-0.3%) | Very rare |
| Ang II levels | ↓ | ↑ (receptor blocked) |
| AT2 receptor activation | Modest | Enhanced (more Ang II available) |
| Non-ACE Ang II sources | NOT blocked | Blocked (receptor-level) |
| First-line preference | Yes (primary) | When ACE inhibitor not tolerated |
| Pregnancy | Contraindicated | Contraindicated |
| Combined use (ACE + ARB) | Contraindicated (increased harm) | Contraindicated |
Special Populations and Considerations
- CKD with proteinuria: Both ACE inhibitors and ARBs are first-line; reduce proteinuria independent of BP. A rise in creatinine up to 30% above baseline is acceptable.
- Bilateral renal artery stenosis: Both are contraindicated - loss of efferent arteriolar tone precipitates acute kidney injury.
- Heart failure: ACE inhibitors remain first-line (Class I); ARBs are Class I alternatives for ACE-intolerant patients. ARNI (sacubitril/valsartan) is preferred early if tolerated.
- Black patients: Monotherapy with ACE inhibitors or ARBs is less effective (lower renin activity); calcium channel blockers or thiazides are preferred unless a compelling indication (e.g., HF, CKD) exists.
- High dietary sodium: Can abrogate the antiproteinuric effect of ACE inhibitors; adding a thiazide diuretic restores the effect.
Sources: Lippincott Illustrated Reviews: Pharmacology, p. 302-305 | Goldman-Cecil Medicine | Goodman & Gilman's Pharmacological Basis of Therapeutics | Braunwald's Heart Disease | Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.