Explain emergency drugs that's adrenaline in detail it's mechanism how it's works and criteria ana protocols before giving in detail way
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
epinephrine adrenaline mechanism adrenergic receptor cardiac arrest anaphylaxis
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content. Let me compile the full, detailed answer:
Adrenaline (Epinephrine) — Complete Emergency Drug Reference

1. What Is Adrenaline?
Adrenaline (epinephrine) is an endogenous catecholamine synthesized by the adrenal medulla. In emergencies it is administered exogenously as a synthetic racemic preparation. It is the single most important drug in emergency medicine, with roles in:
- Anaphylaxis (first-line, only life-saving treatment)
- Cardiac arrest (ACLS/PALS — only vasopressor recommended)
- Symptomatic bradycardia refractory to atropine
- Septic/cardiogenic shock (vasopressor infusion)
- Severe bronchospasm
2. Mechanism of Action
Adrenaline is a non-selective adrenergic agonist, stimulating α₁, α₂, β₁, and β₂ receptors. The clinical effects follow directly from receptor pharmacology.
α₁-Adrenergic Effects (vasoconstriction)
| Effect | Clinical benefit |
|---|---|
| Peripheral vasoconstriction ↑ SVR | Raises blood pressure; reverses vasodilatory shock |
| Coronary and cerebral vasoconstriction (high dose) | Directs blood to core during CPR |
| Mucosal vasoconstriction | Reduces angioedema / laryngeal swelling |
α₂-Adrenergic Effects
- Pre-synaptic feedback inhibition of noradrenaline release (minor clinical relevance at therapeutic doses)
β₁-Adrenergic Effects (cardiac stimulation)
| Effect | Clinical benefit |
|---|---|
| Positive inotropy (↑ force of contraction) | Raises cardiac output |
| Positive chronotropy (↑ heart rate) | Increases minute output |
| Positive dromotropy (↑ AV conduction) | Useful in bradycardia/heart block |
| Increased automaticity | Can restore rhythm in asystole/PEA |
β₂-Adrenergic Effects (bronchodilation + metabolic)
| Effect | Clinical benefit |
|---|---|
| Bronchial smooth muscle relaxation | Reverses bronchoconstriction |
| Inhibits mast cell degranulation | Stops ongoing mediator release in anaphylaxis |
| Glycogenolysis, lipolysis | Metabolic stress response |
| Vasodilation (skeletal muscle) | At low doses, mild BP decrease |
Cellular Signal Transduction (β-receptor pathway)
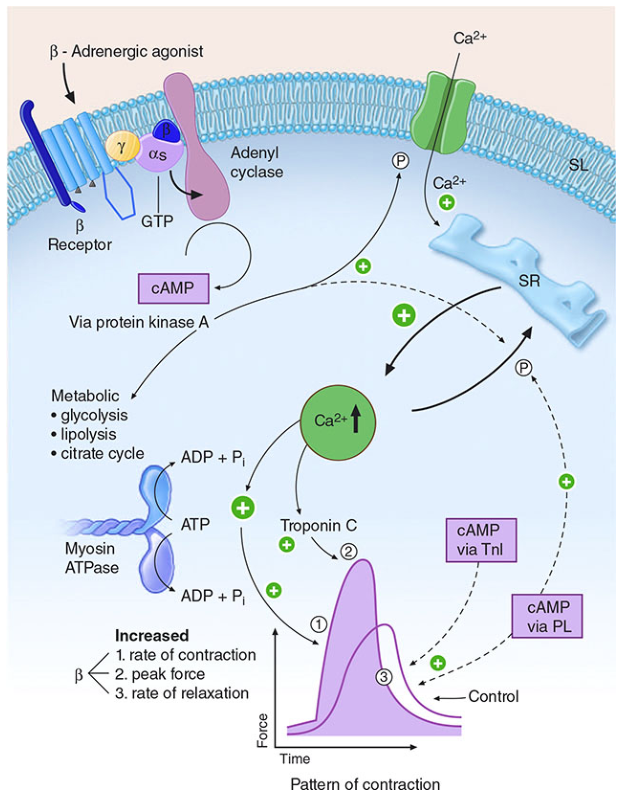
The β-receptor couples to a Gs protein → activates adenylyl cyclase → generates cAMP → activates Protein Kinase A (PKA) → phosphorylates:
- L-type Ca²⁺ channels → increased Ca²⁺ influx
- Ryanodine receptors on the sarcoplasmic reticulum → increased Ca²⁺ release
- Troponin I → accelerates calcium dissociation (faster relaxation)
- Phospholamban → enhances SR calcium re-uptake
- Myosin ATPase → more ATP hydrolysis → faster cross-bridge cycling
Net result: increased rate of contraction, peak force, and rate of relaxation (lusitropy).
"The α-adrenergic action (vasoconstriction) increases SVR and PVR. The resultant higher aortic diastolic blood pressure improves coronary perfusion pressure and myocardial blood flow... Epinephrine also increases cerebral blood flow during good-quality CPR because peripheral vasoconstriction directs more flow to the cerebral circulation." — Miller's Anesthesia, 10e
3. Pharmacokinetics
| Parameter | Detail |
|---|---|
| Onset (IV) | 1–2 minutes |
| Onset (IM) | 3–8 minutes |
| Half-life | ~2–3 minutes (rapidly metabolized by COMT and MAO) |
| Metabolism | Liver, kidney, plasma — methylation (COMT) + oxidative deamination (MAO) |
| Excretion | Renal (as inactive metabolites: metanephrine, VMA) |
| Stability | Inactivated by alkaline solutions — never mix with sodium bicarbonate |
4. Clinical Indications, Criteria, and Protocols
A. ANAPHYLAXIS
Diagnostic Criteria (Table 14-1, Tintinalli's Emergency Medicine)
Anaphylaxis is highly likely when ANY ONE of the following three criteria is met:
Criterion 1: Acute onset of illness (minutes to hours) with skin or mucosal involvement (urticaria, flushing, generalised itching, lip/tongue/uvula edema) AND at least one of:
- Respiratory distress or hypoxia
- Hypotension or cardiovascular collapse
- Associated organ dysfunction (hypotonia, syncope, incontinence)
Criterion 2: Two or more of the following occurring minutes to hours after allergen exposure:
- Skin and/or mucosal involvement
- Respiratory compromise
- Hypotension or associated symptoms
- Persistent GI cramps or vomiting
Criterion 3: Hypotension after exposure to a known allergen for that patient (even without skin signs)
Common Triggers
Drugs (β-lactams, NSAIDs, vancomycin), foods (nuts, shellfish, eggs), insect stings, latex, contrast media, blood products.
Clinical Features by System
| System | Signs/Symptoms | Incidence |
|---|---|---|
| Skin | Urticaria, angioedema, flushing, pruritus | 60–90% |
| Respiratory | Wheezing, laryngeal edema, stridor, rhinitis | 45–60% |
| ENT | Throat fullness, tongue swelling, uvular edema | 50% |
| Cardiovascular | Hypotension, chest pain | 30–35% |
| GI | Nausea, vomiting, cramps, diarrhea | 25–30% |
| Neuro | Headache, seizure | 5–8% |
Anaphylaxis Treatment Protocol
Step 1 — Immediate Assessment (ABC)
- Airway: examine for angioedema, stridor → intubate early if airway threatened (do not delay — progressive edema can make intubation impossible)
- Breathing: SpO₂ monitoring, O₂ to maintain saturation >90%
- Circulation: IV access, cardiac monitor, BP
Step 2 — Decontamination
- Stop the offending agent if identifiable (stop drug infusion, remove stinger)
- Do NOT perform gastric lavage for food allergens
Step 3 — EPINEPHRINE (FIRST-LINE — given immediately)
"Epinephrine is the first-line, most effective treatment for anaphylaxis." — Tintinalli's EM
| Route | Dose | Concentration | Notes |
|---|---|---|---|
| IM (preferred) | 0.3–0.5 mg (adult) | 1:1000 (1 mg/mL) | Anterolateral thigh — fastest absorption |
| IM (child) | 0.01 mg/kg (max 0.5 mg) | 1:1000 | |
| Autoinjector (EpiPen) | 0.3 mg adult / 0.15 mg child | 1:1000 | |
| IV (severe/arrest) | 0.1–0.5 mg bolus | 1:10,000 (0.1 mg/mL) | Only in cardiovascular collapse with IV access |
| IV infusion | 1 mg in 500 mL NS; start 2–10 mcg/min | Titrate to BP |
- Repeat IM dose every 5–15 minutes if no response
- IM into the anterolateral thigh gives faster and more reliable absorption than deltoid or subcutaneous routes
Why does epinephrine work in anaphylaxis?
- α₁: Constricts blood vessels → reverses hypotension and reduces mucosal edema/angioedema
- β₁: Positive inotropy/chronotropy → supports cardiac output
- β₂: Bronchodilation → reverses bronchoconstriction; also inhibits mast cell degranulation → stops further mediator release
Step 4 — IV Fluids
- Bolus 1–2 L NS (or LR) rapidly for hypotension
- Massive fluid shifts occur due to increased vascular permeability
Step 5 — Second-Line Agents (adjuncts only — do NOT replace epinephrine)
| Drug | Dose | Role |
|---|---|---|
| Diphenhydramine (H₁ blocker) | 25–50 mg IV/IM | Reduces urticaria/pruritus; does NOT treat hypotension or respiratory compromise |
| Ranitidine/famotidine (H₂ blocker) | 50 mg IV | H₂ blockade complements H₁ |
| Methylprednisolone | 125 mg IV | Prevents biphasic reaction; onset delayed 4–6 h |
| Salbutamol (nebulised) | 2.5–5 mg | Persistent bronchospasm after epinephrine |
| Glucagon | 1–2 mg IV | Critical in β-blocker patients who are resistant to epinephrine's β effects |
Special Consideration — β-Blockers:
Patients on β-blockers may have blunted response to epinephrine. Give glucagon 1–2 mg IV as it bypasses adrenergic receptors and directly activates adenylyl cyclase. Consider atropine for bradycardia. Switch β-blocker to another class at discharge.
Biphasic Reaction Risk:
- Occurs 3–11 hours after initial episode in 1–20% of patients
- Observe all anaphylaxis patients for minimum 4–6 hours (8–12 hours if severe)
- Discharge with prescription for ≥2 epinephrine autoinjectors, antihistamines (5 days), prednisolone (40–60 mg/day for 3–5 days), and allergy referral
B. CARDIAC ARREST
Indications
- Ventricular fibrillation (VF) or pulseless VT — unresponsive to initial shock
- Asystole
- Pulseless electrical activity (PEA)
- Profoundly symptomatic bradycardia (when atropine fails)
Mechanism in Cardiac Arrest
"Epinephrine may provide the most benefit within the first 15 to 20 minutes of cardiac arrest during the circulatory phase, based on its alpha effects of increasing peripheral vasoconstriction and coronary and cerebral blood flow." — Tintinalli's EM
- α₁ vasoconstriction raises aortic diastolic pressure → increases coronary perfusion pressure (CPP) → critical determinant of ROSC
- β₁ stimulation increases automaticity and contractile force if any cardiac activity present
- Adverse: May worsen myocardial ischemia, increase O₂ demand, induce ventricular ectopy, and cause cerebral vasoconstriction (worsening neurologic outcomes especially after 20 min)
Cardiac Arrest Protocol (Adult — ACLS)
| Timing | Action |
|---|---|
| 0 min | Collapse → CPR (30:2 compressions:ventilations) |
| ASAP | Defibrillate if shockable rhythm (VF/pVT) |
| After 2nd shock / PEA/Asystole | Epinephrine 1 mg IV/IO |
| Every 3–5 min | Repeat epinephrine 1 mg IV/IO (no maximum number of doses) |
| Persistent VF/pVT | Add amiodarone 300 mg IV bolus after 3rd shock |
| ROSC achieved | Post-resuscitation care |
Dose (Adult Cardiac Arrest):
- Standard: 1 mg (1:10,000 concentration = 10 mL) IV or IO
- Flush with ≥20 mL NS and elevate limb after each peripheral IV dose
- Repeat every 3–5 minutes
- High-dose epinephrine (2–5 mg) — no benefit over standard dose in survival; not recommended
Pediatric Cardiac Arrest:
- Dose: 0.01 mg/kg IV/IO (1:10,000), max 1 mg per dose
- Repeat every 3–5 minutes
- Evidence for early administration in non-shockable arrest: may not be effective if given >15 minutes after EMS arrival
Route Preference:
IV > IO > Central venous. The endotracheal route is no longer recommended (unreliable absorption due to pulmonary edema).
C. BRADYCARDIA (Non-Arrest)
Indication: Haemodynamically unstable bradycardia (hypotension, altered consciousness, chest pain, pulmonary edema) after atropine fails
IV Infusion Protocol:
- 1 mg in 500 mL NS
- Start at 2–10 mcg/min
- Titrate upward every 3–5 minutes to effect
- Monitor: HR, BP, ECG continuously
D. SEPTIC/CARDIOGENIC SHOCK
"The α causes vasoconstriction, while β has positive inotropic and chronotropic effects. At higher doses, epinephrine has a similar profile (at lower doses, the β effects predominate) but is associated with more adverse effects." — Harrison's Principles of Internal Medicine, 22e
- Used when noradrenaline is insufficient (second-line vasopressor in septic shock)
- Also used post-cardiac arrest for myocardial dysfunction
- Dose: Infusion titrated from 0.01–1 mcg/kg/min
- Higher doses → predominantly α effects (vasoconstriction)
- Lower doses → predominantly β effects (inotropy)
5. Adverse Effects
| Effect | Mechanism | Clinical Significance |
|---|---|---|
| Tachycardia | β₁ | Most common adverse effect |
| Hypertension | α₁ | Can precipitate stroke, pulmonary edema |
| Ventricular ectopy / VT | β₁ over-stimulation | Especially with high/prolonged doses |
| Myocardial ischemia | Increased O₂ demand, α coronary vasoconstriction | Risk in CAD patients |
| Pulmonary shunting | β₂ vasodilation | Worsens V/Q mismatch |
| Cerebral vasoconstriction | α₁ (high dose) | May worsen neurologic outcome post-arrest |
| Anxiety, tremor, headache | CNS/PNS stimulation | Common at lower doses |
| Hyperglycaemia | β₂ glycogenolysis | Monitor in diabetics |
| Tissue necrosis | α₁ extravasation | Use central/IO route; treat extravasation with phentolamine |
6. Contraindications and Cautions
| Situation | Consideration |
|---|---|
| Anaphylaxis | NO absolute contraindications — epinephrine is always given |
| Cardiac arrest | No absolute contraindications |
| Hypertension | Caution in non-emergency use |
| Coronary artery disease | Increased ischemia risk; caution with infusions |
| Hyperthyroidism | Enhanced sensitivity |
| β-blockers | Reduced β-response → give glucagon; α effects may be exaggerated |
| Alkaline IV solutions | Do not mix — inactivated |
| Pheochromocytoma | Relative CI — can precipitate hypertensive crisis |
7. Concentration Guide — Critical for Safety
| Concentration | Ratio | Use |
|---|---|---|
| 1 mg/mL | 1:1000 | Anaphylaxis (IM), nebulisation |
| 0.1 mg/mL | 1:10,000 | Cardiac arrest (IV), haemodynamic infusions |
| 0.01 mg/mL | 1:100,000 | Local anaesthesia additive |
⚠️ Medication error risk: Always confirm the concentration before administration. Administering 1:1000 IV instead of 1:10,000 delivers 10× the intended dose and can cause hypertensive crisis, arrhythmia, or death.
8. Summary — Decision Framework
EMERGENCY PRESENTATION
│
├── ANAPHYLAXIS?
│ ├── Epinephrine 0.3–0.5 mg IM (1:1000) anterolateral thigh
│ ├── Repeat q5–15 min if needed
│ ├── IV fluids, O₂, airway management
│ └── Antihistamines + corticosteroids (adjunct only)
│
├── CARDIAC ARREST (VF/pVT/PEA/Asystole)?
│ ├── CPR + defibrillation (shockable rhythm)
│ ├── Epinephrine 1 mg IV/IO (1:10,000)
│ ├── Repeat every 3–5 min
│ └── Amiodarone for refractory shockable rhythm
│
├── BRADYCARDIA (haemodynamically unstable, atropine failed)?
│ └── Epinephrine infusion 2–10 mcg/min IV, titrate
│
└── SEPTIC/CARDIOGENIC SHOCK (refractory)?
└── Epinephrine infusion 0.01–1 mcg/kg/min, titrate
Sources: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9e | Miller's Anesthesia, 10e | Harrison's Principles of Internal Medicine, 22e | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Fuster and Hurst's The Heart, 15e
Create a quick reference PDF on epinephrine dosing and protocols for emergency use
Reading File
Running Command
Running Command
Writing File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Create a comparison poster: Anaphylaxis vs Vasovagal Syncope mimickers
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.