Tomorrow is my psm practical exam of mbbs 2nd year from nepal. I dont know about RDA . External maam surely ask me RDA . Could you please provide me about RDA in easy language so that i will never forget it . And the external will impress
ICMR RDA recommended dietary allowance India 2020 PSM MBBS values table
RDA - Complete PSM Exam Guide (MBBS 2nd Year)
1. What is RDA? (The One-Line Answer)
RDA (Recommended Dietary Allowance) is the average daily dietary intake of a nutrient that is sufficient to meet the nutritional requirements of nearly all (97-98%) healthy individuals of a specific age, sex, and physiological state.
- Lippincott Biochemistry, 8th ed.
2. The Big Picture - DRI Family (Must Know!)
| Short Form | Full Name | What it means | % covered |
|---|---|---|---|
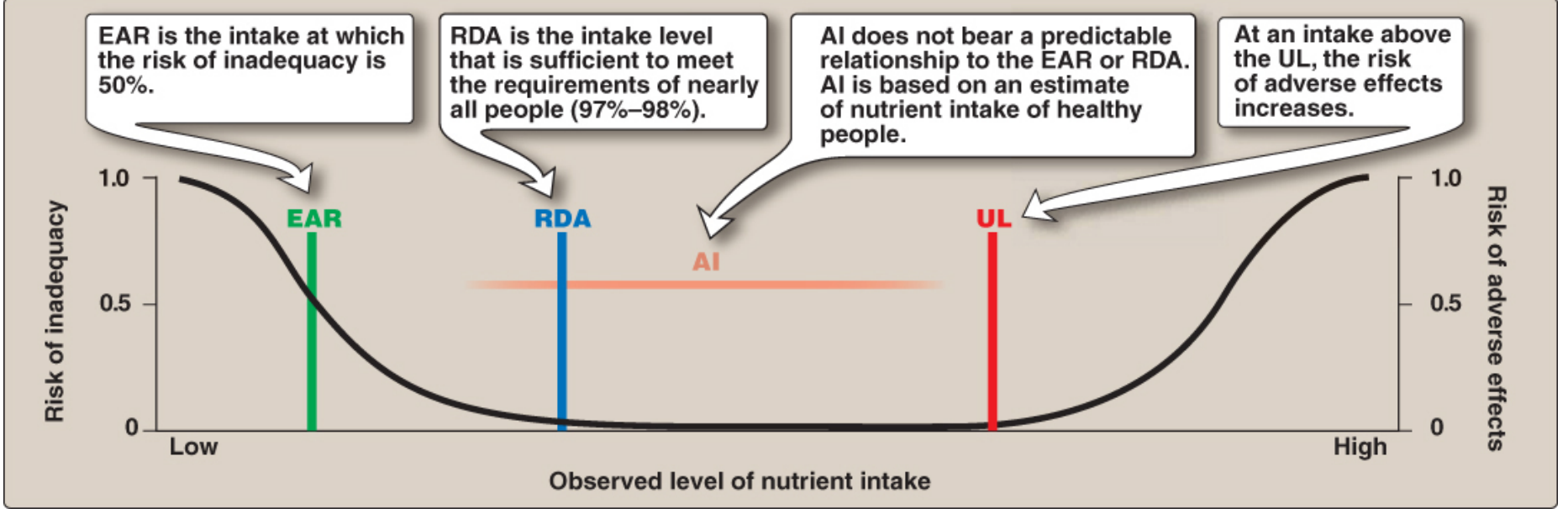
| EAR | Estimated Average Requirement | Meets needs of 50% of healthy people | 50% |
| RDA | Recommended Dietary Allowance | Meets needs of 97-98% of healthy people | 97-98% |
| AI | Adequate Intake | Used when EAR/RDA cannot be calculated | Not defined |
| UL | Tolerable Upper Intake Level | Maximum safe intake - above this, adverse effects start | - |
3. How is RDA Calculated? (Impress the Examiner!)
RDA = EAR + 2 SD (standard deviations)
- This is because RDA must cover 97-98% of people, which statistically = mean + 2 SD on a normal distribution curve.
- So RDA is always higher than EAR - it has a built-in safety margin.
- RDA is NOT the minimum requirement. It is an intentionally high value to ensure safety for almost everyone.
4. When is AI Used Instead of RDA?
5. ICMR RDA for Indians - The Key Values (Nepal follows ICMR/WHO standards)
Energy (Moderate work - most commonly asked)
| Group | Energy (kcal/day) |
|---|---|
| Adult Man (moderate work) | 2710 kcal |
| Adult Woman (moderate work) | 2130 kcal |
| Pregnant woman (2nd trimester extra) | +350 kcal |
| Lactating woman (0-6 months extra) | +600 kcal |
Protein
| Group | Protein (g/day) | Formula |
|---|---|---|
| Adult Man | 54 g | 0.83 g/kg/day |
| Adult Woman | 46 g | 0.83 g/kg/day |
| Pregnant (2nd trimester) | +9.5 g extra | |
| Pregnant (3rd trimester) | +22 g extra | |
| Lactating (0-6 months) | +17 g extra |
Note: ICMR 2020 changed protein RDA from 1.0 g/kg/day (old 2010 value) to 0.83 g/kg/day based on DIAAS (Digestible Indispensable Amino Acid Score) - this impresses examiners!
Key Minerals (ICMR 2020)
| Nutrient | Adult Man | Adult Woman | Pregnant | Lactating |
|---|---|---|---|---|
| Calcium | 1000 mg | 1000 mg | 1000 mg | 1200 mg |
| Iron | 19 mg | 29 mg | 35 mg | - |
| Zinc | 17 mg | 13 mg | 14.5 mg | 14 mg |
| Iodine | 150 µg | 150 µg | 200 µg | 200 µg |
Key Vitamins (ICMR 2020)
| Nutrient | Adult Man | Adult Woman |
|---|---|---|
| Vitamin A | 1000 µg | 840 µg |
| Vitamin C | 80 mg | 65 mg |
| Vitamin D | 600 IU | 600 IU |
| Folate | 300 µg | 220 µg |
| Vitamin B12 | 2.2 µg | 2.2 µg |
6. Important Concepts to Say Out Loud in the Exam
Who sets RDA?
- In India/Nepal: ICMR-NIN (Indian Council of Medical Research - National Institute of Nutrition), last revised in 2020
- In the USA: Institute of Medicine (IOM) / National Academies
- For international use: WHO/FAO
RDA vs EAR - The Key Difference
- EAR satisfies 50% of people - useful for assessing population groups
- RDA satisfies 97-98% of people - useful for planning diets for individuals
- If someone's intake is at or above RDA → their diet is adequate
- If intake is below EAR → definitely inadequate
RDA is NOT:
- The minimum requirement
- The optimal requirement
- The same for everyone (it varies by age, sex, physiological state like pregnancy/lactation)
7. Factors that Affect RDA (Determinants)
| Factor | Effect |
|---|---|
| Age | Children, adolescents, elderly have different values |
| Sex | Men and women differ (e.g., iron - women need more due to menstruation) |
| Pregnancy | Increased requirements for almost all nutrients |
| Lactation | Extra energy, protein, calcium needed |
| Physical activity | More activity = more energy needed |
| Physiological state | Illness, malabsorption affect needs |
| Bioavailability | Nutrient form and food matrix affect absorption (e.g., iron from plant foods = lower bioavailability) |
8. Uses / Importance of RDA (Common Viva Question)
- Planning diets for individuals and groups
- Evaluating nutritional adequacy of existing diets
- Formulating food and nutrition policies at national level
- Planning supplementation programs (e.g., iron-folic acid tablets for pregnant women)
- Food labeling - percent daily values on food packages
- Research - baseline for nutrition studies
- Targeted interventions for vulnerable groups (children, pregnant women)
9. Quick One-Liners to Impress the Examiner
- "RDA = EAR + 2 SD, providing a safety margin for 97-98% of the population"
- "ICMR revised the RDA in 2020, changing protein from 1 g/kg/day to 0.83 g/kg/day based on DIAAS"
- "When EAR cannot be established, AI is used instead of RDA - for example, in infants under 6 months"
- "RDA for iron in women is higher than men (29 vs 19 mg/day) due to menstrual losses"
- "UL is not the same as toxic dose - it is the highest safe average daily intake"
10. Super-Short Summary to Memorize Tonight
RDA = Average daily intake sufficient for 97-98% healthy people
= EAR + 2 SD
= Part of DRI system: EAR → RDA → AI → UL
= Set by ICMR-NIN for India (latest: 2020)
Key values (adult, moderate work):
Energy: Man 2710, Woman 2130 kcal/day
Protein: Man 54g, Woman 46g (0.83 g/kg/day)
Calcium: 1000 mg/day
Iron: Man 19 mg, Woman 29 mg/day
Vitamin D: 600 IU/day
Create a quick reference PDF summary of RDA values I can print tonight
Create a quick reference PDF summary of RDA
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
mkdir -p /home/daytona/workspace/rda-summary && python3 -c "from reportlab.lib import colors; print('reportlab ok')"
~/rda-summary/generate_rda_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.pdfbase import pdfmetrics
OUTPUT = "/home/daytona/workspace/rda-summary/RDA_Quick_Reference.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=1.5*cm,
leftMargin=1.5*cm,
topMargin=1.5*cm,
bottomMargin=1.5*cm,
)
W, H = A4
styles = getSampleStyleSheet()
# ── Custom styles ─────────────────────────────────────────────────────────────
BLUE = colors.HexColor("#1565C0")
DARK_BLUE = colors.HexColor("#0D47A1")
LIGHT_BLUE = colors.HexColor("#E3F2FD")
GREEN = colors.HexColor("#1B5E20")
LIGHT_GREEN= colors.HexColor("#E8F5E9")
ORANGE = colors.HexColor("#E65100")
ORANGE_BG = colors.HexColor("#FFF3E0")
RED = colors.HexColor("#B71C1C")
RED_BG = colors.HexColor("#FFEBEE")
GREY_BG = colors.HexColor("#F5F5F5")
HEADER_BG = colors.HexColor("#1565C0")
ALT_ROW = colors.HexColor("#EEF4FF")
title_style = ParagraphStyle(
"Title", parent=styles["Normal"],
fontSize=20, fontName="Helvetica-Bold",
textColor=colors.white, alignment=TA_CENTER,
spaceAfter=2,
)
subtitle_style = ParagraphStyle(
"Subtitle", parent=styles["Normal"],
fontSize=10, fontName="Helvetica",
textColor=colors.HexColor("#BBDEFB"), alignment=TA_CENTER,
spaceAfter=0,
)
section_style = ParagraphStyle(
"Section", parent=styles["Normal"],
fontSize=11, fontName="Helvetica-Bold",
textColor=colors.white, alignment=TA_LEFT,
spaceAfter=0, spaceBefore=0,
leftIndent=6,
)
body_style = ParagraphStyle(
"Body", parent=styles["Normal"],
fontSize=8.5, fontName="Helvetica",
textColor=colors.HexColor("#212121"),
spaceAfter=2, leading=12,
)
bold_style = ParagraphStyle(
"Bold", parent=styles["Normal"],
fontSize=8.5, fontName="Helvetica-Bold",
textColor=colors.HexColor("#212121"),
spaceAfter=2,
)
formula_style = ParagraphStyle(
"Formula", parent=styles["Normal"],
fontSize=10, fontName="Helvetica-Bold",
textColor=ORANGE, alignment=TA_CENTER,
spaceAfter=4, spaceBefore=4,
borderPad=4,
)
note_style = ParagraphStyle(
"Note", parent=styles["Normal"],
fontSize=7.5, fontName="Helvetica-Oblique",
textColor=colors.HexColor("#555555"),
spaceAfter=2, leftIndent=4,
)
footer_style = ParagraphStyle(
"Footer", parent=styles["Normal"],
fontSize=7, fontName="Helvetica",
textColor=colors.HexColor("#9E9E9E"), alignment=TA_CENTER,
)
tip_style = ParagraphStyle(
"Tip", parent=styles["Normal"],
fontSize=8, fontName="Helvetica-Bold",
textColor=GREEN, spaceAfter=1,
)
def section_header(text, bg=HEADER_BG):
t = Table([[Paragraph(text, section_style)]], colWidths=[doc.width])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("ROWBACKGROUNDS", (0,0), (-1,-1), [bg]),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS", [4,4,4,4]),
]))
return t
def make_table(headers, rows, col_widths, alt=True):
header_row = [Paragraph(f"<b>{h}</b>", ParagraphStyle(
"TH", parent=styles["Normal"], fontSize=8, fontName="Helvetica-Bold",
textColor=colors.white, alignment=TA_CENTER
)) for h in headers]
data = [header_row]
for i, row in enumerate(rows):
styled = []
for j, cell in enumerate(row):
align = TA_CENTER if j > 0 else TA_LEFT
styled.append(Paragraph(str(cell), ParagraphStyle(
"TD", parent=styles["Normal"], fontSize=8, fontName="Helvetica",
textColor=colors.HexColor("#212121"), alignment=align
)))
data.append(styled)
row_bgs = []
for i in range(1, len(data)):
bg = ALT_ROW if (alt and i % 2 == 0) else colors.white
row_bgs.append(bg)
t = Table(data, colWidths=col_widths)
ts = TableStyle([
("BACKGROUND", (0,0), (-1,0), DARK_BLUE),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#BDBDBD")),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING",(0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
])
for i, bg in enumerate(row_bgs, start=1):
ts.add("ROWBACKGROUNDS", (0,i), (-1,i), [bg])
t.setStyle(ts)
return t
# ── Title Banner ───────────────────────────────────────────────────────────────
def title_banner():
banner_data = [[
Paragraph("RDA - Quick Reference Sheet", title_style),
],[
Paragraph("PSM Practical Exam | MBBS 2nd Year | ICMR-NIN 2020 Guidelines", subtitle_style),
]]
t = Table(banner_data, colWidths=[doc.width])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS", [6,6,6,6]),
]))
return t
# ─────────────────────────────────────────────────────────────────────────────
story = []
# TITLE
story.append(title_banner())
story.append(Spacer(1, 6))
# ── SECTION 1: Definition & DRI Family ───────────────────────────────────────
story.append(section_header("1. DEFINITION"))
story.append(Spacer(1, 4))
def_box_data = [[Paragraph(
"<b>RDA</b> = The average daily dietary intake level sufficient to meet the nutritional "
"requirements of <b>nearly all (97–98%)</b> healthy individuals of a specific age, sex, "
"and physiological state.",
ParagraphStyle("Def", parent=styles["Normal"], fontSize=9, fontName="Helvetica",
textColor=DARK_BLUE, leading=13)
)]]
def_box = Table(def_box_data, colWidths=[doc.width])
def_box.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_BLUE),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
("BOX", (0,0), (-1,-1), 1, BLUE),
]))
story.append(def_box)
story.append(Spacer(1, 5))
# Formula box
formula_data = [[Paragraph("RDA = EAR + 2 SD (covers 97–98% of population)", formula_style)]]
fbox = Table(formula_data, colWidths=[doc.width])
fbox.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), ORANGE_BG),
("BOX", (0,0), (-1,-1), 1.5, ORANGE),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING",(0,0), (-1,-1), 6),
]))
story.append(fbox)
story.append(Spacer(1, 5))
# ── DRI Table ─────────────────────────────────────────────────────────────────
story.append(section_header("2. DRI FAMILY — 4 COMPONENTS (Remember: EAR → RDA → AI → UL)"))
story.append(Spacer(1, 4))
dri_rows = [
["EAR", "Estimated Average Requirement", "Meets needs of 50% of healthy people", "Assess population groups"],
["RDA", "Recommended Dietary Allowance", "Meets needs of 97–98% of healthy people", "Plan individual diets"],
["AI", "Adequate Intake", "Used when EAR/RDA cannot be calculated", "Infants, nutrients with insufficient data"],
["UL", "Tolerable Upper Intake Level", "Highest safe average daily intake", "Avoid toxicity from supplements"],
]
story.append(make_table(
["Term", "Full Form", "Covers", "Use"],
dri_rows,
[1.2*cm, 4.5*cm, 6*cm, 5.1*cm],
))
story.append(Spacer(1, 3))
story.append(Paragraph(
"* EAR is set first → RDA is derived from EAR. "
"If EAR cannot be set → use AI instead of RDA. "
"Above UL → risk of adverse effects increases.",
note_style
))
story.append(Spacer(1, 6))
# ── SECTION 3: Energy & Protein ──────────────────────────────────────────────
story.append(section_header("3. ENERGY & PROTEIN RDA (ICMR-NIN 2020)"))
story.append(Spacer(1, 4))
# Energy table
story.append(Paragraph("<b>ENERGY</b>", bold_style))
energy_rows = [
["Adult Man", "Sedentary", "2110", "—", "—"],
["Adult Man", "Moderate ★", "2710", "—", "—"],
["Adult Man", "Heavy", "3470", "—", "—"],
["Adult Woman", "Sedentary", "1660", "—", "—"],
["Adult Woman", "Moderate ★", "2130", "—", "—"],
["Adult Woman", "Heavy", "2720", "—", "—"],
["Pregnant", "2nd Trimester", "+350", "—", "—"],
["Pregnant", "3rd Trimester", "+350", "—", "—"],
["Lactating", "0–6 months", "+600", "—", "—"],
["Lactating", "7–12 months","+ 520","—", "—"],
]
# Simpler energy table
e_rows = [
["Adult Man", "Sedentary / Moderate ★ / Heavy", "2110 / 2710 / 3470 kcal"],
["Adult Woman", "Sedentary / Moderate ★ / Heavy", "1660 / 2130 / 2720 kcal"],
["Pregnant", "Extra (2nd / 3rd trimester)", "+350 / +350 kcal"],
["Lactating", "Extra (0–6 m / 7–12 m)", "+600 / +520 kcal"],
["Children 1–3 y","—", "1010 kcal"],
["Children 4–6 y","—", "1360 kcal"],
["Children 7–9 y","—", "1700 kcal"],
]
story.append(make_table(
["Group", "Activity Level", "Energy (kcal/day)"],
e_rows,
[4*cm, 5.5*cm, 7.3*cm],
))
story.append(Spacer(1, 4))
# Protein table
story.append(Paragraph("<b>PROTEIN</b> (RDA = 0.83 g/kg/day — revised down from 1.0 g/kg in 2010)", bold_style))
p_rows = [
["Adult Man (60 kg)", "54 g/day"],
["Adult Woman (55 kg)", "46 g/day"],
["Pregnant — 2nd trimester extra", "+9.5 g/day"],
["Pregnant — 3rd trimester extra", "+22 g/day"],
["Lactating 0–6 months extra", "+17 g/day"],
["Lactating 7–12 months extra", "+13 g/day"],
["Infants 0–6 months", "8.0 g/day"],
["Children 1–3 y", "12.5 g/day"],
["Children 4–6 y", "16.0 g/day"],
]
story.append(make_table(
["Group", "Protein RDA"],
p_rows,
[10*cm, 6.8*cm],
))
story.append(Spacer(1, 3))
story.append(Paragraph(
"★ = Moderate work is the standard reference. ICMR 2020 uses DIAAS (Digestible Indispensable Amino Acid Score) "
"instead of PDCAAS, and a cereal:legume:milk ratio of 3:1:2.5.",
note_style
))
story.append(Spacer(1, 6))
# ── SECTION 4: Key Minerals ───────────────────────────────────────────────────
story.append(section_header("4. KEY MINERALS (ICMR-NIN 2020)", bg=colors.HexColor("#1B5E20")))
story.append(Spacer(1, 4))
min_rows = [
["Calcium (mg)", "1000", "1000", "1000", "1200", "300 (infant)"],
["Iron (mg)", "19", "29 ★", "35", "—", "—"],
["Zinc (mg)", "17", "13", "14.5", "14", "2.5 (6–12 m)"],
["Iodine (µg)", "150", "150", "200", "200", "90"],
["Magnesium (mg)","440", "370", "—", "—", "—"],
["Phosphorus (mg)","1000","1000", "1000", "1000", "450 (infant)"],
["Sodium (mg)", "2000", "2000", "2000", "2000", "—"],
]
story.append(make_table(
["Mineral", "Man", "Woman ★", "Pregnant", "Lactating", "Child/Infant"],
min_rows,
[3.5*cm, 2*cm, 2.5*cm, 2.5*cm, 2.5*cm, 3.8*cm],
))
story.append(Spacer(1, 3))
story.append(Paragraph(
"★ Iron for women is higher (29 mg) than men (19 mg) due to menstrual losses — frequently asked in viva!",
note_style
))
story.append(Spacer(1, 6))
# ── SECTION 5: Key Vitamins ───────────────────────────────────────────────────
story.append(section_header("5. KEY VITAMINS (ICMR-NIN 2020)", bg=colors.HexColor("#4A148C")))
story.append(Spacer(1, 4))
vit_rows = [
["Vitamin A (µg)", "1000", "840", "1000", "1950"],
["Vitamin D (IU)", "600", "600", "600", "600"],
["Vitamin C (mg)", "80", "65", "80", "95"],
["Folate (µg DFE)", "300", "220", "500", "300"],
["Vitamin B12 (µg)", "2.2", "2.2", "2.2", "2.2"],
["Thiamine (mg)", "1.8", "1.7", "2.0", "1.9"],
["Riboflavin (mg)", "2.5", "2.4", "2.5", "2.5"],
["Niacin (mg)", "18", "14", "18", "17"],
["Vitamin B6 (mg)", "2.4", "1.9", "2.5", "2.5"],
["Vitamin E (mg)", "10", "8", "10", "12"],
["Vitamin K (µg)", "55", "55", "55", "55"],
]
story.append(make_table(
["Vitamin", "Man", "Woman", "Pregnant", "Lactating"],
vit_rows,
[4*cm, 2.5*cm, 2.5*cm, 3*cm, 3*cm], # adjusted for margins
))
story.append(Spacer(1, 3))
story.append(Paragraph(
"Note: Vitamin D 600 IU for all adults; >70 years = 800 IU. "
"Folate 500 µg in pregnancy (prevents neural tube defects).",
note_style
))
story.append(Spacer(1, 6))
# ── SECTION 6: Who Sets RDA ───────────────────────────────────────────────────
story.append(section_header("6. WHO SETS RDA?", bg=colors.HexColor("#37474F")))
story.append(Spacer(1, 4))
who_rows = [
["India / Nepal", "ICMR-NIN", "2020 (latest)"],
["USA", "National Academies of Medicine (IOM)", "2010–2019 (varies by nutrient)"],
["International", "WHO / FAO", "Ongoing updates"],
["Europe", "EFSA (European Food Safety Authority)", "Ongoing updates"],
]
story.append(make_table(
["Country/Region", "Body", "Latest Version"],
who_rows,
[3.5*cm, 8*cm, 5.3*cm],
))
story.append(Spacer(1, 6))
# ── SECTION 7: Determinants ───────────────────────────────────────────────────
story.append(section_header("7. FACTORS AFFECTING RDA (Determinants)", bg=colors.HexColor("#BF360C")))
story.append(Spacer(1, 4))
det_rows = [
["Age", "Infants, adolescents, elderly have different needs"],
["Sex", "Men vs women differ (e.g., iron, calcium)"],
["Pregnancy", "Increased requirements for almost ALL nutrients"],
["Lactation", "Extra energy, protein, calcium, vitamins"],
["Physical Activity", "More activity = more energy needed"],
["Bioavailability", "Plant iron (non-haem) absorbed less → higher RDA"],
["Disease State", "Illness/malabsorption may alter requirements"],
["Nutrient Interactions", "E.g., Vitamin C enhances iron absorption"],
]
story.append(make_table(
["Factor", "Explanation"],
det_rows,
[4*cm, 12.8*cm],
))
story.append(Spacer(1, 6))
# ── SECTION 8: Uses of RDA ────────────────────────────────────────────────────
story.append(section_header("8. USES / IMPORTANCE OF RDA", bg=DARK_BLUE))
story.append(Spacer(1, 4))
uses_data = [
[
Paragraph("1. Plan individual diets\n2. Evaluate dietary adequacy\n3. National nutrition policy", body_style),
Paragraph("4. Food labeling (% daily values)\n5. Supplementation programs\n6. Research baseline", body_style),
Paragraph("7. School / hospital meal planning\n8. Targeting vulnerable groups\n9. Fortification programs", body_style),
]
]
uses_table = Table(uses_data, colWidths=[doc.width/3]*3)
uses_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_BLUE),
("BOX", (0,0), (-1,-1), 0.5, BLUE),
("INNERGRID", (0,0), (-1,-1), 0.5, colors.HexColor("#BDBDBD")),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING",(0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("VALIGN", (0,0), (-1,-1), "TOP"),
]))
story.append(uses_table)
story.append(Spacer(1, 6))
# ── SECTION 9: Exam Tips ──────────────────────────────────────────────────────
story.append(section_header("9. EXAM TIPS — SAY THESE TO IMPRESS THE EXAMINER!", bg=colors.HexColor("#1B5E20")))
story.append(Spacer(1, 4))
tips_data = [[Paragraph(
"✔ <b>\"RDA = EAR + 2 SD\"</b> — most students don't know this formula!\n"
"✔ <b>\"ICMR 2020 revised protein RDA from 1.0 g/kg to 0.83 g/kg using DIAAS\"</b> — shows you're updated.\n"
"✔ <b>\"Iron RDA for women (29 mg) is higher than men (19 mg) due to menstrual losses.\"</b>\n"
"✔ <b>\"AI is used instead of RDA when sufficient data is unavailable — e.g., infants <6 months.\"</b>\n"
"✔ <b>\"Folate RDA doubles in pregnancy (220→500 µg) to prevent neural tube defects.\"</b>\n"
"✔ <b>\"RDA is NOT the minimum requirement — it has a built-in safety margin above EAR.\"</b>",
ParagraphStyle("Tips", parent=styles["Normal"], fontSize=8.5, fontName="Helvetica",
textColor=colors.HexColor("#1B5E20"), leading=14)
)]]
tips_box = Table(tips_data, colWidths=[doc.width])
tips_box.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_GREEN),
("BOX", (0,0), (-1,-1), 1.5, GREEN),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING",(0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
]))
story.append(tips_box)
story.append(Spacer(1, 8))
# ── SECTION 10: Quick Memory Card ─────────────────────────────────────────────
story.append(section_header("10. RAPID RECALL CARD", bg=ORANGE))
story.append(Spacer(1, 4))
recall_data = [[Paragraph(
"<b>RDA</b> = 97–98% healthy individuals | <b>EAR</b> = 50% | <b>AI</b> = when no EAR | <b>UL</b> = max safe\n\n"
"<b>Key Values (Adult, Moderate Work):</b>\n"
"Energy: Man 2710 kcal | Woman 2130 kcal\n"
"Protein: Man 54 g | Woman 46 g (0.83 g/kg/day)\n"
"Ca: 1000 mg | Fe: Man 19 mg, Woman 29 mg | Zn: Man 17 mg, Woman 13 mg\n"
"Vit A: Man 1000 µg, Woman 840 µg | Vit D: 600 IU | Vit C: Man 80 mg, Woman 65 mg\n"
"Folate: 220 µg (→500 µg in pregnancy) | B12: 2.2 µg | Iodine: 150 µg\n\n"
"<b>Formula:</b> RDA = EAR + 2 SD | <b>Set by:</b> ICMR-NIN (India/Nepal), latest 2020",
ParagraphStyle("Recall", parent=styles["Normal"], fontSize=8.5, fontName="Helvetica",
textColor=colors.HexColor("#212121"), leading=13)
)]]
recall_box = Table(recall_data, colWidths=[doc.width])
recall_box.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), ORANGE_BG),
("BOX", (0,0), (-1,-1), 2, ORANGE),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING",(0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
]))
story.append(recall_box)
story.append(Spacer(1, 8))
# Footer
story.append(HRFlowable(width=doc.width, thickness=0.5, color=colors.HexColor("#BDBDBD")))
story.append(Spacer(1, 3))
story.append(Paragraph(
"PSM Practical Quick Reference | MBBS 2nd Year | ICMR-NIN 2020 | "
"Source: Lippincott Biochemistry 8e, ICMR-NIN 2020 Report | Generated by Orris",
footer_style
))
# BUILD
doc.build(story)
print(f"PDF saved to: {OUTPUT}")
cd /home/daytona/workspace/rda-summary && python3 generate_rda_pdf.py 2>&1
ls -lh /home/daytona/workspace/rda-summary/RDA_Quick_Reference.pdf
RDA Quick Reference
PDF Document · PDF
- Definition - highlighted box with the one-line answer
- DRI Family Table - EAR / RDA / AI / UL comparison
- Energy & Protein - all groups including pregnancy/lactation (ICMR 2020)
- Key Minerals Table - Ca, Fe, Zn, Iodine, Mg across Man/Woman/Pregnant/Lactating
- Key Vitamins Table - A, D, C, Folate, B12 and more
- Who Sets RDA - ICMR-NIN for India/Nepal (2020)
- Factors affecting RDA - determinants table
- Uses of RDA - 9 uses in 3 columns
- Exam Tips (green box) - 6 lines to impress the examiner
- Rapid Recall Card (orange box) - ultra-short cheat sheet for last-minute review
This pdf is not openinhg in my macbook m2
python3 -c " from pypdf import PdfReader try: r = PdfReader('/home/daytona/workspace/rda-summary/RDA_Quick_Reference.pdf') print(f'Pages: {len(r.pages)}') print(r.pages[0].extract_text()[:200]) except Exception as e: print(f'Error: {e}') "
python3 -c " from pypdf import PdfReader, PdfWriter reader = PdfReader('/home/daytona/workspace/rda-summary/RDA_Quick_Reference.pdf') writer = PdfWriter() for page in reader.pages: writer.add_page(page) writer.add_metadata({ '/Title': 'RDA Quick Reference Sheet', '/Author': 'Orris', '/Subject': 'PSM MBBS 2nd Year', }) with open('/home/daytona/workspace/rda-summary/RDA_Quick_Reference_v2.pdf', 'wb') as f: writer.write(f) import os print('Size:', os.path.getsize('/home/daytona/workspace/rda-summary/RDA_Quick_Reference_v2.pdf')) "
which libreoffice && libreoffice --version 2>/dev/null || echo "not found"
~/rda-summary/RDA_Quick_Reference.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>RDA Quick Reference Sheet</title>
<style>
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: Arial, Helvetica, sans-serif;
font-size: 10px;
color: #212121;
background: #fff;
padding: 14px;
}
/* TITLE BANNER */
.title-banner {
background: #0D47A1;
color: white;
text-align: center;
padding: 10px 8px 8px;
border-radius: 6px;
margin-bottom: 8px;
}
.title-banner h1 { font-size: 18px; font-weight: bold; margin-bottom: 3px; }
.title-banner p { font-size: 9px; color: #BBDEFB; }
/* SECTION HEADERS */
.sec-header {
color: white;
font-size: 10px;
font-weight: bold;
padding: 5px 8px;
border-radius: 4px;
margin: 8px 0 5px;
}
.blue { background: #1565C0; }
.green { background: #1B5E20; }
.purple { background: #4A148C; }
.grey { background: #37474F; }
.red { background: #BF360C; }
.orange { background: #E65100; }
/* DEFINITION BOX */
.def-box {
background: #E3F2FD;
border: 1px solid #1565C0;
padding: 7px 10px;
border-radius: 4px;
font-size: 9.5px;
color: #0D47A1;
margin-bottom: 5px;
line-height: 1.5;
}
/* FORMULA BOX */
.formula-box {
background: #FFF3E0;
border: 2px solid #E65100;
padding: 6px;
text-align: center;
font-size: 12px;
font-weight: bold;
color: #E65100;
border-radius: 4px;
margin-bottom: 5px;
}
/* TABLES */
table {
width: 100%;
border-collapse: collapse;
margin-bottom: 4px;
font-size: 8.5px;
}
thead tr { background: #0D47A1; color: white; }
thead th { padding: 4px 5px; text-align: center; font-size: 8.5px; border: 1px solid #90A4AE; }
tbody td { padding: 3.5px 5px; border: 1px solid #CFD8DC; vertical-align: middle; }
tbody td:first-child { text-align: left; }
tbody td:not(:first-child) { text-align: center; }
tbody tr:nth-child(even) { background: #EEF4FF; }
tbody tr:nth-child(odd) { background: #ffffff; }
/* TIPS BOX */
.tips-box {
background: #E8F5E9;
border: 2px solid #1B5E20;
padding: 8px 10px;
border-radius: 4px;
font-size: 8.5px;
color: #1B5E20;
line-height: 1.8;
}
/* RECALL BOX */
.recall-box {
background: #FFF3E0;
border: 2px solid #E65100;
padding: 8px 10px;
border-radius: 4px;
font-size: 8.5px;
line-height: 1.7;
}
/* USES 3-COL */
.uses-grid {
display: grid;
grid-template-columns: 1fr 1fr 1fr;
gap: 0;
border: 1px solid #1565C0;
background: #E3F2FD;
border-radius: 4px;
overflow: hidden;
}
.uses-col {
padding: 6px 8px;
font-size: 8.5px;
border-right: 1px solid #90CAF9;
line-height: 1.8;
}
.uses-col:last-child { border-right: none; }
/* FOOTER */
.footer {
margin-top: 8px;
border-top: 1px solid #BDBDBD;
padding-top: 4px;
font-size: 7px;
color: #9E9E9E;
text-align: center;
}
.note { font-size: 7.5px; color: #555; font-style: italic; margin-top: 2px; margin-bottom: 2px; }
.bold-label { font-size: 9px; font-weight: bold; margin: 4px 0 2px; }
/* TWO COLUMN LAYOUT */
.two-col { display: grid; grid-template-columns: 1fr 1fr; gap: 8px; }
.col-block { }
</style>
</head>
<body>
<!-- TITLE -->
<div class="title-banner">
<h1>RDA — Quick Reference Sheet</h1>
<p>PSM Practical Exam | MBBS 2nd Year | ICMR-NIN 2020 Guidelines</p>
</div>
<!-- SECTION 1 -->
<div class="sec-header blue">1. DEFINITION</div>
<div class="def-box">
<b>RDA (Recommended Dietary Allowance)</b> = The average daily dietary intake level sufficient to meet the nutritional requirements of <b>nearly all (97–98%)</b> healthy individuals of a specific age, sex, and physiological state.
</div>
<div class="formula-box">RDA = EAR + 2 SD (covers 97–98% of population)</div>
<!-- SECTION 2 -->
<div class="sec-header blue">2. DRI FAMILY — 4 COMPONENTS (Remember: EAR → RDA → AI → UL)</div>
<table>
<thead><tr><th>Term</th><th>Full Form</th><th>Covers</th><th>Use For</th></tr></thead>
<tbody>
<tr><td><b>EAR</b></td><td>Estimated Average Requirement</td><td>50% of healthy people</td><td>Assess population groups</td></tr>
<tr><td><b>RDA</b></td><td>Recommended Dietary Allowance</td><td>97–98% of healthy people</td><td>Plan individual diets</td></tr>
<tr><td><b>AI</b></td><td>Adequate Intake</td><td>Used when EAR/RDA cannot be calculated</td><td>Infants; nutrients with insufficient data</td></tr>
<tr><td><b>UL</b></td><td>Tolerable Upper Intake Level</td><td>Max safe average daily intake</td><td>Avoid toxicity from supplements</td></tr>
</tbody>
</table>
<p class="note">* EAR is set first → RDA derived from EAR. If EAR cannot be set → use AI. Above UL → risk of adverse effects increases.</p>
<!-- SECTION 3 -->
<div class="sec-header blue">3. ENERGY & PROTEIN RDA (ICMR-NIN 2020)</div>
<div class="two-col">
<div class="col-block">
<p class="bold-label">ENERGY</p>
<table>
<thead><tr><th>Group</th><th>Activity</th><th>kcal/day</th></tr></thead>
<tbody>
<tr><td>Adult Man</td><td>Sedentary</td><td>2110</td></tr>
<tr><td>Adult Man</td><td><b>Moderate ★</b></td><td><b>2710</b></td></tr>
<tr><td>Adult Man</td><td>Heavy</td><td>3470</td></tr>
<tr><td>Adult Woman</td><td>Sedentary</td><td>1660</td></tr>
<tr><td>Adult Woman</td><td><b>Moderate ★</b></td><td><b>2130</b></td></tr>
<tr><td>Adult Woman</td><td>Heavy</td><td>2720</td></tr>
<tr><td>Pregnant</td><td>2nd / 3rd trim.</td><td>+350 / +350</td></tr>
<tr><td>Lactating</td><td>0–6 / 7–12 m</td><td>+600 / +520</td></tr>
<tr><td>Children 1–3 y</td><td>—</td><td>1010</td></tr>
<tr><td>Children 4–6 y</td><td>—</td><td>1360</td></tr>
<tr><td>Children 7–9 y</td><td>—</td><td>1700</td></tr>
</tbody>
</table>
</div>
<div class="col-block">
<p class="bold-label">PROTEIN <span style="font-weight:normal;font-size:7.5px;">(RDA = 0.83 g/kg/day; revised from 1.0 g/kg in 2010)</span></p>
<table>
<thead><tr><th>Group</th><th>Protein RDA</th></tr></thead>
<tbody>
<tr><td><b>Adult Man (60 kg)</b></td><td><b>54 g/day</b></td></tr>
<tr><td><b>Adult Woman (55 kg)</b></td><td><b>46 g/day</b></td></tr>
<tr><td>Pregnant — 2nd trimester extra</td><td>+9.5 g/day</td></tr>
<tr><td>Pregnant — 3rd trimester extra</td><td>+22 g/day</td></tr>
<tr><td>Lactating 0–6 m extra</td><td>+17 g/day</td></tr>
<tr><td>Lactating 7–12 m extra</td><td>+13 g/day</td></tr>
<tr><td>Infants 0–6 m</td><td>8.0 g/day</td></tr>
<tr><td>Children 1–3 y</td><td>12.5 g/day</td></tr>
<tr><td>Children 4–6 y</td><td>16.0 g/day</td></tr>
<tr><td>Boys 16–18 y</td><td>55 g/day</td></tr>
<tr><td>Girls 16–18 y</td><td>46 g/day</td></tr>
</tbody>
</table>
<p class="note">★ Moderate work is the standard reference. ICMR 2020 uses DIAAS (Digestible Indispensable Amino Acid Score).</p>
</div>
</div>
<!-- SECTION 4 -->
<div class="sec-header green">4. KEY MINERALS (ICMR-NIN 2020)</div>
<table>
<thead><tr><th>Mineral</th><th>Adult Man</th><th>Adult Woman</th><th>Pregnant</th><th>Lactating</th><th>Child / Infant</th></tr></thead>
<tbody>
<tr><td>Calcium (mg)</td><td>1000</td><td>1000</td><td>1000</td><td>1200</td><td>300–850 mg</td></tr>
<tr><td><b>Iron (mg) ★</b></td><td><b>19</b></td><td><b>29</b></td><td>35</td><td>—</td><td>5–18 mg</td></tr>
<tr><td>Zinc (mg)</td><td>17</td><td>13</td><td>14.5</td><td>14</td><td>2.5–14 mg</td></tr>
<tr><td>Iodine (µg)</td><td>150</td><td>150</td><td>200</td><td>200</td><td>90 µg</td></tr>
<tr><td>Magnesium (mg)</td><td>440</td><td>370</td><td>—</td><td>—</td><td>80–350 mg</td></tr>
<tr><td>Phosphorus (mg)</td><td>1000</td><td>1000</td><td>1000</td><td>1000</td><td>450 (infant)</td></tr>
<tr><td>Sodium (mg)</td><td>2000</td><td>2000</td><td>2000</td><td>2000</td><td>—</td></tr>
<tr><td>Fluoride (mg)</td><td>3.5</td><td>3.0</td><td>—</td><td>—</td><td>0.1–2 mg</td></tr>
</tbody>
</table>
<p class="note">★ Iron for women (29 mg) > men (19 mg) due to menstrual losses — very commonly asked in viva!</p>
<!-- SECTION 5 -->
<div class="sec-header purple">5. KEY VITAMINS (ICMR-NIN 2020)</div>
<table>
<thead><tr><th>Vitamin</th><th>Adult Man</th><th>Adult Woman</th><th>Pregnant</th><th>Lactating</th></tr></thead>
<tbody>
<tr><td>Vitamin A (µg)</td><td>1000</td><td>840</td><td>1000</td><td>1950</td></tr>
<tr><td><b>Vitamin D (IU)</b></td><td><b>600</b></td><td><b>600</b></td><td>600</td><td>600</td></tr>
<tr><td>Vitamin C (mg)</td><td>80</td><td>65</td><td>80</td><td>95</td></tr>
<tr><td><b>Folate (µg DFE) ★</b></td><td><b>300</b></td><td><b>220</b></td><td><b>500</b></td><td>300</td></tr>
<tr><td>Vitamin B12 (µg)</td><td>2.2</td><td>2.2</td><td>2.2</td><td>2.2</td></tr>
<tr><td>Thiamine B1 (mg)</td><td>1.8</td><td>1.7</td><td>2.0</td><td>1.9</td></tr>
<tr><td>Riboflavin B2 (mg)</td><td>2.5</td><td>2.4</td><td>2.5</td><td>2.5</td></tr>
<tr><td>Niacin B3 (mg)</td><td>18</td><td>14</td><td>18</td><td>17</td></tr>
<tr><td>Pyridoxine B6 (mg)</td><td>2.4</td><td>1.9</td><td>2.5</td><td>2.5</td></tr>
<tr><td>Vitamin E (mg)</td><td>10</td><td>8</td><td>10</td><td>12</td></tr>
<tr><td>Vitamin K (µg)</td><td>55</td><td>55</td><td>55</td><td>55</td></tr>
</tbody>
</table>
<p class="note">★ Folate doubles in pregnancy (220→500 µg) to prevent Neural Tube Defects. Vit D 800 IU for age >70 years.</p>
<!-- SECTION 6 + 7 side by side -->
<div class="two-col">
<div>
<div class="sec-header grey">6. WHO SETS RDA?</div>
<table>
<thead><tr><th>Country/Region</th><th>Body</th><th>Year</th></tr></thead>
<tbody>
<tr><td><b>India / Nepal</b></td><td><b>ICMR-NIN</b></td><td><b>2020</b></td></tr>
<tr><td>USA</td><td>National Academies (IOM)</td><td>2010–2019</td></tr>
<tr><td>International</td><td>WHO / FAO</td><td>Ongoing</td></tr>
<tr><td>Europe</td><td>EFSA</td><td>Ongoing</td></tr>
</tbody>
</table>
</div>
<div>
<div class="sec-header red">7. FACTORS AFFECTING RDA</div>
<table>
<thead><tr><th>Factor</th><th>Effect</th></tr></thead>
<tbody>
<tr><td>Age</td><td>Different values per life stage</td></tr>
<tr><td>Sex</td><td>Men vs women differ (e.g., iron)</td></tr>
<tr><td>Pregnancy</td><td>Increased for almost all nutrients</td></tr>
<tr><td>Lactation</td><td>Extra energy, protein, Ca</td></tr>
<tr><td>Physical Activity</td><td>More activity = more energy</td></tr>
<tr><td>Bioavailability</td><td>Plant iron absorbed less → higher RDA</td></tr>
<tr><td>Disease/Malabsorption</td><td>May alter requirements</td></tr>
</tbody>
</table>
</div>
</div>
<!-- SECTION 8 -->
<div class="sec-header blue">8. USES / IMPORTANCE OF RDA</div>
<div class="uses-grid">
<div class="uses-col">
1. Plan individual diets<br>
2. Evaluate dietary adequacy<br>
3. National nutrition policy
</div>
<div class="uses-col">
4. Food labeling (% daily values)<br>
5. Supplementation programs<br>
6. Research baseline
</div>
<div class="uses-col">
7. School/hospital meal planning<br>
8. Targeting vulnerable groups<br>
9. Food fortification programs
</div>
</div>
<!-- SECTION 9 -->
<div class="sec-header green">9. EXAM TIPS — SAY THESE TO IMPRESS THE EXAMINER!</div>
<div class="tips-box">
✔ <b>"RDA = EAR + 2 SD"</b> — most students don't know this formula!<br>
✔ <b>"ICMR 2020 revised protein RDA from 1.0 g/kg to 0.83 g/kg using DIAAS"</b> — shows you're updated.<br>
✔ <b>"Iron RDA for women (29 mg) > men (19 mg) due to menstrual losses."</b><br>
✔ <b>"AI is used when sufficient data is unavailable — e.g., infants under 6 months."</b><br>
✔ <b>"Folate RDA doubles in pregnancy (220→500 µg) to prevent neural tube defects."</b><br>
✔ <b>"RDA is NOT the minimum requirement — it has a built-in safety margin above EAR."</b>
</div>
<!-- SECTION 10 -->
<div class="sec-header orange">10. RAPID RECALL CARD</div>
<div class="recall-box">
<b>RDA</b> = 97–98% healthy individuals | <b>EAR</b> = 50% | <b>AI</b> = when no EAR | <b>UL</b> = max safe | Formula: <b>RDA = EAR + 2 SD</b><br><br>
<b>Key Values (Adult, Moderate Work):</b><br>
Energy: Man <b>2710</b> kcal | Woman <b>2130</b> kcal |
Protein: Man <b>54 g</b> | Woman <b>46 g</b> (0.83 g/kg/day)<br>
Ca: <b>1000 mg</b> | Fe: Man <b>19</b> mg, Woman <b>29</b> mg | Zn: Man <b>17</b> mg, Woman <b>13</b> mg | Iodine: <b>150</b> µg<br>
Vit A: Man <b>1000</b> µg, Woman <b>840</b> µg | Vit D: <b>600</b> IU | Vit C: Man <b>80</b> mg, Woman <b>65</b> mg<br>
Folate: <b>220</b> µg (→<b>500</b> µg pregnancy) | B12: <b>2.2</b> µg | Protein pregnancy 3rd trim extra: <b>+22 g</b><br><br>
<b>Set by:</b> ICMR-NIN (India/Nepal), latest revision <b>2020</b>
</div>
<div class="footer">
PSM Practical Quick Reference | MBBS 2nd Year | ICMR-NIN 2020 | Source: Lippincott Biochemistry 8e, ICMR-NIN 2020 Report | Generated by Orris
</div>
</body>
</html>
libreoffice --headless --convert-to pdf --outdir /home/daytona/workspace/rda-summary/ /home/daytona/workspace/rda-summary/RDA_Quick_Reference.html 2>&1
libreoffice --headless --convert-to pdf --outdir /tmp/ /home/daytona/workspace/rda-summary/RDA_Quick_Reference.html 2>&1 && ls -lh /tmp/RDA_Quick_Reference.pdf && cp /tmp/RDA_Quick_Reference.pdf /home/daytona/workspace/rda-summary/RDA_Quick_Reference_LO.pdf
python3 -c " from pypdf import PdfReader r = PdfReader('/home/daytona/workspace/rda-summary/RDA_Quick_Reference_LO.pdf') print(f'Pages: {len(r.pages)}') print(r.pages[0].extract_text()[:300]) "
RDA Quick Reference LO
PDF Document · PDF
RDA Quick Reference
HTML File · HTML
Tomorrow is my psm practical exam of mbbs 2nd year from nepal. I dont know about rubella and mumps . External maam surely ask me from this pptx . Could you please provide me about rubella and mumps in easy language so that i will never forget it . And the external will impress
python -m markitdown "/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Rubella (German measles).edited.pptx" 2>/dev/null
python -m markitdown "/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Mumps edited_4d0cd49a-4ee5-481f-9883-30fd52801478.pptx" 2>/dev/null
python3 -c " from pptx import Presentation import sys path = '/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Rubella (German measles).edited.pptx' prs = Presentation(path) for i, slide in enumerate(prs.slides): title = '' content = [] for shape in slide.shapes: if hasattr(shape, 'text') and shape.text.strip(): txt = shape.text.strip() if shape.shape_type == 13: continue content.append(txt) if content: print(f'=== SLIDE {i+1} ===') for c in content: print(c) print() " 2>&1 | head -300
python3 -c " from pptx import Presentation path = '/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Mumps edited_4d0cd49a-4ee5-481f-9883-30fd52801478.pptx' prs = Presentation(path) for i, slide in enumerate(prs.slides): content = [] for shape in slide.shapes: if hasattr(shape, 'text') and shape.text.strip(): if shape.shape_type == 13: continue content.append(shape.text.strip()) if content: print(f'=== SLIDE {i+1} ===') for c in content: print(c) print() " 2>&1 | head -300
pip install python-pptx --quiet --user 2>&1 | tail -3
python3 -c " from pptx import Presentation path = '/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Rubella (German measles).edited.pptx' prs = Presentation(path) for i, slide in enumerate(prs.slides): content = [] for shape in slide.shapes: if hasattr(shape, 'text') and shape.text.strip(): if shape.shape_type == 13: continue content.append(shape.text.strip()) if content: print(f'=== SLIDE {i+1} ===') for c in content: print(c) print() " 2>&1 | head -400
python3 -c " from pptx import Presentation path = '/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Mumps edited_4d0cd49a-4ee5-481f-9883-30fd52801478.pptx' prs = Presentation(path) for i, slide in enumerate(prs.slides): content = [] for shape in slide.shapes: if hasattr(shape, 'text') and shape.text.strip(): if shape.shape_type == 13: continue content.append(shape.text.strip()) if content: print(f'=== SLIDE {i+1} ===') for c in content: print(c) print() " 2>&1 | head -400
python3 -c " from pptx import Presentation path = '/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Rubella (German measles).edited.pptx' prs = Presentation(path) for i, slide in enumerate(prs.slides): content = [] for shape in slide.shapes: if hasattr(shape, 'text') and shape.text.strip(): if shape.shape_type == 13: continue for para in shape.text_frame.paragraphs if hasattr(shape, 'text_frame') else []: t = para.text.strip() if t: content.append(t) if content: print(f'=== SLIDE {i+1} ===') for c in content: print(c) print() " 2>&1
python3 -c " from pptx import Presentation path = '/home/daytona/workspace/attachments/089ac1f9-ca81-49be-b673-d52cd92941fa/Mumps edited_4d0cd49a-4ee5-481f-9883-30fd52801478.pptx' prs = Presentation(path) for i, slide in enumerate(prs.slides): content = [] for shape in slide.shapes: if hasattr(shape, 'text') and shape.text.strip(): if shape.shape_type == 13: continue for para in shape.text_frame.paragraphs if hasattr(shape, 'text_frame') else []: t = para.text.strip() if t: content.append(t) if content: print(f'=== SLIDE {i+1} ===') for c in content: print(c) print() " 2>&1
RUBELLA & MUMPS — Complete PSM Exam Guide 🎓
PART 1: RUBELLA (German Measles / जर्मन दादुरा)
1. What is Rubella?
Rubella is a mild, self-limiting viral illness caused by Rubella virus (RNA virus, Togavirus family) - also called "German Measles" or "3-day measles" (rash lasts only 3 days).
2. Epidemiology (Quick Facts)
| Feature | Detail |
|---|---|
| Causative agent | Rubella virus (RNA virus, Togavirus) |
| Reservoir | Humans only (no animal reservoir) |
| Source | Infected persons (including subclinical cases) |
| Transmission | Droplet infection (respiratory route) |
| Communicability | 7 days before to 7 days after rash appears |
| Incubation period | 14-21 days (average 18 days) |
| Contagiousness | Less contagious than measles |
| Seasonality | Late winter to early spring |
| Age group | Children 5-15 years most affected |
3. Clinical Features
In Children (Post-natal rubella):
- Rash - maculopapular, starts on face → trunk → limbs (centrifugal spread)
- Rash lasts only 3 days (hence "3-day measles")
- Mild or no fever (low-grade at most)
- Lymphadenopathy - occipital + post-auricular (behind the ear) lymph nodes enlarged and TENDER - this is the hallmark!
- No koplik spots (unlike measles)
- Rash is usually faint, mild, hard to detect in dark skin
In Adults (especially women):
- Arthralgia and arthritis (very common in adult women - a distinguishing feature!)
- Mild constitutional symptoms
Does rubella always present with rash? NO!
- Up to 50% of cases are subclinical (no rash, no symptoms)
- This makes rubella dangerous - infected women may not know they have it during pregnancy!
4. Measles vs Rubella (Your slide has this comparison - very commonly asked!)
| Feature | Measles | Rubella |
|---|---|---|
| Other name | Hard measles | German measles / 3-day measles |
| Virus | Paramyxovirus (Morbillivirus) | Togavirus |
| Rash duration | 4-7 days | 3 days |
| Rash type | Maculopapular, coalescent | Maculopapular, discrete |
| Koplik spots | Present (pathognomonic) | Absent |
| Lymphadenopathy | Cervical | Occipital + post-auricular |
| Fever | High | Low grade / absent |
| Incubation period | 10-12 days | 14-21 days (avg 18 days) |
| Severity | More severe | Milder |
| Danger in pregnancy | Less | Extremely dangerous (CRS) |
| Catarrhal stage | Present (3C's) | Absent |
5. Congenital Rubella Syndrome (CRS) ⭐ MOST IMPORTANT TOPIC
When does it occur?
- When a pregnant woman gets rubella, the virus crosses the placenta and damages the fetus
- Maximum damage in 1st trimester (especially first 8-12 weeks)
- After 16 weeks of pregnancy: NO major abnormalities (very important MCQ answer!)
Classic Triad of CRS (Gregg's Triad):
"CCC" = Cataract + Cardiac defects + Cochlear deafness
| System | Defect |
|---|---|
| Eyes | Congenital cataract, glaucoma, retinopathy |
| Heart | Patent Ductus Arteriosus (PDA), VSD, pulmonary artery stenosis |
| Ears | Sensorineural deafness (most common single defect) |
| Brain | Microcephaly, intellectual disability |
| Other | Hepatosplenomegaly, thrombocytopenic purpura ("blueberry muffin baby") |
Risk of CRS by trimester:
| Trimester | Risk of CRS |
|---|---|
| 1st (1-12 weeks) | Up to 90% - MOST DISASTROUS |
| 2nd (13-24 weeks) | 10-20% |
| After 16-20 weeks | Rare/no major defects |
6. Diagnosis
| Test | What it shows |
|---|---|
| IgM antibodies at birth | Confirms CRS in newborn (IgM does NOT cross placenta → if present = baby made it) |
| IgG antibodies persist >6 months | Also confirms CRS (maternal IgG disappears by 6 months; if still present = baby's own) |
| Virus isolation | From throat, urine, CSF |
| PCR | Detect viral RNA |
7. Prevention (Your slide: MMR Vaccine)
MMR Vaccine:
- Measles + Mumps + Rubella (live attenuated)
- Given at: 9 months + 15 months (Nepal/India schedule)
- Route: Subcutaneous
- Efficacy: ~95% after single dose
Rubella Vaccination Strategy (MCQ from your slide):
- During a rubella outbreak → vaccinate Women 15-49 years (non-pregnant) on PRIORITY
- Why women? Because the real danger is not rubella itself, but CRS in their future babies
- Pregnant women should NOT get MMR (live virus - theoretical risk)
- Conception should be delayed 1 month after MMR vaccination
Contraindications to MMR:
- Pregnancy (delay conception 1 month after vaccine)
- Severe immunocompromise
- Severe allergy to vaccine components
8. MCQ Answers from Your Slides
| Question | Answer | Key reason |
|---|---|---|
| Vaccination priority during rubella outbreak | Women 15-49 years (non-pregnant) | Prevent CRS |
| Max fetal damage in | 6-12 weeks pregnancy (1st trimester) | Organogenesis |
| Rubella incubation period | 14-21 days, avg 18 days (NOT <10 days) | Important exception |
| Infection after 16 weeks | No major abnormalities | Safe window |
| CRS diagnosed by | IgM at birth OR IgG persisting >6 months | Both correct |
PART 2: MUMPS
1. What is Mumps?
Mumps is an acute viral illness caused by Mumps virus (RNA virus, Paramyxovirus family - Rubulavirus genus) characterized by painful swelling of the parotid glands (parotitis).
2. Epidemiology
| Feature | Detail |
|---|---|
| Causative agent | Mumps virus (RNA virus, Paramyxovirus) |
| Reservoir | Humans only |
| Transmission | Droplet infection + direct contact with infected saliva |
| Incubation period | 16-18 days (range 12-25 days) - MCQ answer = 18 days |
| Communicability | 2 days before to 9 days after parotitis starts |
| Peak age | School-age children (5-14 years) |
| Seasonality | Late winter to spring |
| Immunity | Lifelong after natural infection |
3. Clinical Features
Prodrome (1-2 days before swelling):
- Fever, malaise, headache, anorexia
Main Sign - Parotitis:
- Painful swelling of parotid gland (in front of and below the ear)
- Usually bilateral (but can start unilateral then become bilateral)
- Swelling pushes the earlobe upward and outward
- Tender to touch
- Lasts about 7-10 days
- Stensen's duct opening (opposite upper 2nd molar) appears red and swollen
Clinical clue:
- Angle of the jaw is obliterated by swelling (unlike lymph node enlargement where you can feel the angle)
4. Complications (⭐ Most asked in exams)
Most Common Complication in CHILDREN = Aseptic Meningitis (MCQ answer from your slide!)
Most Common Complication overall = Orchitis (in post-pubertal males)
| Complication | Frequency (unvaccinated) | Key points |
|---|---|---|
| Aseptic meningitis | Up to 10% | Most common in children; self-limiting |
| Orchitis | 30% of post-pubertal males | Develops 1st week of parotitis; 30-50% testicular atrophy |
| Oophoritis | 7% of post-pubertal women | Ovarian inflammation |
| Pancreatitis | ~4% | Elevated amylase + lipase |
| Encephalitis | <1% | Mortality 1.5% |
| Hearing loss | Up to 4% | Usually unilateral, transient |
| Mastitis | 30% unvaccinated women | - |
Important about Orchitis:
- Occurs in 30% of unvaccinated post-pubertal males (only 6% if vaccinated)
- Develops in the 1st week of parotitis
- Both testes in 10-30% of cases
- 30-50% testicular atrophy but permanent infertility is RARE
- Causes fear but rarely leads to complete sterility
Important about Meningitis:
- Up to 55% have subclinical CSF pleocytosis (but no symptoms)
- Only ~10% unvaccinated patients develop symptomatic meningitis
- Self-limited (recovers fully)
5. Diagnosis
| Method | Detail |
|---|---|
| Clinical | Painful bilateral parotid swelling + epidemiological history |
| Serology | IgM antibodies in acute phase (diagnostic) |
| Elevated serum amylase | Suggests parotitis or pancreatitis |
| Elevated lipase (with amylase) | Suggests pancreatitis specifically |
| PCR | Virus from saliva, urine, CSF |
6. Management
- No specific antiviral treatment for mumps
- Symptomatic treatment only:
- Analgesics/antipyretics (paracetamol) for pain and fever
- Soft diet (chewing is painful)
- Warm/cold compresses on parotid area
- Rest and hydration
- For orchitis: bed rest, scrotal support, analgesics
7. Prevention
MMR Vaccine:
- Same vaccine as rubella: MMR (live attenuated)
- Given at 9 months + 15 months
- Two-dose MMR reduces mumps incidence by 97-99%
- One-dose MMR reduces incidence by 87-88%
- Vaccine strain used: Jeryl Lynn strain
Other measures:
- Isolation of cases for 9 days after onset of parotitis
- Avoid schools/crowded places during infectious period
8. MCQ Answers from Your Slides
| Question | Answer | Why |
|---|---|---|
| Most common complication of mumps in children | Aseptic meningitis | Orchitis is post-pubertal males only |
| Incubation period of mumps | 18 days | Range 12-25 days |
QUICK COMPARISON: RUBELLA vs MUMPS
| Feature | Rubella | Mumps |
|---|---|---|
| Virus family | Togavirus | Paramyxovirus (Rubulavirus) |
| Virus type | RNA | RNA |
| Incubation | 18 days (14-21) | 18 days (12-25) |
| Key sign | Rash + occipital LN | Parotitis (swollen cheeks) |
| Koplik spots | No | No |
| Most dangerous in | Pregnancy (CRS) | Post-pubertal males (orchitis) |
| Most common complication | Subclinical (50%) | Aseptic meningitis (children) / Orchitis (adults) |
| Vaccine | MMR (live attenuated) | MMR (live attenuated) |
| Treatment | Symptomatic | Symptomatic |
LINES TO IMPRESS THE EXAMINER 🌟
- "Both rubella and mumps are RNA viruses given via the same MMR live attenuated vaccine at 9 and 15 months."
- "Up to 50% of rubella cases are subclinical - this is why pregnant women can unknowingly infect their fetus."
- "CRS triad = Cataract + Cardiac defect (PDA) + Cochlear deafness (Gregg's triad)."
- "During rubella outbreak, we vaccinate non-pregnant women aged 15-49 years on priority to prevent CRS."
- "Most common complication of mumps in children is aseptic meningitis - NOT orchitis - because orchitis only occurs in post-pubertal males."
- "Mumps orchitis causes testicular atrophy in 30-50% but permanent infertility is rare."
- "IgM cannot cross the placenta - so IgM in a newborn confirms CRS regardless of maternal status."
- "Rubella incubation is 14-21 days (avg 18) - NOT less than 10 days - a common wrong answer in MCQs."
Create a printable quick reference cheat sheet for Rubella & Mumps
mkdir -p /home/daytona/workspace/rubella-mumps && echo "ready"
~/rubella-mumps/cheatsheet.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Rubella & Mumps Quick Reference</title>
<style>
@page { size: A4; margin: 10mm; }
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: Arial, Helvetica, sans-serif;
font-size: 8.5px;
color: #1a1a1a;
background: #fff;
padding: 8px;
line-height: 1.35;
}
/* ── TOP BANNER ──────────────────────────────── */
.banner {
background: linear-gradient(135deg, #1a237e 0%, #283593 50%, #3949ab 100%);
color: white;
text-align: center;
padding: 7px 10px 6px;
border-radius: 6px;
margin-bottom: 7px;
}
.banner h1 { font-size: 16px; font-weight: 900; letter-spacing: 1px; margin-bottom: 2px; }
.banner p { font-size: 8px; color: #c5cae9; letter-spacing: 0.5px; }
/* ── TWO-COLUMN LAYOUT ───────────────────────── */
.two-col {
display: grid;
grid-template-columns: 1fr 1fr;
gap: 7px;
margin-bottom: 6px;
}
/* ── CARD ────────────────────────────────────── */
.card {
border-radius: 5px;
overflow: hidden;
border: 1px solid #e0e0e0;
}
.card-header {
padding: 5px 8px;
font-size: 10px;
font-weight: 900;
color: white;
letter-spacing: 0.5px;
}
.card-body { padding: 5px 7px; }
/* rubella palette */
.r-hdr { background: #c62828; }
.r-sub { background: #ef9a9a; color: #b71c1c; font-size: 8px; font-weight: 700; padding: 2px 7px; }
/* mumps palette */
.m-hdr { background: #1565c0; }
.m-sub { background: #90caf9; color: #0d47a1; font-size: 8px; font-weight: 700; padding: 2px 7px; }
.sub-label {
display: block;
font-size: 7.5px;
font-weight: 700;
text-transform: uppercase;
letter-spacing: 0.4px;
margin: 5px 0 2px;
padding-bottom: 1px;
border-bottom: 1px solid #e0e0e0;
}
.r-lbl { color: #c62828; border-color: #ef9a9a; }
.m-lbl { color: #1565c0; border-color: #90caf9; }
.g-lbl { color: #2e7d32; border-color: #a5d6a7; }
.o-lbl { color: #e65100; border-color: #ffcc80; }
/* ── TABLES ──────────────────────────────────── */
table { width: 100%; border-collapse: collapse; margin-bottom: 3px; font-size: 8px; }
thead th {
padding: 3px 4px;
text-align: center;
font-size: 7.5px;
font-weight: 700;
color: white;
border: 0.5px solid rgba(255,255,255,0.3);
}
.r-thead thead th { background: #e53935; }
.m-thead thead th { background: #1e88e5; }
.g-thead thead th { background: #388e3c; }
tbody td {
padding: 2.5px 4px;
border: 0.5px solid #e0e0e0;
vertical-align: top;
}
tbody td:first-child { font-weight: 600; }
tbody tr:nth-child(even) { background: #fafafa; }
/* ── HIGHLIGHT BOXES ────────────────────────── */
.box {
border-radius: 4px;
padding: 5px 7px;
margin-bottom: 4px;
font-size: 8px;
}
.box-red { background: #ffebee; border-left: 3px solid #c62828; }
.box-blue { background: #e3f2fd; border-left: 3px solid #1565c0; }
.box-green { background: #e8f5e9; border-left: 3px solid #2e7d32; }
.box-orange { background: #fff3e0; border-left: 3px solid #e65100; }
.box-purple { background: #f3e5f5; border-left: 3px solid #6a1b9a; }
.box-yellow { background: #fffde7; border-left: 3px solid #f9a825; }
.box b { color: inherit; }
.box .title { font-size: 8.5px; font-weight: 900; margin-bottom: 2px; display: block; }
/* ── BADGE ───────────────────────────────────── */
.badge {
display: inline-block;
padding: 1px 5px;
border-radius: 10px;
font-size: 7px;
font-weight: 700;
margin-left: 4px;
vertical-align: middle;
}
.badge-red { background: #c62828; color: white; }
.badge-blue { background: #1565c0; color: white; }
.badge-green { background: #2e7d32; color: white; }
.badge-orange { background: #e65100; color: white; }
.badge-purple { background: #6a1b9a; color: white; }
/* ── COMPARISON SECTION ─────────────────────── */
.comp-header {
background: linear-gradient(90deg, #c62828, #1565c0);
color: white;
font-size: 10px;
font-weight: 900;
padding: 4px 8px;
border-radius: 5px 5px 0 0;
text-align: center;
letter-spacing: 0.5px;
}
.comp-table { width: 100%; border-collapse: collapse; font-size: 8px; }
.comp-table th {
padding: 3px 5px;
text-align: center;
font-size: 8px;
font-weight: 700;
color: white;
border: 0.5px solid rgba(255,255,255,0.4);
}
.comp-table .th-feat { background: #37474f; }
.comp-table .th-r { background: #c62828; }
.comp-table .th-m { background: #1565c0; }
.comp-table td {
padding: 2.5px 5px;
border: 0.5px solid #e0e0e0;
vertical-align: middle;
}
.comp-table td:first-child { font-weight: 700; background: #f5f5f5; }
.comp-table td:nth-child(2) { background: #fff5f5; }
.comp-table td:nth-child(3) { background: #f0f6ff; }
.comp-table tr:nth-child(even) td:first-child { background: #eeeeee; }
.comp-table tr:nth-child(even) td:nth-child(2) { background: #ffebee; }
.comp-table tr:nth-child(even) td:nth-child(3) { background: #e3f2fd; }
/* ── TIPS SECTION ───────────────────────────── */
.tips-banner {
background: linear-gradient(90deg, #1b5e20, #2e7d32);
color: white;
font-size: 10px;
font-weight: 900;
padding: 4px 8px;
border-radius: 5px 5px 0 0;
letter-spacing: 0.5px;
}
.tips-grid {
display: grid;
grid-template-columns: 1fr 1fr 1fr;
background: #e8f5e9;
border: 1px solid #a5d6a7;
border-top: none;
border-radius: 0 0 5px 5px;
overflow: hidden;
}
.tip-item {
padding: 5px 7px;
border-right: 1px solid #c8e6c9;
font-size: 8px;
line-height: 1.4;
}
.tip-item:last-child { border-right: none; }
.tip-item b { color: #1b5e20; }
/* ── MCQ SECTION ────────────────────────────── */
.mcq-banner {
background: linear-gradient(90deg, #4a148c, #6a1b9a);
color: white;
font-size: 10px;
font-weight: 900;
padding: 4px 8px;
border-radius: 5px 5px 0 0;
letter-spacing: 0.5px;
}
.mcq-grid {
display: grid;
grid-template-columns: 1fr 1fr;
background: #f3e5f5;
border: 1px solid #ce93d8;
border-top: none;
border-radius: 0 0 5px 5px;
overflow: hidden;
gap: 0;
}
.mcq-item {
padding: 4px 7px;
border-right: 1px solid #e1bee7;
border-bottom: 1px solid #e1bee7;
font-size: 8px;
line-height: 1.4;
}
.mcq-item:nth-child(2n) { border-right: none; }
.mcq-q { color: #4a148c; font-weight: 700; }
.mcq-a { color: #c62828; font-weight: 900; }
/* ── FOOTER ──────────────────────────────────── */
.footer {
text-align: center;
font-size: 7px;
color: #9e9e9e;
margin-top: 6px;
padding-top: 4px;
border-top: 0.5px solid #e0e0e0;
}
ul { padding-left: 10px; margin: 0; }
li { margin-bottom: 1.5px; }
</style>
</head>
<body>
<!-- BANNER -->
<div class="banner">
<h1>🦠 RUBELLA & MUMPS — PSM Quick Reference</h1>
<p>MBBS 2nd Year | PSM Practical Exam | Based on Dr. Narendra Kumar Yadav's Slides | Harrison's 22e | ICMR Guidelines</p>
</div>
<!-- ROW 1: RUBELLA + MUMPS BASICS -->
<div class="two-col">
<!-- ── RUBELLA CARD ── -->
<div>
<div class="card">
<div class="card-header r-hdr">🔴 RUBELLA (German Measles / जर्मन दादुरा)</div>
<div class="card-body">
<span class="sub-label r-lbl">BASICS</span>
<table class="r-thead">
<thead><tr><th>Feature</th><th>Detail</th></tr></thead>
<tbody>
<tr><td>Virus</td><td>RNA virus — Togavirus family</td></tr>
<tr><td>Reservoir</td><td>Humans ONLY</td></tr>
<tr><td>Transmission</td><td>Droplet infection</td></tr>
<tr><td>Incubation</td><td><b>14–21 days (avg 18 days)</b> ★ NOT <10 days!</td></tr>
<tr><td>Communicability</td><td>7 days before → 7 days after rash</td></tr>
<tr><td>Age group</td><td>Children 5–15 yrs; adults susceptible</td></tr>
<tr><td>Seasonality</td><td>Late winter – early spring</td></tr>
</tbody>
</table>
<span class="sub-label r-lbl">CLINICAL FEATURES (Post-natal)</span>
<ul>
<li><b>Rash:</b> Maculopapular, face→trunk→limbs, lasts <b>3 days</b> only</li>
<li><b>Lymphadenopathy:</b> Occipital + <b>post-auricular</b> (TENDER) ★ Hallmark!</li>
<li><b>Low-grade fever</b> (or absent); no Koplik spots</li>
<li>Arthralgia/arthritis in adult women (common)</li>
<li><b>50% cases are SUBCLINICAL</b> — no rash, no symptoms!</li>
</ul>
<span class="sub-label r-lbl">WHY CALLED "3-DAY MEASLES"?</span>
<div class="box box-red" style="font-size:8px;">
Rash lasts only <b>3 days</b> (vs measles = 4–7 days). Milder than measles but DANGEROUS in pregnancy!
</div>
<span class="sub-label r-lbl">DIAGNOSIS</span>
<table>
<tbody>
<tr><td>Acquired rubella</td><td><b>IgM antibodies</b> in acute phase OR 4× rise in IgG</td></tr>
<tr><td>CRS at birth</td><td><b>IgM antibodies</b> (IgM does NOT cross placenta → baby made it!)</td></tr>
<tr><td>CRS confirm later</td><td>IgG persists <b>>6 months</b> (maternal IgG disappears by 6 m)</td></tr>
</tbody>
</table>
</div>
</div>
</div>
<!-- ── MUMPS CARD ── -->
<div>
<div class="card">
<div class="card-header m-hdr">🔵 MUMPS (Gulphulia / गुल्फुलिया)</div>
<div class="card-body">
<span class="sub-label m-lbl">BASICS</span>
<table class="m-thead">
<thead><tr><th>Feature</th><th>Detail</th></tr></thead>
<tbody>
<tr><td>Virus</td><td>RNA virus — Paramyxovirus (Rubulavirus genus)</td></tr>
<tr><td>Reservoir</td><td>Humans ONLY</td></tr>
<tr><td>Transmission</td><td>Droplet + direct contact with saliva</td></tr>
<tr><td>Incubation</td><td><b>16–18 days (avg 18 days)</b> ★ MCQ = 18 days!</td></tr>
<tr><td>Communicability</td><td>2 days before → 9 days after parotitis</td></tr>
<tr><td>Age group</td><td>School-age children 5–14 yrs</td></tr>
<tr><td>Immunity</td><td>Lifelong after natural infection</td></tr>
</tbody>
</table>
<span class="sub-label m-lbl">CLINICAL FEATURES</span>
<ul>
<li><b>Parotitis:</b> Painful swelling of parotid gland (in front + below ear)</li>
<li>Usually <b>bilateral</b> (may start unilateral)</li>
<li>Earlobe pushed upward & outward — angle of jaw obliterated</li>
<li>Stensen's duct orifice: red & swollen</li>
<li>Prodrome: fever, malaise, headache, anorexia (1–2 days before)</li>
<li>Swelling lasts ~7–10 days</li>
</ul>
<span class="sub-label m-lbl">MANAGEMENT</span>
<div class="box box-blue" style="font-size:8px;">
<b>NO specific antiviral.</b> Symptomatic only: paracetamol, soft diet, warm/cold compress, rest, hydration. Orchitis: scrotal support + analgesics.
</div>
<span class="sub-label m-lbl">DIAGNOSIS</span>
<table>
<tbody>
<tr><td>Serology</td><td><b>IgM antibodies</b> in acute phase (confirmatory)</td></tr>
<tr><td>Parotitis vs pancreatitis</td><td>Both ↑ amylase; <b>↑ lipase = pancreatitis</b></td></tr>
<tr><td>CSF pleocytosis</td><td>Up to 55% subclinical CNS involvement</td></tr>
</tbody>
</table>
</div>
</div>
</div>
</div><!-- end two-col -->
<!-- ROW 2: CRS + COMPLICATIONS -->
<div class="two-col">
<!-- CRS -->
<div>
<div class="card">
<div class="card-header r-hdr">⭐ CONGENITAL RUBELLA SYNDROME (CRS) — MOST IMPORTANT!</div>
<div class="card-body">
<div class="box box-red">
<span class="title">GREGG'S TRIAD (Classic CRS = "CCC")</span>
<b>C</b>ataract + <b>C</b>ardiac defect (PDA) + <b>C</b>ochlear deafness (sensorineural)
</div>
<span class="sub-label r-lbl">RISK BY TRIMESTER</span>
<table class="r-thead">
<thead><tr><th>Trimester</th><th>Risk of CRS</th><th>Note</th></tr></thead>
<tbody>
<tr><td><b>1st (1–12 wks) ★</b></td><td><b>Up to 90%</b></td><td><b>MOST DISASTROUS!</b></td></tr>
<tr><td>2nd (13–24 wks)</td><td>10–20%</td><td>Moderate risk</td></tr>
<tr><td><b>After 16 wks ★</b></td><td><b>RARE</b></td><td><b>No major defects (MCQ!)</b></td></tr>
</tbody>
</table>
<span class="sub-label r-lbl">CRS DEFECTS</span>
<table>
<tbody>
<tr><td><b>Eyes</b></td><td>Cataract, glaucoma, retinopathy, microphthalmia</td></tr>
<tr><td><b>Heart</b></td><td>PDA, VSD, pulmonary artery stenosis</td></tr>
<tr><td><b>Ears</b></td><td>Sensorineural deafness (most common single defect)</td></tr>
<tr><td><b>Brain</b></td><td>Microcephaly, intellectual disability</td></tr>
<tr><td><b>Transient</b></td><td>Hepatosplenomegaly, thrombocytopenic purpura ("Blueberry muffin baby")</td></tr>
</tbody>
</table>
<div class="box box-orange" style="margin-top:4px;">
<span class="title">IgM vs IgG LOGIC (Exam favourite!)</span>
IgM does <b>NOT</b> cross placenta → <b>IgM in newborn = CRS confirmed</b> (baby made it)<br>
IgG <b>DOES</b> cross placenta → maternal IgG disappears by 6 months → <b>IgG persisting >6 m = CRS</b>
</div>
</div>
</div>
</div>
<!-- MUMPS COMPLICATIONS -->
<div>
<div class="card">
<div class="card-header m-hdr">⚡ MUMPS COMPLICATIONS (Very Frequently Asked!)</div>
<div class="card-body">
<div class="box box-blue">
<span class="title">KEY MCQ RULE:</span>
Most common in <b>CHILDREN</b> = <b>Aseptic Meningitis</b> <span class="badge badge-blue">★ MCQ</span><br>
Most common overall = <b>Orchitis</b> (only in post-pubertal males)
</div>
<span class="sub-label m-lbl">COMPLICATION TABLE</span>
<table class="m-thead">
<thead><tr><th>Complication</th><th>Freq (unvax)</th><th>Key Points</th></tr></thead>
<tbody>
<tr><td><b>Aseptic meningitis ★</b></td><td>Up to 10%</td><td>Most common in children; self-limiting</td></tr>
<tr><td><b>Orchitis ★</b></td><td><b>30%</b> post-pubertal ♂</td><td>30–50% testicular atrophy; rarely permanent infertility</td></tr>
<tr><td>Oophoritis</td><td>7% post-pubertal ♀</td><td>Ovarian inflammation</td></tr>
<tr><td>Pancreatitis</td><td>~4%</td><td>↑ amylase + ↑ lipase</td></tr>
<tr><td>Encephalitis</td><td><1%</td><td>Mortality 1.5%</td></tr>
<tr><td>Hearing loss</td><td>Up to 4%</td><td>Usually unilateral, transient</td></tr>
<tr><td>Mastitis</td><td>30% ♀</td><td>Post-pubertal females</td></tr>
</tbody>
</table>
<span class="sub-label m-lbl">ORCHITIS FACTS (Examiners love this!)</span>
<ul>
<li>Occurs in <b>30% unvaccinated</b> post-pubertal males (6% if vaccinated)</li>
<li>Develops in <b>1st week of parotitis</b> (up to 6 weeks after)</li>
<li>Bilateral in 10–30% of cases</li>
<li>Testicular atrophy in <b>30–50%</b> of affected testes</li>
<li><b>Permanent infertility is RARE</b> despite atrophy</li>
</ul>
</div>
</div>
</div>
</div><!-- end two-col -->
<!-- ROW 3: VACCINE + COMPARISON -->
<div class="two-col">
<!-- VACCINE + PREVENTION -->
<div>
<div class="card">
<div class="card-header" style="background:#2e7d32;">💉 MMR VACCINE & PREVENTION (Both diseases)</div>
<div class="card-body">
<span class="sub-label g-lbl">MMR VACCINE</span>
<table class="g-thead">
<thead><tr><th>Feature</th><th>Detail</th></tr></thead>
<tbody>
<tr><td>Type</td><td><b>Live attenuated</b> (M + M + R combined)</td></tr>
<tr><td>Schedule</td><td><b>9 months + 15 months</b> (Nepal/India)</td></tr>
<tr><td>Route</td><td>Subcutaneous (SC)</td></tr>
<tr><td>Efficacy</td><td>~95% single dose; two-dose reduces mumps by 97–99%</td></tr>
<tr><td>Mumps strain</td><td>Jeryl Lynn strain (genotype A)</td></tr>
<tr><td>Rubella strain</td><td>RA 27/3 strain (grown in human diploid cells)</td></tr>
</tbody>
</table>
<span class="sub-label g-lbl">CONTRAINDICATIONS (Both MMR)</span>
<ul>
<li><b>Pregnancy</b> — delay conception 1 month after MMR!</li>
<li>Severe immunocompromise (HIV with severe immunosuppression)</li>
<li>Severe febrile illness</li>
<li>Note: egg allergy is NOT a contraindication (grown in human cells)</li>
</ul>
<span class="sub-label g-lbl">RUBELLA VACCINATION STRATEGY</span>
<div class="box box-green">
<b>During rubella outbreak → vaccinate NON-PREGNANT WOMEN aged 15–49 years on PRIORITY</b><br>
(Goal = prevent CRS; NOT to protect women themselves)
</div>
<span class="sub-label g-lbl">MUMPS ISOLATION</span>
<div class="box box-blue" style="font-size:8px;">
Isolate for <b>9 days</b> after onset of parotitis. Avoid schools/crowded places during infectious period.
</div>
</div>
</div>
</div>
<!-- MEASLES VS RUBELLA -->
<div>
<div class="card">
<div class="card-header" style="background:#37474f;">⚖️ MEASLES vs RUBELLA (Comparison — Examiners Always Ask!)</div>
<div class="card-body">
<table style="font-size:7.8px;">
<thead>
<tr>
<th style="background:#37474f; color:white; text-align:left; padding:3px 4px;">Feature</th>
<th style="background:#c62828; color:white; padding:3px 4px;">Measles</th>
<th style="background:#e53935; color:white; padding:3px 4px;">Rubella</th>
</tr>
</thead>
<tbody>
<tr><td>Other name</td><td>Hard measles</td><td>German measles / 3-day measles</td></tr>
<tr><td>Virus</td><td>Paramyxovirus (Morbillivirus)</td><td>Togavirus</td></tr>
<tr><td>Incubation</td><td>10–12 days</td><td><b>14–21 days (avg 18)</b></td></tr>
<tr><td>Rash duration</td><td><b>4–7 days</b></td><td><b>3 days only</b></td></tr>
<tr><td>Koplik spots</td><td><b>Present ★</b></td><td><b>ABSENT</b></td></tr>
<tr><td>LN enlarged</td><td>Cervical</td><td><b>Occipital + post-auricular</b></td></tr>
<tr><td>Fever</td><td>High (3C's prodrome)</td><td>Low grade / absent</td></tr>
<tr><td>Severity</td><td><b>More severe</b></td><td>Milder</td></tr>
<tr><td>3C's prodrome</td><td><b>Yes</b> (Cough, Coryza, Conjunctivitis)</td><td>No</td></tr>
<tr><td>Subclinical cases</td><td>Rare</td><td><b>50%!</b></td></tr>
<tr><td>Danger in pregnancy</td><td>Less</td><td><b>EXTREMELY DANGEROUS → CRS</b></td></tr>
<tr><td>Arthritis in adults</td><td>Rare</td><td><b>Common (esp. women)</b></td></tr>
<tr><td>Vaccine</td><td colspan="2" style="text-align:center;"><b>Both in MMR (live attenuated)</b></td></tr>
</tbody>
</table>
</div>
</div>
</div>
</div><!-- end two-col -->
<!-- MCQ BANK -->
<div style="margin-bottom:6px;">
<div class="mcq-banner">📝 MCQ ANSWERS (Directly from Your Slides)</div>
<div class="mcq-grid">
<div class="mcq-item">
<span class="mcq-q">Q. Vaccination priority in rubella outbreak?</span><br>
<span class="mcq-a">✔ Women 15–49 years (NON-PREGNANT)</span>
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Max fetal damage from maternal rubella?</span><br>
<span class="mcq-a">✔ 6–12 weeks (1st trimester)</span>
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Rubella incubation period?</span><br>
<span class="mcq-a">✔ 14–21 days avg 18 days (NOT <10 days!)</span>
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Rubella infection after 16 weeks?</span><br>
<span class="mcq-a">✔ No major congenital abnormalities</span>
</div>
<div class="mcq-item">
<span class="mcq-q">Q. How to diagnose CRS at birth?</span><br>
<span class="mcq-a">✔ IgM at birth OR IgG persisting >6 months</span>
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Rubella caused by which type of virus?</span><br>
<span class="mcq-a">✔ RNA virus (Togavirus) — NOT DNA!</span>
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Most common mumps complication in CHILDREN?</span><br>
<span class="mcq-a">✔ Aseptic meningitis (NOT orchitis!)</span>
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Incubation period of mumps?</span><br>
<span class="mcq-a">✔ 18 days (range 12–25 days)</span>
</div>
</div>
</div>
<!-- EXAM TIPS -->
<div style="margin-bottom:5px;">
<div class="tips-banner">🌟 IMPRESS THE EXAMINER — SAY THESE LINES!</div>
<div class="tips-grid">
<div class="tip-item">
✔ <b>"50% of rubella cases are subclinical — this is why pregnant women don't know they're infected, making CRS prevention so critical."</b>
</div>
<div class="tip-item">
✔ <b>"IgM cannot cross the placenta — so IgM in a newborn confirms CRS regardless of the mother's history."</b>
</div>
<div class="tip-item">
✔ <b>"Gregg's triad = Cataract + Cardiac defect (PDA) + Cochlear deafness — the three C's of CRS."</b>
</div>
<div class="tip-item">
✔ <b>"During a rubella outbreak, we vaccinate non-pregnant women 15–49 years NOT to protect them, but to prevent CRS in future pregnancies."</b>
</div>
<div class="tip-item">
✔ <b>"Most common mumps complication in CHILDREN is aseptic meningitis — orchitis only occurs in post-pubertal males, so it cannot be the answer for children."</b>
</div>
<div class="tip-item">
✔ <b>"Mumps orchitis causes testicular atrophy in 30–50% but permanent infertility is rare — so patients should be reassured."</b>
</div>
</div>
</div>
<!-- FOOTER -->
<div class="footer">
PSM Practical Quick Reference | MBBS 2nd Year |
Based on: Dr. Narendra Kumar Yadav's Slides + Harrison's Principles of Internal Medicine 22e + ICMR Guidelines |
Generated by Orris — Good luck on your exam! 🎓
</div>
</body>
</html>
libreoffice --headless --convert-to pdf --outdir /tmp/ /home/daytona/workspace/rubella-mumps/cheatsheet.html 2>&1 && ls -lh /tmp/cheatsheet.pdf && cp /tmp/cheatsheet.pdf /home/daytona/workspace/rubella-mumps/Rubella_Mumps_Cheatsheet.pdf
python3 -c " from pypdf import PdfReader r = PdfReader('/home/daytona/workspace/rubella-mumps/Rubella_Mumps_Cheatsheet.pdf') print(f'Pages: {len(r.pages)}') print('First 200 chars:', r.pages[0].extract_text()[:200]) "
Rubella Mumps Cheatsheet
PDF Document · PDF
cheatsheet
HTML File · HTML
| Section | What's inside |
|---|---|
| 🔴 Rubella basics | Virus, incubation, transmission, clinical features, diagnosis |
| 🔵 Mumps basics | Virus, parotitis features, management, diagnosis |
| ⭐ CRS section | Gregg's triad, risk by trimester, all defects, IgM vs IgG logic |
| ⚡ Mumps complications | Full table with %, orchitis facts, the children vs adult MCQ rule |
| 💉 MMR vaccine | Schedule, strains, contraindications, rubella outbreak strategy |
| ⚖️ Measles vs Rubella | Full comparison table - 13 features |
| 📝 MCQ bank | All 8 MCQs directly from your teacher's slides with answers |
| 🌟 Exam tips | 6 impressive lines to say to the external examiner |
Tomorrow is my psm practical exam of mbbs 2nd year from nepal. I dont know about chickenpox and smallpox . External maam surely ask me this topic . Could you please provide me about chicken pox and small pox from k park psm in easy language so that i will never forget it . And the external will impress
mkdir -p /home/daytona/workspace/chickenpox-smallpox && echo "ready"
~/chickenpox-smallpox/cheatsheet.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Chickenpox & Smallpox Quick Reference</title>
<style>
@page { size: A4; margin: 9mm; }
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: Arial, Helvetica, sans-serif;
font-size: 8.2px;
color: #1a1a1a;
background: #fff;
padding: 7px;
line-height: 1.35;
}
.banner {
background: linear-gradient(135deg, #1a237e 0%, #283593 50%, #3949ab 100%);
color: white;
text-align: center;
padding: 7px 10px 6px;
border-radius: 6px;
margin-bottom: 7px;
}
.banner h1 { font-size: 15px; font-weight: 900; letter-spacing: 0.8px; margin-bottom: 2px; }
.banner p { font-size: 7.5px; color: #c5cae9; }
.two-col { display: grid; grid-template-columns: 1fr 1fr; gap: 6px; margin-bottom: 6px; }
.three-col { display: grid; grid-template-columns: 1fr 1fr 1fr; gap: 6px; margin-bottom: 6px; }
.card { border-radius: 5px; overflow: hidden; border: 1px solid #e0e0e0; }
.card-header { padding: 5px 8px; font-size: 10px; font-weight: 900; color: white; }
.card-body { padding: 5px 7px; }
/* chickenpox = warm orange */
.cp-hdr { background: #e65100; }
.cp-lbl { color: #bf360c; border-color: #ffcc80; }
.cp-thead thead th { background: #f4511e; }
.cp-box { background: #fff3e0; border-left: 3px solid #e65100; }
/* smallpox = dark maroon */
.sp-hdr { background: #4a148c; }
.sp-lbl { color: #4a148c; border-color: #ce93d8; }
.sp-thead thead th { background: #6a1b9a; }
.sp-box { background: #f3e5f5; border-left: 3px solid #6a1b9a; }
/* green = shared/comparison */
.g-hdr { background: #1b5e20; }
.g-lbl { color: #1b5e20; border-color: #a5d6a7; }
.g-thead thead th { background: #2e7d32; }
.sub-label {
display: block; font-size: 7.5px; font-weight: 700;
text-transform: uppercase; letter-spacing: 0.4px;
margin: 4px 0 2px; padding-bottom: 1px; border-bottom: 1px solid #e0e0e0;
}
table { width: 100%; border-collapse: collapse; margin-bottom: 3px; font-size: 8px; }
thead th { padding: 3px 4px; text-align: center; font-size: 7.5px; font-weight: 700; color: white; border: 0.5px solid rgba(255,255,255,0.3); }
tbody td { padding: 2.5px 4px; border: 0.5px solid #e0e0e0; vertical-align: top; }
tbody td:first-child { font-weight: 600; }
tbody tr:nth-child(even) { background: #fafafa; }
.box { border-radius: 4px; padding: 4px 7px; margin-bottom: 3px; font-size: 8px; }
.box-red { background: #ffebee; border-left: 3px solid #c62828; }
.box-orange { background: #fff3e0; border-left: 3px solid #e65100; }
.box-purple { background: #f3e5f5; border-left: 3px solid #6a1b9a; }
.box-green { background: #e8f5e9; border-left: 3px solid #2e7d32; }
.box-blue { background: #e3f2fd; border-left: 3px solid #1565c0; }
.box-yellow { background: #fffde7; border-left: 3px solid #f9a825; }
.box .title { font-size: 8.5px; font-weight: 900; display: block; margin-bottom: 2px; }
ul { padding-left: 10px; margin: 0; }
li { margin-bottom: 1.5px; }
/* COMPARISON TABLE */
.comp-wrap { margin-bottom: 6px; }
.comp-banner { background: linear-gradient(90deg, #e65100, #4a148c); color: white; font-size: 10px; font-weight: 900; padding: 4px 8px; border-radius: 5px 5px 0 0; text-align: center; letter-spacing: 0.5px; }
.comp-table { width: 100%; border-collapse: collapse; font-size: 7.8px; }
.comp-table th { padding: 3px 5px; text-align: center; font-weight: 700; color: white; border: 0.5px solid rgba(255,255,255,0.3); }
.comp-table .th-f { background: #37474f; text-align: left; }
.comp-table .th-cp { background: #e65100; }
.comp-table .th-sp { background: #6a1b9a; }
.comp-table td { padding: 2.5px 5px; border: 0.5px solid #e0e0e0; vertical-align: top; }
.comp-table td:first-child { font-weight: 700; background: #f5f5f5; }
.comp-table td:nth-child(2) { background: #fff8f2; }
.comp-table td:nth-child(3) { background: #faf4ff; }
.comp-table tr:nth-child(even) td:first-child { background: #eeeeee; }
.comp-table tr:nth-child(even) td:nth-child(2) { background: #fff3e0; }
.comp-table tr:nth-child(even) td:nth-child(3) { background: #f3e5f5; }
/* MCQ */
.mcq-banner { background: linear-gradient(90deg, #1565c0, #0d47a1); color: white; font-size: 9.5px; font-weight: 900; padding: 4px 8px; border-radius: 5px 5px 0 0; letter-spacing: 0.5px; }
.mcq-grid { display: grid; grid-template-columns: 1fr 1fr 1fr; background: #e3f2fd; border: 1px solid #90caf9; border-top: none; border-radius: 0 0 5px 5px; }
.mcq-item { padding: 4px 7px; border-right: 1px solid #bbdefb; border-bottom: 1px solid #bbdefb; font-size: 7.8px; line-height: 1.4; }
.mcq-q { color: #0d47a1; font-weight: 700; }
.mcq-a { color: #b71c1c; font-weight: 900; }
/* TIPS */
.tips-banner { background: linear-gradient(90deg, #1b5e20, #2e7d32); color: white; font-size: 9.5px; font-weight: 900; padding: 4px 8px; border-radius: 5px 5px 0 0; letter-spacing: 0.5px; }
.tips-grid { display: grid; grid-template-columns: 1fr 1fr 1fr; background: #e8f5e9; border: 1px solid #a5d6a7; border-top: none; border-radius: 0 0 5px 5px; }
.tip-item { padding: 4px 7px; border-right: 1px solid #c8e6c9; font-size: 7.8px; line-height: 1.5; }
.tip-item:last-child { border-right: none; }
.tip-item b { color: #1b5e20; }
.footer { text-align: center; font-size: 6.8px; color: #9e9e9e; margin-top: 5px; padding-top: 3px; border-top: 0.5px solid #e0e0e0; }
.badge { display: inline-block; padding: 1px 5px; border-radius: 10px; font-size: 7px; font-weight: 700; margin-left: 3px; }
.badge-red { background: #c62828; color: white; }
.badge-orange { background: #e65100; color: white; }
.badge-purple { background: #6a1b9a; color: white; }
.badge-green { background: #2e7d32; color: white; }
</style>
</head>
<body>
<!-- BANNER -->
<div class="banner">
<h1>🐔 CHICKENPOX & SMALLPOX — PSM Quick Reference (K. Park)</h1>
<p>MBBS 2nd Year | PSM Practical Exam | Park's Textbook of PSM | Red Book 2021 | Harrison's 22e</p>
</div>
<!-- ROW 1: CHICKENPOX + SMALLPOX BASICS -->
<div class="two-col">
<!-- CHICKENPOX -->
<div class="card">
<div class="card-header cp-hdr">🐔 CHICKENPOX (Varicella)</div>
<div class="card-body">
<span class="sub-label cp-lbl">BASICS</span>
<table class="cp-thead">
<thead><tr><th>Feature</th><th>Detail</th></tr></thead>
<tbody>
<tr><td>Causative agent</td><td><b>Varicella-Zoster Virus (VZV)</b> — also called Human (alpha) Herpesvirus 3</td></tr>
<tr><td>Type</td><td>DNA virus (Herpesvirus family)</td></tr>
<tr><td>Reservoir</td><td>Humans only</td></tr>
<tr><td>Source</td><td>Cases of chickenpox; rarely herpes zoster patients</td></tr>
<tr><td>Transmission</td><td>Droplet + <b>direct contact</b> with lesions + <b>airborne</b> (most contagious)</td></tr>
<tr><td>Incubation</td><td><b>15 days (range: 7–21 days)</b></td></tr>
<tr><td>Communicability</td><td><b>1–2 days before rash → 4–5 days after rash</b> (until lesions crust)</td></tr>
<tr><td>Secondary attack rate</td><td><b>~85%</b> in susceptible household contacts</td></tr>
<tr><td>Immunity</td><td>One attack = <b>lifelong immunity</b>; second attacks rare</td></tr>
<tr><td>Infectivity of scabs</td><td><b>Scabs are NOT infective</b> ★</td></tr>
</tbody>
</table>
<span class="sub-label cp-lbl">CLINICAL FEATURES</span>
<div class="box cp-box">
<span class="title">PRODROMAL STAGE (1–2 days before rash)</span>
Mild fever, malaise. Children often have NO prodrome — rash is the 1st sign.
</div>
<div class="box cp-box">
<span class="title">ERUPTIVE STAGE — 4 KEY FEATURES</span>
<b>(1) Distribution (CENTRIPETAL):</b> Trunk first (abundant) → face, arms, legs (less). Axilla affected. <b>Palms & soles usually SPARED.</b> Mucous membranes involved.<br>
<b>(2) Rapid evolution:</b> Macule → Papule → Vesicle ("dew-drop on skin") → Scab in 4–7 days. Vesicles are <b>superficial, unilocular, easily ruptured</b>. Area of inflammation around vesicles.<br>
<b>(3) PLEOMORPHISM ★:</b> All stages (papules, vesicles, crusts) present simultaneously in same area — because rash comes in successive crops over 4–5 days.<br>
<b>(4) Fever:</b> Low-grade; rises with each new crop of rash.
</div>
<span class="sub-label cp-lbl">COMPLICATIONS</span>
<ul>
<li><b>Secondary bacterial infection</b> (Group A Strep, Staph aureus) — most common</li>
<li>Cellulitis, erysipelas, osteomyelitis</li>
<li><b>Pneumonia</b> (adults especially)</li>
<li><b>Encephalitis / Cerebellar ataxia</b> (neurological)</li>
<li><b>Reye's syndrome</b> (if aspirin given to children!)</li>
<li><b>Herpes Zoster</b> — virus stays latent in dorsal root ganglia; reactivates later</li>
<li>Immunocompromised: disseminated disease, DIC (rapidly fatal)</li>
<li>Pitted scars (frequent sequelae)</li>
</ul>
</div>
</div>
<!-- SMALLPOX -->
<div class="card">
<div class="card-header sp-hdr">☠️ SMALLPOX (Variola) — ERADICATED!</div>
<div class="card-body">
<span class="sub-label sp-lbl">BASICS</span>
<table class="sp-thead">
<thead><tr><th>Feature</th><th>Detail</th></tr></thead>
<tbody>
<tr><td>Causative agent</td><td><b>Variola virus</b> (DNA virus, Poxvirus family — Orthopoxvirus)</td></tr>
<tr><td>Types</td><td><b>Variola major</b> (CFR ~30%) and <b>Variola minor</b> (CFR ~1%)</td></tr>
<tr><td>Reservoir</td><td><b>Humans only</b> (no animal reservoir — key for eradication)</td></tr>
<tr><td>Transmission</td><td>Droplet + direct contact; scabs also infective (unlike chickenpox)</td></tr>
<tr><td>Incubation</td><td><b>12 days (range: 7–17 days)</b></td></tr>
<tr><td>Communicability</td><td>From onset of oral lesions until all crusts fall off (~3–4 weeks)</td></tr>
<tr><td>Status</td><td><b>GLOBALLY ERADICATED — 1980 (WHO confirmed)</b></td></tr>
</tbody>
</table>
<span class="sub-label sp-lbl">CLINICAL FEATURES</span>
<div class="box sp-box">
<span class="title">PRODROMAL STAGE (2–4 days) — SEVERE</span>
High fever (38.9–40°C), severe headache, <b>backache</b> (characteristic!), malaise, prostration. Children: vomiting, seizures. Patient is <b>bedridden</b>.
</div>
<div class="box sp-box">
<span class="title">ERUPTIVE STAGE — KEY FEATURES</span>
<b>(1) Distribution (CENTRIFUGAL):</b> Face first → forearms → trunk → legs. <b>Palms & soles involved. Axilla usually free.</b><br>
<b>(2) Slow, deliberate, "majestic" evolution:</b> Macule → Papule → Vesicle → Pustule → Scab. Each stage 1–2 days. Scabs form in 10–14 days.<br>
<b>(3) MONOMORPHISM ★:</b> All lesions at same stage in same area at same time.<br>
<b>(4) Vesicles deep-seated, multilocular, umbilicated, hard ("pearls of pus").</b> No area of inflammation around lesions.<br>
<b>(5) Fever:</b> Falls with rash; may rise again in pustular stage (secondary rise).
</div>
<span class="sub-label sp-lbl">ERADICATION STORY (Park's) ★ Impress!</span>
<ul>
<li>WHO campaign began <b>1967</b> (surveillance & containment strategy)</li>
<li>Last case in <b>India: 24 May 1975</b>; India declared free: <b>5 July 1975</b></li>
<li>Last natural case worldwide: <b>Somalia, 1977</b></li>
<li>WHO declared global eradication: <b>May 1980</b></li>
<li>Virus still kept in 2 labs: <b>USA (CDC Atlanta)</b> & <b>Russia (Novosibirsk)</b></li>
<li>Bioterrorism concern: vaccination restarted for military (2002) & first responders (2003)</li>
</ul>
</div>
</div>
</div><!-- end two-col -->
<!-- ROW 2: TREATMENT/VACCINE + HERPES ZOSTER -->
<div class="two-col">
<!-- CHICKENPOX TREATMENT + VACCINE -->
<div class="card">
<div class="card-header" style="background:#bf360c;">💊 TREATMENT & PREVENTION — CHICKENPOX</div>
<div class="card-body">
<span class="sub-label cp-lbl">TREATMENT</span>
<div class="box box-orange">
<b>Antiviral of choice: ACYCLOVIR</b> (also valacyclovir, famciclovir, foscarnet)<br>
Used in: immunocompromised, adults, severe disease, pneumonia.<br>
Prevents disseminated disease in immunosuppressed patients.
</div>
<div class="box box-red">
<b>⚠️ ASPIRIN (Salicylates) CONTRAINDICATED</b> in children with chickenpox!<br>
Risk of <b>Reye's syndrome</b> (hepatic encephalopathy). Avoid salicylates for 6 weeks post-vaccination too.
</div>
<span class="sub-label cp-lbl">VARICELLA VACCINE (Active Immunization)</span>
<table>
<tbody>
<tr><td>Type</td><td><b>Live attenuated</b> varicella vaccine (Oka strain)</td></tr>
<tr><td>Schedule</td><td>2 doses: <b>12–15 months + 4–6 years</b></td></tr>
<tr><td>Route</td><td>Subcutaneous (SC)</td></tr>
<tr><td>Efficacy</td><td>~85–90% against disease; ~100% against severe disease</td></tr>
<tr><td>Contraindications</td><td>Pregnancy (delay 4 weeks post-vaccine), severe immunocompromise</td></tr>
<tr><td>Post-exposure use</td><td>Within <b>5 days</b> of exposure; >90% efficacy if within 3 days</td></tr>
</tbody>
</table>
<span class="sub-label cp-lbl">VZIG (Passive Immunization)</span>
<div class="box box-blue" style="font-size:8px;">
<b>Varicella-Zoster Immunoglobulin (VZIG)</b> — given within <b>72 hours</b> of exposure.<br>
For: pregnant women, immunocompromised, neonates exposed perinatally, premature infants.
</div>
<span class="sub-label cp-lbl">CONTROL MEASURES</span>
<ul>
<li>Notification to health authorities</li>
<li><b>Isolation</b> for 6 days after onset of rash</li>
<li>Disinfection of articles soiled by secretions</li>
<li>PCR of vesicular fluid for laboratory confirmation</li>
</ul>
</div>
</div>
<!-- HERPES ZOSTER + SMALLPOX VACCINE -->
<div class="card">
<div class="card-header" style="background:#37474f;">🔥 HERPES ZOSTER + SMALLPOX VACCINE</div>
<div class="card-body">
<span class="sub-label" style="color:#37474f; border-color:#90a4ae;">HERPES ZOSTER (Shingles) — Same VZV Virus!</span>
<div class="box box-yellow">
<span class="title">The VZV Link: Chickenpox → Herpes Zoster</span>
After chickenpox, VZV stays <b>LATENT</b> in cranial nerve sensory ganglia & dorsal root ganglia. When cell-mediated immunity <b>wanes</b> (old age, steroids, HIV) → virus reactivates → <b>Herpes Zoster</b>.
</div>
<ul>
<li>Affects ~10–30% of chickenpox survivors</li>
<li>Risk increases sharply after <b>50 years</b></li>
<li>~50% of people reaching age 85 will have had at least 1 zoster episode</li>
<li>Painful vesicular eruption along <b>1 dermatome</b> distribution</li>
<li>Complication: <b>Post-herpetic neuralgia</b> (acyclovir does NOT prevent this!)</li>
<li>Contact with zoster rash → <b>VARICELLA</b> (not zoster) in susceptible person</li>
<li>Zoster is ~20% as infectious as chickenpox</li>
</ul>
<span class="sub-label sp-lbl" style="margin-top:5px;">SMALLPOX VACCINE (Vaccinia Virus)</span>
<table>
<tbody>
<tr><td>Type</td><td><b>Live vaccinia virus</b> (not variola — a related poxvirus)</td></tr>
<tr><td>Route</td><td>Intradermal — <b>bifurcated needle</b> technique</td></tr>
<tr><td>Efficacy</td><td>~95%; protects against variola major & minor</td></tr>
<tr><td>Immunity duration</td><td>3–5 years (wanes; no routine boosters now)</td></tr>
<tr><td>Status now</td><td><b>Routine vaccination DISCONTINUED worldwide after 1980</b></td></tr>
<tr><td>Stockpiles</td><td>WHO maintains reserve for >200 million people</td></tr>
<tr><td>Strategy used</td><td><b>Ring vaccination / Surveillance & Containment</b> (not mass vaccination)</td></tr>
</tbody>
</table>
<div class="box box-purple" style="margin-top:4px;font-size:7.8px;">
<b>Why was smallpox eradicated (but not polio/measles yet)?</b><br>
✔ No animal reservoir ✔ No subclinical infectious cases ✔ Effective vaccine available ✔ Visible rash (easy to identify cases) ✔ Single stable serotype
</div>
</div>
</div>
</div><!-- end two-col -->
<!-- BIG COMPARISON TABLE -->
<div class="comp-wrap">
<div class="comp-banner">⚖️ CHICKENPOX vs SMALLPOX — PARK'S COMPARISON TABLE (Most Frequently Asked!)</div>
<table class="comp-table">
<thead>
<tr>
<th class="th-f">Feature</th>
<th class="th-cp">🐔 CHICKENPOX (Varicella)</th>
<th class="th-sp">☠️ SMALLPOX (Variola)</th>
</tr>
</thead>
<tbody>
<tr><td>Causative agent</td><td>VZV (Herpesvirus) — DNA virus</td><td>Variola virus (Poxvirus) — DNA virus</td></tr>
<tr><td>Incubation period</td><td><b>15 days (7–21 days)</b></td><td><b>12 days (7–17 days)</b></td></tr>
<tr><td>Prodromal symptoms</td><td><b>Usually mild</b> (often no prodrome in children)</td><td><b>Severe</b> — high fever, backache, prostration, bedridden</td></tr>
<tr><td>Distribution of rash</td><td><b>CENTRIPETAL</b> — trunk first, then limbs</td><td><b>CENTRIFUGAL</b> — face first, then trunk, limbs</td></tr>
<tr><td>Palms & soles</td><td><b>Seldom affected</b></td><td><b>Frequently involved</b> ★</td></tr>
<tr><td>Axilla</td><td><b>Affected</b></td><td><b>Usually FREE</b></td></tr>
<tr><td>Rash surface</td><td>Mostly <b>flexor surfaces</b></td><td>Mostly <b>extensor surfaces and bony prominences</b></td></tr>
<tr><td>Vesicle character</td><td><b>Superficial, unilocular</b>, dew-drop appearance, easily ruptured, area of inflammation around</td><td><b>Deep-seated, multilocular, umbilicated</b>, "pearls of pus", NO area of inflammation around</td></tr>
<tr><td>Rash stages</td><td><b>PLEOMORPHIC</b> — all stages simultaneously (crops)</td><td><b>MONOMORPHIC</b> — all lesions at same stage</td></tr>
<tr><td>Evolution of rash</td><td><b>Very rapid</b></td><td><b>Slow, deliberate, "majestic"</b></td></tr>
<tr><td>Scabbing begins</td><td><b>4–7 days</b> after rash</td><td><b>10–14 days</b> after rash</td></tr>
<tr><td>Fever pattern</td><td>Rises with each <b>new crop</b> of rash</td><td>Falls with rash; <b>secondary rise in pustular stage</b></td></tr>
<tr><td>Infectivity of scabs</td><td><b>Scabs NOT infective</b> ★</td><td><b>Scabs ARE infective</b></td></tr>
<tr><td>Scarring</td><td>Less (pitted scars if scratched)</td><td><b>Severe scarring</b></td></tr>
<tr><td>Case fatality rate</td><td><b>~3 per 100,000</b> (very low)</td><td>Variola major: <b>~30%</b>; Minor: ~1%</td></tr>
<tr><td>Treatment</td><td><b>Acyclovir</b> (symptomatic + antiviral)</td><td><b>No specific treatment</b> (supportive only)</td></tr>
<tr><td>Vaccine</td><td>Live attenuated <b>varicella (Oka strain)</b></td><td>Live <b>vaccinia virus</b> — discontinued after eradication</td></tr>
<tr><td>Current status</td><td>Still occurring worldwide</td><td><b>GLOBALLY ERADICATED (1980)</b></td></tr>
</tbody>
</table>
</div>
<!-- MCQ BANK -->
<div style="margin-bottom:5px;">
<div class="mcq-banner">📝 EXPECTED MCQs & VIVA QUESTIONS WITH ANSWERS</div>
<div class="mcq-grid">
<div class="mcq-item">
<span class="mcq-q">Q. Rash in chickenpox is?</span><br>
<span class="mcq-a">✔ PLEOMORPHIC (all stages at once)</span><br>
Rash in smallpox = MONOMORPHIC
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Distribution of rash in chickenpox?</span><br>
<span class="mcq-a">✔ CENTRIPETAL (trunk first)</span><br>
Smallpox = CENTRIFUGAL (face first)
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Global eradication of smallpox confirmed by?</span><br>
<span class="mcq-a">✔ WHO, May 1980</span><br>
Last natural case: Somalia 1977
</div>
<div class="mcq-item">
<span class="mcq-q">Q. India declared smallpox-free when?</span><br>
<span class="mcq-a">✔ 5th July 1975</span><br>
Last case in India: 24 May 1975
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Scabs in chickenpox are infective? True/False?</span><br>
<span class="mcq-a">✔ FALSE — scabs are NOT infective</span><br>
But smallpox scabs ARE infective!
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Secondary attack rate of varicella?</span><br>
<span class="mcq-a">✔ ~85% in household contacts</span><br>
Highly contagious disease
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Drug CONTRAINDICATED in childhood chickenpox?</span><br>
<span class="mcq-a">✔ ASPIRIN (causes Reye's syndrome)</span><br>
Use paracetamol instead!
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Eradication strategy used for smallpox?</span><br>
<span class="mcq-a">✔ Surveillance & Containment (Ring vaccination)</span><br>
NOT mass vaccination!
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Where is smallpox virus still stored?</span><br>
<span class="mcq-a">✔ CDC (USA) & VECTOR Institute (Russia)</span><br>
Only 2 labs in world
</div>
</div>
</div>
<!-- EXAM TIPS -->
<div style="margin-bottom:5px;">
<div class="tips-banner">🌟 IMPRESS THE EXAMINER — SAY THESE EXACT LINES!</div>
<div class="tips-grid">
<div class="tip-item">
✔ <b>"Chickenpox rash is pleomorphic — all stages seen simultaneously because it appears in successive crops. Smallpox is monomorphic — all lesions at the same stage."</b>
</div>
<div class="tip-item">
✔ <b>"Chickenpox scabs are not infective — the virus dies out before the pustular stage. But smallpox scabs ARE infective until they fall off."</b>
</div>
<div class="tip-item">
✔ <b>"Aspirin must never be given to children with chickenpox because it causes Reye's syndrome — a potentially fatal hepatic encephalopathy."</b>
</div>
<div class="tip-item">
✔ <b>"Smallpox was eradicated because it had no animal reservoir, no subclinical infectious cases, a visible rash for easy detection, and an effective vaccine — unique combination."</b>
</div>
<div class="tip-item">
✔ <b>"After chickenpox, VZV lies latent in dorsal root ganglia for decades. When cell-mediated immunity wanes — with age or immunosuppression — it reactivates as Herpes Zoster."</b>
</div>
<div class="tip-item">
✔ <b>"India was declared smallpox-free on 5th July 1975. WHO confirmed global eradication in May 1980 — the first and only human disease to be eradicated."</b>
</div>
</div>
</div>
<div class="footer">
PSM Quick Reference | MBBS 2nd Year | Source: Park's Textbook of Preventive & Social Medicine | Red Book 2021 | Harrison's 22e | Generated by Orris — Good luck! 🎓
</div>
</body>
</html>
libreoffice --headless --convert-to pdf --outdir /tmp/ /home/daytona/workspace/chickenpox-smallpox/cheatsheet.html 2>&1 && ls -lh /tmp/cheatsheet.pdf && cp /tmp/cheatsheet.pdf /home/daytona/workspace/chickenpox-smallpox/Chickenpox_Smallpox_Cheatsheet.pdf && python3 -c "from pypdf import PdfReader; r=PdfReader('/home/daytona/workspace/chickenpox-smallpox/Chickenpox_Smallpox_Cheatsheet.pdf'); print(f'Pages: {len(r.pages)}')"
CHICKENPOX & MUMPS — Complete PSM Guide (K. Park)
PART 1: CHICKENPOX (Varicella)
1. One-Line Definition (Park's)
Chickenpox is an acute, highly infectious disease caused by Varicella-Zoster Virus (VZV), also called Human (alpha) Herpesvirus 3, characterized by a vesicular rash with fever and malaise.
2. Epidemiological Determinants
| Feature | Detail |
|---|---|
| Agent | VZV — Human (alpha) Herpesvirus 3, DNA virus |
| Source | Cases of chickenpox; rarely herpes zoster patients |
| Virus in | Oropharyngeal secretions + lesions of skin and mucosa |
| Scabs | Scabs are NOT infective (virus dies before pustular stage) |
- Droplet infection + direct contact with lesions + airborne (highly contagious)
- Most common under 10 years of age
- One attack = lifelong immunity (second attacks rare)
- Maternal antibody protects infants in first few months
- Adults get more severe disease
3. Clinical Features (Park's exact description)
- Mild fever, malaise
- In children: often no prodrome — rash is the FIRST sign
- Trunk first (abundant) → face, arms, legs (less abundant)
- Axilla affected
- Palms and soles usually NOT affected
- Mucosal surfaces (buccal, pharyngeal) involved
- Macule → Papule → Vesicle → Scab in just 4–7 days
- Vesicles = "dew-drops on skin" — superficial, unilocular, easily ruptured
- Area of inflammation around vesicles (erythematous halo)
- Many lesions abort; some go directly to crust without pustule
- All stages — papules, vesicles, crusts — present simultaneously in the same area
- Because rash appears in successive crops over 4–5 days
- Low-grade; rises with each new crop of rash
4. Complications
| Complication | Notes |
|---|---|
| Secondary bacterial infection | Most common; Group A Strep, Staph aureus |
| Cellulitis, erysipelas, osteomyelitis | Bacterial complications |
| Pneumonia | Especially in adults |
| Encephalitis / Cerebellar ataxia | Neurological |
| Reye's syndrome | If aspirin given — NEVER give aspirin! |
| Herpes Zoster | Latent virus reactivates later in life |
| Disseminated disease, DIC | In immunocompromised (rapidly fatal) |
| Pitted scars | Frequent sequelae |
5. Treatment & Prevention (Park's)
- Acyclovir (drug of choice) — also valacyclovir, famciclovir, foscarnet
- Prevents disseminated disease in immunosuppressed patients
- Acyclovir does NOT prevent post-herpetic neuralgia
- Live attenuated — Oka strain
- 2 doses: 12–15 months + 4–6 years
- Subcutaneous route
- Post-exposure: within 5 days of exposure (>90% efficacy if within 3 days)
- Contraindicated in pregnancy (delay 4 weeks)
- Varicella-Zoster Immunoglobulin within 72 hours of exposure
- For pregnant women, immunocompromised, perinatally exposed neonates
- Notification + Isolation for 6 days after onset of rash
- Disinfect articles soiled by secretions
PART 2: SMALLPOX (Variola)
1. One-Line Definition (Park's)
Smallpox is an acute infectious disease caused by Variola virus, characterized by sudden fever, headache, backache, vomiting, and on the 3rd day a typical rash appearing in a centrifugal distribution passing through macule → papule → vesicle → pustule → scab with subsequent scarring.
2. Epidemiology
| Feature | Detail |
|---|---|
| Agent | Variola virus — DNA virus, Poxvirus family (Orthopoxvirus) |
| Types | Variola major (CFR ~30%) and Variola minor (CFR ~1%) |
| Reservoir | Humans only — NO animal reservoir |
| Transmission | Droplet + direct contact; scabs are infective |
| Incubation | 12 days (range: 7–17 days) |
| CFR | Variola major: ~30% (highest in pregnant women, infants, elderly) |
3. Clinical Features
- High fever (38.9–40°C)
- Severe headache and BACKACHE (characteristic of smallpox!)
- Malaise, severe prostration — patient is bedridden
- Children: vomiting, convulsions
- Face first → forearms → trunk → legs
- Palms and soles frequently involved
- Axilla usually free
- Rash dense on extensor surfaces and bony prominences
- Macule → Papule → Vesicle → Pustule → Scab
- Each stage lasts 1–2 days
- Scabs form 10–14 days after rash
- NO area of inflammation around lesions
- Ordinary (90% of cases)
- Hemorrhagic (~5%) — CFR ~100%
- Malignant/flat (~5%) — CFR ~95%
4. Eradication of Smallpox — Park's Key Points ⭐
| Event | Date |
|---|---|
| WHO intensified eradication campaign | 1967 |
| Strategy used | Surveillance & Containment (ring vaccination — NOT mass vaccination) |
| Last case in India | 24 May 1975 |
| India declared smallpox-free | 5 July 1975 |
| Last natural case worldwide | Somalia, 1977 |
| Global eradication confirmed | WHO, May 1980 |
| Virus still stored at | CDC Atlanta (USA) + VECTOR Institute (Russia) |
| WHO reserve stockpile | Vaccine for >200 million people |
- No animal reservoir
- No subclinical infectious cases (all cases visible)
- Effective vaccine available
- Stable single serotype
- Visible rash — easy case detection
PART 3: THE BIG COMPARISON TABLE (From Park's — Most Asked!)
| Feature | CHICKENPOX | SMALLPOX |
|---|---|---|
| Agent | VZV (Herpesvirus) | Variola (Poxvirus) |
| Incubation | 15 days (7–21) | 12 days (7–17) |
| Prodrome | Mild or absent | Severe |
| Rash distribution | CENTRIPETAL (trunk first) | CENTRIFUGAL (face first) |
| Palms & soles | Usually SPARED | Frequently involved |
| Axilla | Involved | Usually free |
| Rash surface | Flexor surfaces | Extensor + bony prominences |
| Vesicle type | Superficial, unilocular, dew-drop | Deep, multilocular, umbilicated |
| Inflammation around vesicle | PRESENT | ABSENT |
| Rash type | PLEOMORPHIC (all stages together) | MONOMORPHIC (one stage at a time) |
| Rash evolution | Very rapid (scabs in 4–7 days) | Slow, majestic (scabs in 10–14 days) |
| Fever pattern | Rises with each new crop | Secondary rise in pustular stage |
| Scabs | NOT infective | Infective |
| CFR | ~3 per 100,000 | ~30% (variola major) |
| Treatment | Acyclovir | No specific treatment |
Lines to Impress the Examiner 🌟
- "Chickenpox rash is pleomorphic because it appears in successive crops — all stages simultaneously. Smallpox is monomorphic — all lesions at the same stage, same time. This is the single most important clinical difference."
- "Chickenpox scabs are NOT infective — the virus dies before the pustular stage. This is different from smallpox where scabs are infective."
- "Aspirin is absolutely contraindicated in childhood chickenpox because it causes Reye's syndrome — a fatal hepatic encephalopathy."
- "Smallpox was eradicated because it had no animal reservoir, no subclinical infectious cases, a visible rash, and an effective vaccine — a unique combination that allowed the surveillance and containment strategy to work."
- "India was declared smallpox-free on 5th July 1975. WHO confirmed global eradication in May 1980 — making smallpox the first and only human disease ever to be eradicated."
- "After chickenpox, VZV lies dormant in dorsal root ganglia. When cell-mediated immunity wanes with age or immunosuppression, it reactivates as Herpes Zoster — a painful vesicular eruption along a dermatome."
Chickenpox Smallpox Cheatsheet
PDF Document · PDF
cheatsheet
HTML File · HTML
Create a quick-reference comparison card: Measles vs Rubella vs Chickenpox vs Smallpox
mkdir -p /home/daytona/workspace/comparison-card && echo "ready"
~/comparison-card/card.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Measles vs Rubella vs Chickenpox vs Smallpox</title>
<style>
@page { size: A4 landscape; margin: 8mm; }
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: Arial, Helvetica, sans-serif;
font-size: 8px;
color: #1a1a1a;
background: #fff;
padding: 6px;
line-height: 1.3;
}
/* ── BANNER ── */
.banner {
background: linear-gradient(135deg, #0d47a1 0%, #1565c0 40%, #283593 100%);
color: white;
text-align: center;
padding: 6px 10px 5px;
border-radius: 6px;
margin-bottom: 6px;
}
.banner h1 { font-size: 14px; font-weight: 900; letter-spacing: 0.8px; margin-bottom: 2px; }
.banner p { font-size: 7.5px; color: #bbdefb; }
/* ── COLOUR PALETTE ── */
/* measles = red #c62828 */
/* rubella = teal #00695c */
/* varicella= orange #e65100 */
/* smallpox = purple #4a148c */
/* ── MAIN COMPARISON TABLE ── */
.main-table { width: 100%; border-collapse: collapse; margin-bottom: 6px; font-size: 7.8px; }
/* header row */
.main-table thead tr th { padding: 5px 5px; font-size: 9px; font-weight: 900; color: white; border: 1px solid rgba(255,255,255,0.3); text-align: center; vertical-align: middle; }
.th-feat { background: #263238; text-align: left !important; width: 13%; font-size: 8px; }
.th-measles{ background: #c62828; width: 21.75%; }
.th-rubella{ background: #00695c; width: 21.75%; }
.th-varic { background: #e65100; width: 21.75%; }
.th-small { background: #4a148c; width: 21.75%; }
/* sub-header (category) rows */
.cat-row td { background: #eceff1; font-weight: 900; font-size: 7.5px; color: #37474f; padding: 3px 5px; border: 0.5px solid #b0bec5; text-transform: uppercase; letter-spacing: 0.5px; }
/* data rows */
.main-table tbody td { padding: 3px 5px; border: 0.5px solid #e0e0e0; vertical-align: top; line-height: 1.4; }
.main-table tbody tr:not(.cat-row):nth-child(even) td:nth-child(1) { background: #f5f5f5; }
.feat-col { font-weight: 700; background: #fafafa; font-size: 7.8px; }
/* colour tinting per disease column */
.col-m { background: #fff5f5; }
.col-r { background: #f0faf8; }
.col-v { background: #fff8f2; }
.col-s { background: #faf4ff; }
.main-table tbody tr:not(.cat-row):nth-child(even) .col-m { background: #ffebee; }
.main-table tbody tr:not(.cat-row):nth-child(even) .col-r { background: #e0f2f1; }
.main-table tbody tr:not(.cat-row):nth-child(even) .col-v { background: #fff3e0; }
.main-table tbody tr:not(.cat-row):nth-child(even) .col-s { background: #f3e5f5; }
/* highlight cells */
.hl { font-weight: 900; }
.hl-m { color: #c62828; }
.hl-r { color: #00695c; }
.hl-v { color: #e65100; }
.hl-s { color: #4a148c; }
.hl-shared { color: #1565c0; }
/* ── BOTTOM 3-PANEL ROW ── */
.bottom-row { display: grid; grid-template-columns: 1fr 1fr 1fr; gap: 6px; margin-bottom: 5px; }
.panel { border-radius: 4px; overflow: hidden; border: 1px solid #e0e0e0; }
.panel-hdr { padding: 4px 7px; font-size: 8.5px; font-weight: 900; color: white; }
.panel-body { padding: 5px 7px; font-size: 7.8px; line-height: 1.5; }
.green-hdr { background: #1b5e20; }
.blue-hdr { background: #0d47a1; }
.amber-hdr { background: #e65100; }
.mini-table { width: 100%; border-collapse: collapse; font-size: 7.5px; margin-top: 3px; }
.mini-table td { padding: 2px 4px; border: 0.5px solid #e0e0e0; vertical-align: top; }
.mini-table td:first-child { font-weight: 700; width: 42%; }
/* ── TIPS ROW ── */
.tips-banner { background: linear-gradient(90deg, #1b5e20, #2e7d32); color: white; font-size: 9px; font-weight: 900; padding: 4px 8px; border-radius: 4px 4px 0 0; letter-spacing: 0.5px; }
.tips-grid { display: grid; grid-template-columns: repeat(4,1fr); background: #e8f5e9; border: 1px solid #a5d6a7; border-top: none; border-radius: 0 0 4px 4px; }
.tip { padding: 4px 6px; border-right: 1px solid #c8e6c9; font-size: 7.5px; line-height: 1.5; }
.tip:last-child { border-right: none; }
.tip b { color: #1b5e20; }
/* ── FOOTER ── */
.footer { text-align: center; font-size: 6.5px; color: #9e9e9e; margin-top: 5px; border-top: 0.5px solid #e0e0e0; padding-top: 3px; }
/* dot legend */
.dot { display: inline-block; width: 8px; height: 8px; border-radius: 50%; vertical-align: middle; margin-right: 3px; }
.dot-m { background: #c62828; }
.dot-r { background: #00695c; }
.dot-v { background: #e65100; }
.dot-s { background: #4a148c; }
ul { padding-left: 10px; }
li { margin-bottom: 1px; }
</style>
</head>
<body>
<!-- BANNER -->
<div class="banner">
<h1>🔴 MEASLES vs 🟢 RUBELLA vs 🟠 CHICKENPOX vs 🟣 SMALLPOX — PSM Comparison Card</h1>
<p>MBBS 2nd Year | PSM Practical Exam | K. Park's Textbook of PSM | Harrison's 22e | Source: Park's PSM, Red Book 2021, ICMR Guidelines</p>
</div>
<!-- MAIN COMPARISON TABLE -->
<table class="main-table">
<thead>
<tr>
<th class="th-feat">FEATURE</th>
<th class="th-measles">🔴 MEASLES<br><span style="font-size:7.5px;font-weight:400;">(Rubeola / Hard Measles)</span></th>
<th class="th-rubella">🟢 RUBELLA<br><span style="font-size:7.5px;font-weight:400;">(German / 3-Day Measles)</span></th>
<th class="th-varic">🟠 CHICKENPOX<br><span style="font-size:7.5px;font-weight:400;">(Varicella)</span></th>
<th class="th-small">🟣 SMALLPOX<br><span style="font-size:7.5px;font-weight:400;">(Variola — ERADICATED)</span></th>
</tr>
</thead>
<tbody>
<!-- AETIOLOGY -->
<tr class="cat-row"><td colspan="5">⚗️ AETIOLOGY & BASICS</td></tr>
<tr>
<td class="feat-col">Causative virus</td>
<td class="col-m">Measles virus<br><span class="hl hl-m">Paramyxovirus (Morbillivirus)</span></td>
<td class="col-r">Rubella virus<br><span class="hl hl-r">Togavirus (Rubivirus)</span></td>
<td class="col-v">Varicella-Zoster Virus<br><span class="hl hl-v">Herpesvirus — Human α-HV3</span></td>
<td class="col-s">Variola virus<br><span class="hl hl-s">Poxvirus (Orthopoxvirus)</span></td>
</tr>
<tr>
<td class="feat-col">Nucleic acid</td>
<td class="col-m"><span class="hl hl-m">RNA virus</span></td>
<td class="col-r"><span class="hl hl-r">RNA virus</span></td>
<td class="col-v"><span class="hl hl-v">DNA virus</span></td>
<td class="col-s"><span class="hl hl-s">DNA virus</span></td>
</tr>
<tr>
<td class="feat-col">Reservoir</td>
<td class="col-m">Humans only</td>
<td class="col-r">Humans only</td>
<td class="col-v">Humans only</td>
<td class="col-s">Humans only</td>
</tr>
<tr>
<td class="feat-col">Transmission</td>
<td class="col-m">Droplet + airborne<br><span class="hl hl-m">Most contagious of all!</span></td>
<td class="col-r">Droplet infection</td>
<td class="col-v">Droplet + contact + <span class="hl hl-v">airborne</span></td>
<td class="col-s">Droplet + direct contact</td>
</tr>
<tr>
<td class="feat-col">Incubation period</td>
<td class="col-m"><span class="hl hl-m">10–12 days</span></td>
<td class="col-r"><span class="hl hl-r">14–21 days (avg 18)</span></td>
<td class="col-v"><span class="hl hl-v">15 days (7–21)</span></td>
<td class="col-s"><span class="hl hl-s">12 days (7–17)</span></td>
</tr>
<tr>
<td class="feat-col">Communicability</td>
<td class="col-m">4 days before → 4 days after rash</td>
<td class="col-r">7 days before → 7 days after rash</td>
<td class="col-v">1–2 days before → 4–5 days after rash (till crusted)</td>
<td class="col-s">Onset of oral lesions → all crusts fall off (~3–4 wks)</td>
</tr>
<tr>
<td class="feat-col">Secondary attack rate</td>
<td class="col-m"><span class="hl hl-m">90–95%</span> (highest!)</td>
<td class="col-r">~10–30%</td>
<td class="col-v"><span class="hl hl-v">~85%</span> household contacts</td>
<td class="col-s">Variable; lower than measles</td>
</tr>
<!-- PRODROME -->
<tr class="cat-row"><td colspan="5">🌡️ PRODROME (Before Rash)</td></tr>
<tr>
<td class="feat-col">Severity of prodrome</td>
<td class="col-m"><span class="hl hl-m">3–4 days, severe</span><br>High fever</td>
<td class="col-r"><span class="hl hl-r">1–5 days, mild</span><br>Low fever, malaise</td>
<td class="col-v"><span class="hl hl-v">1–2 days, mild</span><br>Often absent in children</td>
<td class="col-s"><span class="hl hl-s">2–4 days, VERY severe</span><br>Bedridden</td>
</tr>
<tr>
<td class="feat-col">3 C's (Catarrhal stage)</td>
<td class="col-m"><span class="hl hl-m">Present! ★</span><br>Cough, Coryza, Conjunctivitis</td>
<td class="col-r">Absent</td>
<td class="col-v">Absent</td>
<td class="col-s">Absent</td>
</tr>
<tr>
<td class="feat-col">Koplik's spots</td>
<td class="col-m"><span class="hl hl-m">PRESENT ★ (Pathognomonic)</span><br>White spots on buccal mucosa</td>
<td class="col-r">Absent</td>
<td class="col-v">Absent</td>
<td class="col-s">Absent</td>
</tr>
<tr>
<td class="feat-col">Backache</td>
<td class="col-m">Mild</td>
<td class="col-r">Absent / mild</td>
<td class="col-v">Absent</td>
<td class="col-s"><span class="hl hl-s">SEVERE, characteristic ★</span></td>
</tr>
<!-- RASH -->
<tr class="cat-row"><td colspan="5">🌺 RASH CHARACTERISTICS (Most Asked!)</td></tr>
<tr>
<td class="feat-col">Distribution</td>
<td class="col-m"><span class="hl hl-m">Centrifugal</span><br>Face → neck → trunk → limbs</td>
<td class="col-r"><span class="hl hl-r">Centrifugal</span><br>Face → trunk → limbs</td>
<td class="col-v"><span class="hl hl-v">CENTRIPETAL ★</span><br>Trunk → face → limbs</td>
<td class="col-s"><span class="hl hl-s">Centrifugal ★</span><br>Face → arms → trunk → legs</td>
</tr>
<tr>
<td class="feat-col">Palms & soles</td>
<td class="col-m">Not typically affected</td>
<td class="col-r">Not typically affected</td>
<td class="col-v"><span class="hl hl-v">Usually SPARED ★</span></td>
<td class="col-s"><span class="hl hl-s">FREQUENTLY involved ★</span></td>
</tr>
<tr>
<td class="feat-col">Rash type</td>
<td class="col-m">Maculopapular<br><span class="hl hl-m">coalescent, blotchy</span></td>
<td class="col-r">Maculopapular<br><span class="hl hl-r">discrete, fine, faint</span></td>
<td class="col-v"><span class="hl hl-v">Vesicular</span><br>"Dew-drops on skin"</td>
<td class="col-s"><span class="hl hl-s">Vesiculopustular</span><br>"Pearls of pus"</td>
</tr>
<tr>
<td class="feat-col">Vesicle depth</td>
<td class="col-m">No vesicles</td>
<td class="col-r">No vesicles</td>
<td class="col-v"><span class="hl hl-v">SUPERFICIAL, unilocular</span><br>easily ruptured</td>
<td class="col-s"><span class="hl hl-s">DEEP, multilocular</span><br>hard, umbilicated</td>
</tr>
<tr>
<td class="feat-col">Inflammation around lesion</td>
<td class="col-m">—</td>
<td class="col-r">—</td>
<td class="col-v"><span class="hl hl-v">PRESENT (erythematous halo)</span></td>
<td class="col-s"><span class="hl hl-s">ABSENT</span></td>
</tr>
<tr>
<td class="feat-col">Stages of rash (Park's)</td>
<td class="col-m">MONOMORPHIC<br>Macular → papular (coalesce)</td>
<td class="col-r">MONOMORPHIC<br>Maculopapular only (3 days)</td>
<td class="col-v"><span class="hl hl-v">PLEOMORPHIC ★</span><br>All stages simultaneously (crops)</td>
<td class="col-s"><span class="hl hl-s">MONOMORPHIC ★</span><br>One stage at a time</td>
</tr>
<tr>
<td class="feat-col">Rash duration</td>
<td class="col-m"><span class="hl hl-m">4–7 days</span></td>
<td class="col-r"><span class="hl hl-r">3 days only</span></td>
<td class="col-v">Scabs in <span class="hl hl-v">4–7 days</span></td>
<td class="col-s">Scabs in <span class="hl hl-s">10–14 days</span> (slow!)</td>
</tr>
<tr>
<td class="feat-col">Axilla involvement</td>
<td class="col-m">—</td>
<td class="col-r">—</td>
<td class="col-v"><span class="hl hl-v">Affected</span></td>
<td class="col-s"><span class="hl hl-s">Usually FREE</span></td>
</tr>
<tr>
<td class="feat-col">Scarring</td>
<td class="col-m">Minimal</td>
<td class="col-r">None</td>
<td class="col-v">Pitted scars if scratched</td>
<td class="col-s"><span class="hl hl-s">SEVERE, permanent ★</span></td>
</tr>
<!-- LYMPH NODES -->
<tr class="cat-row"><td colspan="5">🫁 LYMPHADENOPATHY & FEVER</td></tr>
<tr>
<td class="feat-col">Lymphadenopathy</td>
<td class="col-m">Cervical lymph nodes<br>+ generalised</td>
<td class="col-r"><span class="hl hl-r">Occipital + post-auricular ★</span><br>TENDER — hallmark!</td>
<td class="col-v">—</td>
<td class="col-s">—</td>
</tr>
<tr>
<td class="feat-col">Fever pattern</td>
<td class="col-m">High fever; falls at rash onset</td>
<td class="col-r">Low grade or absent</td>
<td class="col-v">Rises with each <span class="hl hl-v">new crop</span></td>
<td class="col-s">Falls with rash; <span class="hl hl-s">secondary rise</span> in pustular stage</td>
</tr>
<tr>
<td class="feat-col">Infectivity of scabs</td>
<td class="col-m">No scabs formed</td>
<td class="col-r">No scabs formed</td>
<td class="col-v"><span class="hl hl-v">Scabs NOT infective ★</span></td>
<td class="col-s"><span class="hl hl-s">Scabs ARE infective ★</span></td>
</tr>
<!-- SPECIAL FEATURES -->
<tr class="cat-row"><td colspan="5">⭐ SPECIAL / UNIQUE FEATURES</td></tr>
<tr>
<td class="feat-col">Pathognomonic sign</td>
<td class="col-m"><span class="hl hl-m">Koplik's spots</span></td>
<td class="col-r"><span class="hl hl-r">Occipital LN + 3-day rash</span></td>
<td class="col-v"><span class="hl hl-v">Pleomorphic vesicles (dew-drop)</span></td>
<td class="col-s"><span class="hl hl-s">Deep umbilicated pustules on face</span></td>
</tr>
<tr>
<td class="feat-col">Subclinical cases</td>
<td class="col-m">Rare</td>
<td class="col-r"><span class="hl hl-r">50% subclinical! ★</span></td>
<td class="col-v">Rare</td>
<td class="col-s"><span class="hl hl-s">None (all visible)</span></td>
</tr>
<tr>
<td class="feat-col">Mucosal involvement</td>
<td class="col-m">Oral (Koplik's), conjunctiva</td>
<td class="col-r">Mild oral</td>
<td class="col-v">Buccal, pharyngeal mucosa</td>
<td class="col-s">Oral/pharyngeal — patient becomes <span class="hl hl-s">infectious</span></td>
</tr>
<tr>
<td class="feat-col">Pregnancy danger</td>
<td class="col-m">Pneumonia, preterm birth</td>
<td class="col-r"><span class="hl hl-r">CRITICAL → CRS ★</span><br>CCC: Cataract+Cardiac+Cochlear</td>
<td class="col-v">Neonatal varicella, pneumonia</td>
<td class="col-s">CFR highest in pregnancy (~30%)</td>
</tr>
<tr>
<td class="feat-col">Arthritis in adults</td>
<td class="col-m">Uncommon</td>
<td class="col-r"><span class="hl hl-r">Common (esp. women) ★</span></td>
<td class="col-v">Uncommon</td>
<td class="col-s">—</td>
</tr>
<tr>
<td class="feat-col">Latency / Reactivation</td>
<td class="col-m">None</td>
<td class="col-r">None</td>
<td class="col-v"><span class="hl hl-v">Herpes Zoster ★</span><br>Reactivates from dorsal root ganglia</td>
<td class="col-s">None</td>
</tr>
<!-- COMPLICATIONS -->
<tr class="cat-row"><td colspan="5">⚡ KEY COMPLICATIONS</td></tr>
<tr>
<td class="feat-col">Most feared complication</td>
<td class="col-m">Pneumonia, Encephalitis<br>Subacute sclerosing panencephalitis (SSPE)</td>
<td class="col-r"><span class="hl hl-r">CRS (Congenital Rubella Syndrome)</span></td>
<td class="col-v">Secondary bacterial infection<br>Pneumonia (adults), Reye's syndrome</td>
<td class="col-s"><span class="hl hl-s">Death (CFR 30%)</span><br>Hemorrhagic type CFR ~100%</td>
</tr>
<tr>
<td class="feat-col">Drug contraindication</td>
<td class="col-m">—</td>
<td class="col-r">—</td>
<td class="col-v"><span class="hl hl-v">ASPIRIN → Reye's syndrome ★</span></td>
<td class="col-s">—</td>
</tr>
<!-- TREATMENT & VACCINE -->
<tr class="cat-row"><td colspan="5">💊 TREATMENT & VACCINE</td></tr>
<tr>
<td class="feat-col">Specific treatment</td>
<td class="col-m">Vitamin A + supportive<br>(Vit A reduces mortality!)</td>
<td class="col-r">Supportive only<br>No antiviral</td>
<td class="col-v"><span class="hl hl-v">ACYCLOVIR ★</span><br>(esp. immunocompromised)</td>
<td class="col-s">No specific antiviral<br>Supportive only</td>
</tr>
<tr>
<td class="feat-col">Vaccine type</td>
<td class="col-m">Live attenuated<br>(MMR)</td>
<td class="col-r">Live attenuated<br>(MMR)</td>
<td class="col-v">Live attenuated<br>(Oka strain; separate or MMRV)</td>
<td class="col-s"><span class="hl hl-s">Live vaccinia virus ★</span><br>DISCONTINUED after 1980</td>
</tr>
<tr>
<td class="feat-col">Vaccine schedule (Nepal/India)</td>
<td class="col-m">MMR: 9 m + 15 m</td>
<td class="col-r">MMR: 9 m + 15 m</td>
<td class="col-v">12–15 m + 4–6 yr</td>
<td class="col-s">No routine vaccination<br>(since 1980)</td>
</tr>
<tr>
<td class="feat-col">Post-exposure prophylaxis</td>
<td class="col-m">Vaccine within 72 h OR<br>Normal IG within 6 days</td>
<td class="col-r">Vaccine (non-pregnant)<br>No benefit post-exposure in pregnancy</td>
<td class="col-v"><span class="hl hl-v">Vaccine within 5 days</span><br>VZIG within 72 h (high-risk)</td>
<td class="col-s">Ring vaccination</td>
</tr>
<tr>
<td class="feat-col">Vaccine contraindication</td>
<td class="col-m">Pregnancy, severe immunocomp.</td>
<td class="col-r">Pregnancy (delay 1 month)</td>
<td class="col-v">Pregnancy (delay 4 weeks)</td>
<td class="col-s">N/A (routine not given)</td>
</tr>
<!-- STATUS -->
<tr class="cat-row"><td colspan="5">🌍 CURRENT STATUS & ERADICATION</td></tr>
<tr>
<td class="feat-col">Current status</td>
<td class="col-m">Ongoing; elimination target<br>WHO target: eliminate regionally</td>
<td class="col-r">Ongoing; CRS prevention priority</td>
<td class="col-v">Ongoing worldwide<br>~4.2 M hospitalisations/yr</td>
<td class="col-s"><span class="hl hl-s">GLOBALLY ERADICATED 1980 ★</span><br>First human disease eradicated!</td>
</tr>
<tr>
<td class="feat-col">CFR (unvaccinated)</td>
<td class="col-m">1–3 per 1000</td>
<td class="col-r">Very low<br>(<1 per 1000)</td>
<td class="col-v">~3 per 100,000</td>
<td class="col-s"><span class="hl hl-s">~30% (Variola major)</span></td>
</tr>
</tbody>
</table>
<!-- BOTTOM 3-PANEL ROW -->
<div class="bottom-row">
<!-- MEMORY TRICKS -->
<div class="panel">
<div class="panel-hdr green-hdr">🧠 MEMORY TRICKS — NEVER FORGET!</div>
<div class="panel-body">
<b>"MERK" = Measles, EaR (rubella), Koplik's (measles only)</b><br><br>
<b>Rash distribution:</b><br>
<span style="color:#c62828;">●</span> Measles = face→trunk (centri<b>F</b>ugal = <b>F</b>ace first)<br>
<span style="color:#00695c;">●</span> Rubella = face→trunk (centri<b>F</b>ugal = <b>F</b>ace first)<br>
<span style="color:#e65100;">●</span> Chickenpox = trunk→limbs (centri<b>P</b>etal = <b>P</b>ericentral/trunk first)<br>
<span style="color:#4a148c;">●</span> Smallpox = face→trunk (<b>F</b>ace = <b>F</b>earful severity)<br><br>
<b>Rash type trick:</b><br>
Chickenpox = <b>P</b>leomorphic = <b>P</b>lenty of stages at once<br>
Smallpox = <b>M</b>onomorphic = <b>M</b>arching one stage at a time<br><br>
<b>Vesicle depth:</b><br>
Chickenpox = <b>S</b>uperficial = <b>S</b>afe (low CFR)<br>
Smallpox = <b>D</b>eep = <b>D</b>eadly (30% CFR)<br><br>
<b>CRS = "3 C's":</b> Cataract + Cardiac + Cochlear deafness<br>
<b>Measles 3C's:</b> Cough + Coryza + Conjunctivitis (prodrome)<br><br>
<b>Incubation (shortest→longest):</b><br>
Measles (10–12) < Smallpox (12) < Chickenpox (15) < Rubella (18 avg)
</div>
</div>
<!-- MCQ BANK -->
<div class="panel">
<div class="panel-hdr blue-hdr">📝 HIGH-YIELD MCQs</div>
<div class="panel-body">
<table class="mini-table">
<tr><td><b>Only disease with Koplik's spots?</b></td><td><span class="hl hl-m">Measles</span></td></tr>
<tr><td><b>Rash lasts only 3 days?</b></td><td><span class="hl hl-r">Rubella</span></td></tr>
<tr><td><b>Rash centripetal (trunk first)?</b></td><td><span class="hl hl-v">Chickenpox</span></td></tr>
<tr><td><b>Palms & soles always involved?</b></td><td><span class="hl hl-s">Smallpox</span></td></tr>
<tr><td><b>Pleomorphic rash?</b></td><td><span class="hl hl-v">Chickenpox</span></td></tr>
<tr><td><b>Monomorphic rash?</b></td><td><span class="hl hl-s">Smallpox</span></td></tr>
<tr><td><b>50% subclinical cases?</b></td><td><span class="hl hl-r">Rubella</span></td></tr>
<tr><td><b>Scabs NOT infective?</b></td><td><span class="hl hl-v">Chickenpox</span></td></tr>
<tr><td><b>Aspirin contraindicated?</b></td><td><span class="hl hl-v">Chickenpox (Reye's)</span></td></tr>
<tr><td><b>Post-auricular LN tender?</b></td><td><span class="hl hl-r">Rubella</span></td></tr>
<tr><td><b>Arthritis common in adult women?</b></td><td><span class="hl hl-r">Rubella</span></td></tr>
<tr><td><b>CRS triad (Gregg's)?</b></td><td><span class="hl hl-r">Rubella: Cat+Card+Coch</span></td></tr>
<tr><td><b>Herpes zoster reactivation?</b></td><td><span class="hl hl-v">Chickenpox (VZV)</span></td></tr>
<tr><td><b>Globally eradicated 1980?</b></td><td><span class="hl hl-s">Smallpox</span></td></tr>
<tr><td><b>CFR ~30%?</b></td><td><span class="hl hl-s">Smallpox (Variola major)</span></td></tr>
<tr><td><b>Vaccine = live vaccinia virus?</b></td><td><span class="hl hl-s">Smallpox (discontinued)</span></td></tr>
<tr><td><b>Vitamin A reduces mortality?</b></td><td><span class="hl hl-m">Measles</span></td></tr>
<tr><td><b>India declared free: 5 Jul 1975?</b></td><td><span class="hl hl-s">Smallpox</span></td></tr>
</table>
</div>
</div>
<!-- COLOUR-CODED RECAP -->
<div class="panel">
<div class="panel-hdr amber-hdr">⚡ RAPID RECALL — ONE GLANCE!</div>
<div class="panel-body">
<table class="mini-table">
<tr><td colspan="2" style="background:#c62828;color:white;font-weight:900;text-align:center;">🔴 MEASLES (Paramyxovirus, RNA)</td></tr>
<tr><td>Incubation</td><td>10–12 days</td></tr>
<tr><td>Prodrome</td><td>3C's + Koplik's ★</td></tr>
<tr><td>Rash</td><td>Maculopapular, centrifugal, 4–7 days</td></tr>
<tr><td>Treatment</td><td>Vitamin A + supportive</td></tr>
<tr><td>Vaccine</td><td>MMR (9 m + 15 m)</td></tr>
</table>
<br>
<table class="mini-table">
<tr><td colspan="2" style="background:#00695c;color:white;font-weight:900;text-align:center;">🟢 RUBELLA (Togavirus, RNA)</td></tr>
<tr><td>Incubation</td><td>14–21 days (avg 18)</td></tr>
<tr><td>Hallmark</td><td>Occipital/post-auricular LN ★</td></tr>
<tr><td>Rash</td><td>Fine maculopapular, 3 days only</td></tr>
<tr><td>Danger</td><td>CRS (Cataract+Cardiac+Cochlear)</td></tr>
<tr><td>Vaccine</td><td>MMR (9 m + 15 m)</td></tr>
</table>
<br>
<table class="mini-table">
<tr><td colspan="2" style="background:#e65100;color:white;font-weight:900;text-align:center;">🟠 CHICKENPOX (VZV, DNA)</td></tr>
<tr><td>Incubation</td><td>15 days (7–21)</td></tr>
<tr><td>Rash</td><td>CENTRIPETAL; PLEOMORPHIC; dew-drop ★</td></tr>
<tr><td>No aspirin!</td><td>Reye's syndrome risk ★</td></tr>
<tr><td>Treatment</td><td>Acyclovir</td></tr>
<tr><td>Latency</td><td>→ Herpes Zoster later in life</td></tr>
</table>
<br>
<table class="mini-table">
<tr><td colspan="2" style="background:#4a148c;color:white;font-weight:900;text-align:center;">🟣 SMALLPOX (Variola, DNA) — ERADICATED</td></tr>
<tr><td>Incubation</td><td>12 days (7–17)</td></tr>
<tr><td>Rash</td><td>CENTRIFUGAL; MONOMORPHIC; deep pustules ★</td></tr>
<tr><td>CFR</td><td>~30% (Variola major)</td></tr>
<tr><td>Eradicated</td><td>WHO May 1980 (India free: 5 Jul 1975)</td></tr>
<tr><td>Vaccine</td><td>Live vaccinia — discontinued!</td></tr>
</table>
</div>
</div>
</div><!-- end bottom-row -->
<!-- EXAMINER TIPS -->
<div>
<div class="tips-banner">🌟 LINES TO IMPRESS THE EXAMINER</div>
<div class="tips-grid">
<div class="tip">
✔ <b>"Measles is the MOST contagious of all four — secondary attack rate 90–95%. Koplik's spots are pathognomonic and appear before the rash."</b>
</div>
<div class="tip">
✔ <b>"50% of rubella cases are subclinical — this is why pregnant women unknowingly get infected and transmit CRS. Gregg's triad = Cataract + Cardiac (PDA) + Cochlear deafness."</b>
</div>
<div class="tip">
✔ <b>"Chickenpox rash is pleomorphic (successive crops) and centripetal (trunk first). Smallpox is monomorphic (one stage at a time) and centrifugal (face first) — the most important clinical distinction."</b>
</div>
<div class="tip">
✔ <b>"Smallpox was eradicated because no animal reservoir, no subclinical cases, visible rash, effective vaccine — the 1967 WHO surveillance & containment strategy worked perfectly. India was declared free on 5 July 1975; WHO confirmed global eradication May 1980."</b>
</div>
</div>
</div>
<div class="footer">
PSM Comparison Card | MBBS 2nd Year | Source: Park's Textbook of PSM (K. Park) | Harrison's Principles of Internal Medicine 22e | Red Book 2021 | ICMR-NIN 2020 | Generated by Orris — All the best for your exam! 🎓
</div>
</body>
</html>
libreoffice --headless --convert-to pdf --outdir /tmp/ /home/daytona/workspace/comparison-card/card.html 2>&1 && ls -lh /tmp/card.pdf && cp /tmp/card.pdf /home/daytona/workspace/comparison-card/Measles_Rubella_Chickenpox_Smallpox_Comparison.pdf && python3 -c "from pypdf import PdfReader; r=PdfReader('/home/daytona/workspace/comparison-card/Measles_Rubella_Chickenpox_Smallpox_Comparison.pdf'); print(f'Pages: {len(r.pages)}, Size: OK')"
Measles Rubella Chickenpox Smallpox Comparison
PDF Document · PDF
card
HTML File · HTML
| Section | Content |
|---|---|
| Main comparison table | 30+ rows covering aetiology, prodrome, rash characteristics, LN, fever, complications, treatment, vaccine, current status — all 4 diseases side by side |
| Colour coding | 🔴 Red = Measles, 🟢 Teal = Rubella, 🟠 Orange = Chickenpox, 🟣 Purple = Smallpox |
| Memory tricks panel | Centripetal vs centrifugal, pleomorphic vs monomorphic, incubation order |
| 18 MCQs | Every high-yield question with the correct disease answer |
| Rapid recall panel | One mini-table per disease — read in 2 minutes |
| Examiner tips | 4 impressive lines covering all 4 diseases together |
Tomorrow is my psm practical exam of mbbs 2nd year from nepal. I dont know about blindness . External maam surely ask me this topic . Could you please provide me about blindness from k park psm in easy language so that i will never forget it . And the external will impress
mkdir -p /home/daytona/workspace/blindness && echo "ready"
~/blindness/blindness_cheatsheet.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Blindness – PSM Quick Reference (K. Park)</title>
<style>
@page { size: A4; margin: 9mm; }
* { margin:0; padding:0; box-sizing:border-box; }
body { font-family: Arial, Helvetica, sans-serif; font-size:8px; color:#1a1a1a; background:#fff; padding:7px; line-height:1.35; }
.banner { background:linear-gradient(135deg,#1a237e,#283593,#3949ab); color:white; text-align:center; padding:7px 10px 6px; border-radius:6px; margin-bottom:6px; }
.banner h1 { font-size:15px; font-weight:900; letter-spacing:.8px; margin-bottom:2px; }
.banner p { font-size:7.5px; color:#c5cae9; }
.two-col { display:grid; grid-template-columns:1fr 1fr; gap:6px; margin-bottom:6px; }
.three-col { display:grid; grid-template-columns:1fr 1fr 1fr; gap:6px; margin-bottom:6px; }
.card { border-radius:5px; overflow:hidden; border:1px solid #e0e0e0; }
.card-header { padding:5px 8px; font-size:9.5px; font-weight:900; color:white; }
.card-body { padding:5px 7px; }
/* colour palette */
.navy { background:#1a237e; }
.blue { background:#1565c0; }
.green { background:#1b5e20; }
.teal { background:#004d40; }
.red { background:#b71c1c; }
.amber { background:#e65100; }
.purple{ background:#4a148c; }
.grey { background:#37474f; }
.sub { display:block; font-size:7.5px; font-weight:700; text-transform:uppercase; letter-spacing:.4px; margin:4px 0 2px; padding-bottom:1px; border-bottom:1px solid #e0e0e0; }
.sub-b { color:#1565c0; border-color:#90caf9; }
.sub-g { color:#1b5e20; border-color:#a5d6a7; }
.sub-r { color:#b71c1c; border-color:#ef9a9a; }
.sub-a { color:#e65100; border-color:#ffcc80; }
.sub-p { color:#4a148c; border-color:#ce93d8; }
.sub-t { color:#004d40; border-color:#80cbc4; }
.sub-gr{ color:#37474f; border-color:#b0bec5; }
table { width:100%; border-collapse:collapse; margin-bottom:3px; font-size:8px; }
thead th { padding:3px 4px; text-align:center; font-size:7.5px; font-weight:700; color:white; border:.5px solid rgba(255,255,255,.3); }
.th-b thead th { background:#1565c0; }
.th-g thead th { background:#2e7d32; }
.th-r thead th { background:#c62828; }
.th-a thead th { background:#e65100; }
.th-t thead th { background:#00796b; }
tbody td { padding:2.5px 4px; border:.5px solid #e0e0e0; vertical-align:top; }
tbody td:first-child { font-weight:600; }
tbody tr:nth-child(even) { background:#fafafa; }
.box { border-radius:4px; padding:5px 7px; margin-bottom:3px; font-size:8px; }
.box-b { background:#e3f2fd; border-left:3px solid #1565c0; }
.box-g { background:#e8f5e9; border-left:3px solid #2e7d32; }
.box-r { background:#ffebee; border-left:3px solid #c62828; }
.box-a { background:#fff3e0; border-left:3px solid #e65100; }
.box-p { background:#f3e5f5; border-left:3px solid #6a1b9a; }
.box-t { background:#e0f2f1; border-left:3px solid #004d40; }
.box-y { background:#fffde7; border-left:3px solid #f9a825; }
.box .title { font-size:8.5px; font-weight:900; display:block; margin-bottom:2px; }
ul { padding-left:10px; margin:0; }
li { margin-bottom:1.5px; }
.mcq-banner { background:linear-gradient(90deg,#4a148c,#6a1b9a); color:white; font-size:9.5px; font-weight:900; padding:4px 8px; border-radius:4px 4px 0 0; letter-spacing:.5px; }
.mcq-grid { display:grid; grid-template-columns:1fr 1fr 1fr; background:#f3e5f5; border:1px solid #ce93d8; border-top:none; border-radius:0 0 4px 4px; }
.mcq-item { padding:4px 7px; border-right:1px solid #e1bee7; border-bottom:1px solid #e1bee7; font-size:7.8px; line-height:1.4; }
.mcq-q { color:#4a148c; font-weight:700; }
.mcq-a { color:#b71c1c; font-weight:900; }
.tips-banner { background:linear-gradient(90deg,#1b5e20,#2e7d32); color:white; font-size:9.5px; font-weight:900; padding:4px 8px; border-radius:4px 4px 0 0; letter-spacing:.5px; }
.tips-grid { display:grid; grid-template-columns:1fr 1fr 1fr; background:#e8f5e9; border:1px solid #a5d6a7; border-top:none; border-radius:0 0 4px 4px; }
.tip-item { padding:4px 7px; border-right:1px solid #c8e6c9; font-size:7.8px; line-height:1.5; }
.tip-item:last-child { border-right:none; }
.tip-item b { color:#1b5e20; }
.footer { text-align:center; font-size:6.8px; color:#9e9e9e; margin-top:5px; padding-top:3px; border-top:.5px solid #e0e0e0; }
.badge { display:inline-block; padding:1px 5px; border-radius:10px; font-size:7px; font-weight:700; margin-left:3px; }
.b-red { background:#b71c1c; color:white; }
.b-grn { background:#1b5e20; color:white; }
.b-blu { background:#1565c0; color:white; }
.b-amb { background:#e65100; color:white; }
</style>
</head>
<body>
<!-- BANNER -->
<div class="banner">
<h1>👁️ BLINDNESS — PSM Quick Reference (K. Park)</h1>
<p>MBBS 2nd Year | PSM Practical Exam | Park's Textbook of PSM | WHO ICD-11 | Vision 2020 | NPCB India</p>
</div>
<!-- ROW 1: DEFINITION + CLASSIFICATION + MAGNITUDE -->
<div class="two-col">
<!-- DEFINITION & CLASSIFICATION -->
<div class="card">
<div class="card-header navy">📖 DEFINITION & CLASSIFICATION (WHO / ICD-11)</div>
<div class="card-body">
<div class="box box-b">
<span class="title">WHO DEFINITION OF BLINDNESS (Park's)</span>
<b>"Visual acuity of less than 3/60 (Snellen) or its equivalent"</b><br>
— Proposed by WHO; adopted at 25th World Health Assembly, 1972<br>
(Earlier, 65 different definitions of blindness existed worldwide!)
</div>
<span class="sub sub-b">ICD-11 (2018): DISTANCE VISION IMPAIRMENT CATEGORIES</span>
<table class="th-b">
<thead><tr><th>Category</th><th>Visual Acuity</th><th>Memory Aid</th></tr></thead>
<tbody>
<tr><td>Mild impairment</td><td>Worse than <b>6/12</b></td><td>Can't read newspaper</td></tr>
<tr><td>Moderate impairment</td><td>Worse than <b>6/18</b></td><td>Low vision</td></tr>
<tr><td>Severe impairment</td><td>Worse than <b>6/60</b></td><td>Finger counting</td></tr>
<tr><td><b>BLINDNESS ★</b></td><td>Worse than <b>3/60</b></td><td>Perception of light only</td></tr>
</tbody>
</table>
<div class="box box-a" style="margin-top:4px;">
<span class="title">NEAR VISION IMPAIRMENT</span>
Worse than <b>N6 or M0.8 at 40 cm</b> with existing correction (presbyopia main cause — 826 million affected!)
</div>
<span class="sub sub-b">OLD TERMINOLOGY (Still asked in exams)</span>
<table>
<tbody>
<tr><td><b>Economic blindness</b></td><td>VA < 6/60 (cannot earn a living)</td></tr>
<tr><td><b>Social blindness</b></td><td>VA < 3/60 (needs social support)</td></tr>
<tr><td><b>Total blindness</b></td><td>No light perception at all</td></tr>
</tbody>
</table>
<span class="sub sub-b">TYPES: AVOIDABLE vs UNAVOIDABLE</span>
<div class="box box-g">
<b>~80% of all blindness is AVOIDABLE</b> (preventable OR treatable)<br>
Only ~20% is unavoidable (congenital anomalies, hereditary, etc.)<br>
This is the most important PSM concept about blindness!
</div>
</div>
</div>
<!-- GLOBAL MAGNITUDE -->
<div class="card">
<div class="card-header blue">🌍 MAGNITUDE OF THE PROBLEM (Park's)</div>
<div class="card-body">
<span class="sub sub-b">GLOBAL FIGURES</span>
<div class="box box-b">
<b>1 billion people</b> have vision impairment that could be prevented/treated.<br>
82% of all visually impaired are <b>aged ≥50 years</b>.<br>
19 million children are visually impaired; 1.4 million irreversibly blind for life.
</div>
<span class="sub sub-b">GLOBAL CAUSES OF BLINDNESS (Park's Table)</span>
<table class="th-b">
<thead><tr><th>Cause</th><th>% of Blindness</th></tr></thead>
<tbody>
<tr><td><b>1. Un-operated Cataract ★</b></td><td><b>35%</b> — #1 cause of blindness!</td></tr>
<tr><td><b>2. Uncorrected Refractive Error</b></td><td><b>21%</b></td></tr>
<tr><td><b>3. Glaucoma</b></td><td><b>8%</b></td></tr>
<tr><td>4. Age-related Macular Degeneration</td><td>~5%</td></tr>
<tr><td>5. Corneal opacities</td><td>~4%</td></tr>
<tr><td>6. Diabetic Retinopathy</td><td>~3%</td></tr>
<tr><td>7. Trachoma</td><td>~2%</td></tr>
</tbody>
</table>
<span class="sub sub-b">CAUSES OF MODERATE-SEVERE VISION IMPAIRMENT</span>
<table class="th-b">
<thead><tr><th>Cause</th><th>%</th></tr></thead>
<tbody>
<tr><td><b>1. Uncorrected Refractive Errors ★</b></td><td><b>53%</b> — #1 cause of visual impairment!</td></tr>
<tr><td><b>2. Un-operated Cataract</b></td><td><b>25%</b></td></tr>
<tr><td>3. Age-related Macular Degeneration</td><td>4%</td></tr>
<tr><td>4. Glaucoma</td><td>2%</td></tr>
<tr><td>5. Diabetic Retinopathy</td><td>1%</td></tr>
</tbody>
</table>
<div class="box box-r" style="margin-top:3px;font-size:7.8px;">
<b>KEY DISTINCTION (Examiners love this!):</b><br>
#1 cause of <b>BLINDNESS</b> = <b>Cataract (35%)</b><br>
#1 cause of <b>VISUAL IMPAIRMENT</b> = <b>Refractive Error (53%)</b>
</div>
<span class="sub sub-b">SOUTH-EAST ASIA REGION (SEAR) / INDIA</span>
<ul>
<li>Cataract = <b>50–80%</b> of all blindness in SEAR</li>
<li>India: ~1.2 crore (12 million) blind people</li>
<li>Cataract alone accounts for <b>62.6%</b> of blindness in India</li>
<li>Childhood blindness main cause: <b>Xerophthalmia</b> (Vit A deficiency)</li>
<li>Emerging: glaucoma, diabetic retinopathy, corneal ulcer, trauma</li>
</ul>
</div>
</div>
</div>
<!-- ROW 2: CAUSES IN DETAIL + TRACHOMA -->
<div class="two-col">
<!-- MAJOR CAUSES IN DETAIL -->
<div class="card">
<div class="card-header green">🔍 MAJOR CAUSES OF BLINDNESS — DETAILS</div>
<div class="card-body">
<span class="sub sub-g">1. CATARACT (Most Common Cause of Blindness)</span>
<ul>
<li>Opacity of the lens — causes gradual painless loss of vision</li>
<li>Age-related (senile cataract) = most common type</li>
<li>Also: congenital, traumatic, diabetic, radiation-induced</li>
<li><b>Treatment: Surgical removal</b> (ECCE + IOL implant)</li>
<li>Fully treatable — most important reason to prevent avoidable blindness</li>
<li>Key strategy: Cataract Surgical Rate (CSR) — India target: 6 million/year</li>
</ul>
<span class="sub sub-g">2. REFRACTIVE ERRORS (#1 Visual Impairment)</span>
<ul>
<li>Myopia, hypermetropia, astigmatism, presbyopia</li>
<li>Presbyopia = loss of near vision with age (826 million affected globally!)</li>
<li><b>Treatment: Spectacles / contact lenses / refractive surgery</b></li>
<li>Cheapest, most effective intervention for visual impairment</li>
</ul>
<span class="sub sub-g">3. GLAUCOMA (#3 Cause of Blindness)</span>
<ul>
<li>Increased intraocular pressure → optic nerve damage</li>
<li>"Silent thief of sight" — often no symptoms until late</li>
<li>Open angle most common; closed angle = acute emergency</li>
<li><b>Treatment:</b> Eye drops (beta-blockers), laser, surgery</li>
<li>Irreversible blindness if untreated — early detection crucial</li>
</ul>
<span class="sub sub-g">4. VITAMIN A DEFICIENCY / XEROPHTHALMIA</span>
<ul>
<li>Leading cause of <b>childhood blindness</b> in developing countries</li>
<li>Stages: Night blindness → Bitot's spots → Corneal xerosis → Keratomalacia (corneal melting) → Blindness</li>
<li><b>Treatment/Prevention:</b> Vitamin A supplementation</li>
<li>National programme: Vit A given at 9 months, 16 months, then every 6 months till 5 years</li>
<li>Now under control due to immunization programme distribution</li>
</ul>
<span class="sub sub-g">5. DIABETIC RETINOPATHY (Emerging Cause)</span>
<ul>
<li>Microangiopathy of retinal vessels due to diabetes</li>
<li>Globally 3 million moderate-severe visual impairment cases</li>
<li>Prevention: Good glycaemic control; annual retinal screening</li>
<li>Treatment: Laser photocoagulation, anti-VEGF injections, vitrectomy</li>
</ul>
<span class="sub sub-g">6. CORNEAL BLINDNESS</span>
<ul>
<li>Causes: trachoma, xerophthalmia, trauma, infections (HSV), ulcers</li>
<li>3–4 million persons blind due to corneal opacity</li>
<li>Treatment: Corneal transplantation (keratoplasty)</li>
<li>Prevention: Eye banking, eye donation awareness</li>
</ul>
</div>
</div>
<!-- TRACHOMA -->
<div class="card">
<div class="card-header teal">🦠 TRACHOMA — Infectious Cause of Blindness</div>
<div class="card-body">
<div class="box box-t">
<span class="title">DEFINITION (Park's)</span>
Chronic infectious disease of conjunctiva & cornea caused by <b>Chlamydia trachomatis</b>. Leads to conjunctival scarring → trichiasis/entropion → corneal ulceration → blindness.
</div>
<span class="sub sub-t">DISEASE PROCESS (How blindness occurs)</span>
<div class="box box-t" style="font-size:7.8px;">
Infection → Follicles on conjunctiva → <b>Scarring</b> → <b>Trichiasis</b> (inward eyelashes) / <b>Entropion</b> (inward lid) → Eyelashes scratch cornea → <b>Corneal ulcer → Scar → Blindness</b>
</div>
<span class="sub sub-t">DIAGNOSIS (Field criteria — need ≥2 of 4)</span>
<table class="th-t">
<thead><tr><th>#</th><th>Criterion</th></tr></thead>
<tbody>
<tr><td>a</td><td>Follicles on upper tarsal conjunctiva</td></tr>
<tr><td>b</td><td>Limbal follicles or Herbert's pits (their sequelae) ★</td></tr>
<tr><td>c</td><td>Typical conjunctival scarring (trichiasis, entropion)</td></tr>
<tr><td>d</td><td>Vascular pannus at superior limbus</td></tr>
</tbody>
</table>
<span class="sub sub-t">SAFE STRATEGY (WHO — Key for Exams!) ★</span>
<div class="box box-t">
<b>S</b> — Surgery (for trichiasis/entropion to prevent corneal damage)<br>
<b>A</b> — Antibiotics (tetracycline 1% ointment / oral azithromycin)<br>
<b>F</b> — Facial cleanliness (wash face, reduce fly contact)<br>
<b>E</b> — Environmental improvement (safe water, sanitation, hygiene)
</div>
<span class="sub sub-t">MAGNITUDE</span>
<ul>
<li>41 endemic countries affected</li>
<li>~1.9 million visual impairment; 1.2 million irreversibly blind</li>
<li>~190 million at risk of infection</li>
<li>Most affected: poor communities with poor water/sanitation</li>
</ul>
<span class="sub sub-t">CHEMOTHERAPY (Park's)</span>
<ul>
<li><b>Mass treatment</b>: if >5% severe/moderate trachoma in children <10 yr</li>
<li>Tetracycline 1% ointment twice daily × 5 days/month × 6 months</li>
<li>Alternatively: Azithromycin single oral dose (now preferred)</li>
<li><b>Selective treatment</b>: for low/medium prevalence areas — screen first, treat cases</li>
<li>Surgical correction of trichiasis/entropion: immediate impact on preventing blindness</li>
</ul>
</div>
</div>
</div>
<!-- ROW 3: PREVENTION + VISION 2020 + NPCB -->
<div class="three-col">
<!-- PREVENTION STRATEGIES -->
<div class="card">
<div class="card-header red">🛡️ PREVENTION OF BLINDNESS (Park's)</div>
<div class="card-body">
<div class="box box-r">
<b>"Avoidable blindness" = preventable + treatable</b><br>
About 80% of blindness is avoidable. Major opportunity for public health action!
</div>
<span class="sub sub-r">COMPONENTS OF NATIONAL PROGRAMME (Park's)</span>
<ol style="padding-left:12px; font-size:8px;">
<li style="margin-bottom:2px;"><b>Initial Assessment</b> — prevalence survey to identify causes & priorities</li>
<li style="margin-bottom:2px;"><b>Methods of Intervention:</b>
<ul>
<li>(a) Primary eye care — at PHC level</li>
<li>(b) Mass surgery campaigns — eye camps</li>
<li>(c) Treatment of individual patients</li>
<li>(d) Rehabilitation of the blind</li>
</ul>
</li>
<li style="margin-bottom:2px;"><b>Training of Personnel</b> — eye surgeons, assistants, PHC workers</li>
<li style="margin-bottom:2px;"><b>Health Education</b> — public awareness</li>
<li style="margin-bottom:2px;"><b>Evaluation</b> — monitoring outcomes</li>
</ol>
<span class="sub sub-r">LEVELS OF PREVENTION</span>
<table class="th-r">
<thead><tr><th>Level</th><th>Action</th></tr></thead>
<tbody>
<tr><td><b>Primordial</b></td><td>Reduce poverty, malnutrition, improve water/sanitation</td></tr>
<tr><td><b>Primary</b></td><td>Vit A supplementation, immunization, eye safety at work</td></tr>
<tr><td><b>Secondary</b></td><td>Early detection & treatment — screening camps, refraction</td></tr>
<tr><td><b>Tertiary</b></td><td>Surgery (cataract, glaucoma), corneal transplant, rehabilitation</td></tr>
</tbody>
</table>
</div>
</div>
<!-- VISION 2020 -->
<div class="card">
<div class="card-header amber">🎯 VISION 2020 & GLOBAL EYE HEALTH</div>
<div class="card-body">
<div class="box box-a">
<span class="title">VISION 2020: "The Right to Sight"</span>
Joint initiative of <b>WHO + IAPB (International Agency for Prevention of Blindness)</b><br>
Launched: <b>1999</b><br>
Goal: Eliminate avoidable blindness by the year <b>2020</b>
</div>
<span class="sub sub-a">5 PRIORITY DISEASES (Vision 2020)</span>
<ol style="padding-left:12px; font-size:8px;">
<li style="margin-bottom:2px;"><b>Cataract</b> — surgical intervention</li>
<li style="margin-bottom:2px;"><b>Refractive errors</b> — glasses, correction</li>
<li style="margin-bottom:2px;"><b>Trachoma</b> — SAFE strategy</li>
<li style="margin-bottom:2px;"><b>Onchocerciasis</b> (river blindness) — ivermectin</li>
<li style="margin-bottom:2px;"><b>Childhood blindness</b> — Vit A, Rubella vaccine, retinopathy care</li>
</ol>
<span class="sub sub-a">3 CORE STRATEGIES (Vision 2020)</span>
<div class="box box-a">
<b>1. Disease Control</b> — target priority diseases<br>
<b>2. Human Resource Development</b> — train eye care workers<br>
<b>3. Infrastructure Development</b> — equip facilities
</div>
<span class="sub sub-a">GLOBAL EYE HEALTH ACTION PLAN 2014–2019 (WHO)</span>
<ul>
<li>Target: 25% reduction in avoidable visual impairment by 2019 vs 2010 baseline</li>
<li>Universal eye health coverage goal</li>
<li>Integrate eye care into primary health care</li>
<li>National eye health plans for all countries</li>
</ul>
<span class="sub sub-a">CHANGING CONCEPTS IN EYE CARE (Park's)</span>
<ol style="padding-left:12px; font-size:8px;">
<li style="margin-bottom:1px;"><b>Primary eye care</b> at PHC level</li>
<li style="margin-bottom:1px;"><b>Epidemiological approach</b> — population surveys</li>
<li style="margin-bottom:1px;"><b>Team concept</b> — auxiliary workers (ophthalmic assistants)</li>
<li style="margin-bottom:1px;"><b>National programmes</b> — comprehensive, not disease-specific</li>
</ol>
</div>
</div>
<!-- NPCB + INDIA -->
<div class="card">
<div class="card-header purple">🇮🇳 INDIA — NPCB & KEY DATA</div>
<div class="card-body">
<div class="box box-p">
<span class="title">NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS (NPCB) — India</span>
Launched: <b>1976</b> (during 5th Five-Year Plan)<br>
Revised as: <b>NPCBVI</b> (National Programme for Control of Blindness and Visual Impairment) in 2017
</div>
<span class="sub sub-p">INDIA'S BLINDNESS BURDEN</span>
<ul>
<li>~<b>1.2 crore (12 million)</b> blind persons in India</li>
<li><b>Cataract: 62.6%</b> of blindness in India</li>
<li>Refractive error: ~19.7%</li>
<li>Corneal blindness: ~0.9%</li>
<li>Glaucoma: ~5.8%</li>
<li>Surgical backlog: India performs millions of cataract operations/year</li>
</ul>
<span class="sub sub-p">NPCB KEY ACTIVITIES</span>
<ul>
<li>Free cataract surgeries at district hospitals</li>
<li>Eye donation & eye bank strengthening</li>
<li>School eye screening programmes</li>
<li>District Mobile Ophthalmic Units</li>
<li>Training of ophthalmic assistants at PHC level</li>
<li>Vitamin A supplementation programme for children</li>
</ul>
<span class="sub sub-p">VITAMIN A SUPPLEMENTATION PROGRAMME</span>
<table class="th-r">
<thead><tr><th>Age</th><th>Dose</th></tr></thead>
<tbody>
<tr><td>9 months (with measles vaccine)</td><td>1 lakh IU (1,00,000 IU)</td></tr>
<tr><td>16 months</td><td>2 lakh IU (2,00,000 IU)</td></tr>
<tr><td>Every 6 months till 5 years</td><td>2 lakh IU (2,00,000 IU)</td></tr>
</tbody>
</table>
<span class="sub sub-p">WHO SET BLINDNESS THRESHOLD</span>
<div class="box box-r" style="font-size:7.8px;">
Blindness rate <b>>0.5%</b> of population = public health problem requiring urgent action (community with blinding trachoma)
</div>
</div>
</div>
</div>
<!-- MCQ BANK -->
<div style="margin-bottom:5px;">
<div class="mcq-banner">📝 HIGH-YIELD MCQs & VIVA QUESTIONS</div>
<div class="mcq-grid">
<div class="mcq-item">
<span class="mcq-q">Q. WHO definition of blindness?</span><br>
<span class="mcq-a">✔ VA < 3/60 (Snellen)</span><br>
Adopted at 25th WHA, 1972
</div>
<div class="mcq-item">
<span class="mcq-q">Q. #1 cause of blindness globally?</span><br>
<span class="mcq-a">✔ Un-operated Cataract (35%)</span><br>
#1 visual impairment = Refractive error (53%)
</div>
<div class="mcq-item">
<span class="mcq-q">Q. % of avoidable blindness?</span><br>
<span class="mcq-a">✔ About 80% is avoidable</span><br>
(preventable or treatable)
</div>
<div class="mcq-item">
<span class="mcq-q">Q. SAFE strategy is for?</span><br>
<span class="mcq-a">✔ Trachoma control</span><br>
S-Surgery A-Antibiotics F-Face E-Environment
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Vision 2020 launched by?</span><br>
<span class="mcq-a">✔ WHO + IAPB, in 1999</span><br>
Goal: eliminate avoidable blindness by 2020
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Cause of trachoma?</span><br>
<span class="mcq-a">✔ Chlamydia trachomatis</span><br>
Chronic conjunctival & corneal disease
</div>
<div class="mcq-item">
<span class="mcq-q">Q. NPCB launched in India?</span><br>
<span class="mcq-a">✔ 1976 (5th Five Year Plan)</span><br>
Now NPCBVI (2017)
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Leading cause of childhood blindness?</span><br>
<span class="mcq-a">✔ Xerophthalmia (Vit A deficiency)</span><br>
Also: congenital cataract, glaucoma
</div>
<div class="mcq-item">
<span class="mcq-q">Q. Herbert's pits are seen in?</span><br>
<span class="mcq-a">✔ Trachoma (healed limbal follicles)</span><br>
Pathognomonic of old trachoma!
</div>
</div>
</div>
<!-- EXAM TIPS -->
<div style="margin-bottom:5px;">
<div class="tips-banner">🌟 LINES TO IMPRESS THE EXAMINER</div>
<div class="tips-grid">
<div class="tip-item">
✔ <b>"The #1 cause of blindness is cataract (35%) but the #1 cause of visual impairment is uncorrected refractive error (53%) — these are different, and this distinction is very commonly asked."</b>
</div>
<div class="tip-item">
✔ <b>"About 80% of all blindness is avoidable — either preventable or treatable. Cataract alone causes 35% of blindness but is completely curable with a simple surgical procedure."</b>
</div>
<div class="tip-item">
✔ <b>"Trachoma is controlled by the WHO SAFE strategy: Surgery for trichiasis, Antibiotics (azithromycin/tetracycline), Facial cleanliness, and Environmental improvement."</b>
</div>
<div class="tip-item">
✔ <b>"Vision 2020 — The Right to Sight was launched in 1999 by WHO and IAPB with the goal to eliminate avoidable blindness by 2020, focusing on 5 priority diseases: cataract, refractive errors, trachoma, onchocerciasis, and childhood blindness."</b>
</div>
<div class="tip-item">
✔ <b>"The WHO definition of blindness is visual acuity less than 3/60. Before 1972, there were 65 different definitions of blindness worldwide — the 25th World Health Assembly standardized this."</b>
</div>
<div class="tip-item">
✔ <b>"In India, cataract accounts for 62.6% of blindness. The NPCB was launched in 1976 during the 5th Five Year Plan to address this through free cataract surgeries, school screening, and Vitamin A supplementation."</b>
</div>
</div>
</div>
<div class="footer">
PSM Quick Reference — Blindness | MBBS 2nd Year | Source: Park's Textbook of PSM | WHO ICD-11 2018 | Vision 2020 | NPCB India | Generated by Orris — Good luck on your exam! 🎓
</div>
</body>
</html>
libreoffice --headless --convert-to pdf --outdir /tmp/ /home/daytona/workspace/blindness/blindness_cheatsheet.html 2>&1 && cp /tmp/blindness_cheatsheet.pdf /home/daytona/workspace/blindness/Blindness_PSM_Cheatsheet.pdf && python3 -c "from pypdf import PdfReader; r=PdfReader('/home/daytona/workspace/blindness/Blindness_PSM_Cheatsheet.pdf'); print(f'Pages: {len(r.pages)}')" && ls -lh /home/daytona/workspace/blindness/Blindness_PSM_Cheatsheet.pdf
BLINDNESS — Complete PSM Guide (K. Park)
1. Definition of Blindness (Park's — Most Asked!)
Before 1972, there were 65 different definitions of blindness worldwide. The 25th World Health Assembly (1972) standardized it.
"Visual acuity of less than 3/60 (Snellen) or its equivalent"
ICD-11 (2018) Classification — Distance Vision:
| Category | Visual Acuity | Simple way to remember |
|---|---|---|
| Mild impairment | Worse than 6/12 | Can't read fine print |
| Moderate impairment | Worse than 6/18 | Low vision |
| Severe impairment | Worse than 6/60 | Finger counting |
| BLINDNESS ★ | Worse than 3/60 | Light perception only |
Old terms (still asked):
- Economic blindness = VA < 6/60 (cannot earn a living)
- Social blindness = VA < 3/60 (needs social support)
- Total blindness = No light perception at all
2. Magnitude of the Problem (Park's)
- 82% of visually impaired are aged ≥50 years
- 19 million children are visually impaired; 1.4 million irreversibly blind
~80% of all blindness is AVOIDABLE (preventable or treatable) Only 20% is unavoidable (congenital, hereditary)
3. Causes of Blindness — The Most Tested Table (Park's)
Global Causes of BLINDNESS:
| Rank | Cause | % |
|---|---|---|
| 1 | Un-operated Cataract ★ | 35% |
| 2 | Uncorrected Refractive Error | 21% |
| 3 | Glaucoma | 8% |
| 4 | Age-related Macular Degeneration | ~5% |
| 5 | Corneal Opacities | ~4% |
| 6 | Diabetic Retinopathy | ~3% |
| 7 | Trachoma | ~2% |
Global Causes of MODERATE-SEVERE VISUAL IMPAIRMENT:
| Rank | Cause | % |
|---|---|---|
| 1 | Uncorrected Refractive Errors ★ | 53% |
| 2 | Un-operated Cataract | 25% |
| 3 | Age-related Macular Degeneration | 4% |
| 4 | Glaucoma | 2% |
| 5 | Diabetic Retinopathy | 1% |
- #1 cause of BLINDNESS = Cataract (35%)
- #1 cause of VISUAL IMPAIRMENT = Refractive Error (53%)
- These are different — don't confuse them!
India / South-East Asia (SEAR):
- Cataract = 50–80% of all blindness in SEAR
- In India: Cataract = 62.6% of blindness
- ~1.2 crore (12 million) blind persons in India
- Childhood blindness = Xerophthalmia (Vitamin A deficiency) — now declining
4. Causes in Detail
Cataract (Most Important):
- Opacity of the lens — gradual, painless vision loss
- Types: Senile (most common), congenital, traumatic, diabetic
- Treatment: Surgery (ECCE + IOL implant) — complete cure possible
- Fully preventable blindness — just needs access to surgery
Vitamin A Deficiency / Xerophthalmia:
Night blindness → Bitot's spots → Corneal xerosis → Keratomalacia → Corneal scar → BLINDNESS
- Prevention: Vitamin A supplementation programme:
- 9 months: 1 lakh (1,00,000) IU with measles vaccine
- 16 months: 2 lakh (2,00,000) IU
- Every 6 months till age 5: 2 lakh IU
Glaucoma:
- "Silent thief of sight" — progressive optic nerve damage from high intraocular pressure
- Often asymptomatic until late stage → irreversible blindness if missed
- Treatment: Eye drops (timolol), laser, surgery
Trachoma:
- Agent: Chlamydia trachomatis
- Leads to: follicles → scarring → trichiasis (inward eyelashes) → corneal ulcer → blindness
- Controlled by SAFE strategy (see below)
5. Trachoma — SAFE Strategy ⭐ (Most Exam-Favourite Topic)
- Follicles on upper tarsal conjunctiva
- Limbal follicles / Herbert's pits (pathognomonic of old trachoma)
- Conjunctival scarring (trichiasis, entropion)
- Vascular pannus at superior limbus
WHO SAFE Strategy:
| Letter | Meaning | Action |
|---|---|---|
| S | Surgery | Correct trichiasis/entropion to prevent corneal damage |
| A | Antibiotics | Tetracycline 1% ointment / oral Azithromycin single dose |
| F | Facial cleanliness | Wash face, reduce fly contact |
| E | Environmental improvement | Safe water, sanitation, hygiene |
6. Vision 2020 — "The Right to Sight" ⭐
- Launched: 1999 by WHO + IAPB (International Agency for Prevention of Blindness)
- Goal: Eliminate avoidable blindness by 2020
5 Priority Diseases (Vision 2020):
- Cataract — surgical intervention
- Refractive errors — spectacles, correction
- Trachoma — SAFE strategy
- Onchocerciasis (river blindness) — ivermectin
- Childhood blindness — Vitamin A, rubella vaccine
3 Core Strategies:
- Disease Control — target priority diseases
- Human Resource Development — train eye care workers
- Infrastructure Development — equip facilities
7. Prevention of Blindness — Components of National Programme (Park's)
- Initial Assessment — prevalence surveys to identify causes and priorities
- Methods of Intervention:
- (a) Primary eye care — at PHC level (most important concept!)
- (b) Mass surgery campaigns — eye camps
- (c) Treatment of individual patients
- (d) Rehabilitation of the blind
- Training of Personnel — ophthalmic assistants, PHC workers
- Health Education — community awareness
- Evaluation — monitoring and assessment
Levels of Prevention:
| Level | Action |
|---|---|
| Primordial | Reduce poverty, improve water/sanitation |
| Primary | Vit A supplementation, immunization, eye safety |
| Secondary | Screening camps, early detection, refraction |
| Tertiary | Surgery, corneal transplant, rehabilitation |
8. NPCB — India's National Programme
- NPCB (National Programme for Control of Blindness) — launched 1976 (5th Five Year Plan)
- Renamed NPCBVI (+ Visual Impairment) in 2017
- Free cataract surgeries at district hospitals
- Eye donation and eye bank strengthening
- School eye screening programme
- District Mobile Ophthalmic Units
- Training of ophthalmic assistants at PHC level
Lines to Impress the Examiner 🌟
- "The #1 cause of blindness is cataract (35%) but the #1 cause of visual impairment is uncorrected refractive error (53%) — these are two different answers for two different questions."
- "About 80% of all blindness is avoidable — either preventable or treatable. This is the most important public health message about blindness."
- "Trachoma is controlled by the WHO SAFE strategy — Surgery, Antibiotics, Facial cleanliness, and Environmental improvement."
- "Vision 2020 — The Right to Sight was launched in 1999 by WHO and IAPB, focusing on 5 priority diseases including cataract, trachoma, and childhood blindness."
- "Before 1972, there were 65 different definitions of blindness worldwide. The 25th World Health Assembly standardized it as visual acuity less than 3/60."
- "In India, cataract accounts for 62.6% of blindness. NPCB was launched in 1976 to address this through free surgeries and the Vitamin A supplementation programme."
Blindness PSM Cheatsheet
PDF Document · PDF
blindness cheatsheet
HTML File · HTML
| Section | Content |
|---|---|
| Definition & classification | WHO definition, ICD-11 table, old terms, avoidable blindness |
| Magnitude | Global causes of blindness table, visual impairment table, India data |
| Major causes in detail | Cataract, refractive error, glaucoma, Vit A, diabetic retinopathy, corneal blindness |
| Trachoma | SAFE strategy, diagnosis criteria, chemotherapy protocol |
| Prevention | National programme components, levels of prevention |
| Vision 2020 | Launch year, IAPB, 5 priority diseases, 3 strategies |
| NPCB India | 1976 launch, key activities, Vit A schedule |
| 9 MCQs | With answers covering all high-yield topics |
| 6 Examiner tips | Exact sentences to say to impress |
I am new 3rd year students and i have obstretics and gynecology posting tommorow and i dont know aything about taking history in this ward . please help me how to take histroy and how to present so that my professor will impress\