Diagnostic criteria for ckd
Reading File
Finding Sources
Searching PubMed
"chronic kidney disease" AND "diagnostic criteria" AND KDIGO
Finding Sources
Searching PubMed
"chronic kidney disease" AND "GFR" AND classification
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a complete, textbook-grounded summary of the diagnostic criteria for CKD.
Diagnostic Criteria for Chronic Kidney Disease (CKD)
Core Definition (KDIGO 2012)
CKD is defined as any of the following abnormalities present for more than 3 months. Either criterion alone is sufficient - both do not need to be present simultaneously.
Criterion 1 - Markers of Kidney Damage (one or more)
| Marker | Detail |
|---|---|
| Albuminuria | Albumin excretion rate ≥30 mg/24 hr; OR albumin-to-creatinine ratio (ACR) ≥30 mg/g (albuminuria stages A2-A3) |
| Urine sediment abnormalities | Dysmorphic RBCs (suggest glomerular disease), RBC casts (proliferative GN), WBC casts (pyelonephritis/tubulointerstitial nephritis), oval fat bodies |
| Imaging abnormalities | Small kidneys, cortical scarring, hydronephrosis, polycystic kidneys, structural anomalies on ultrasound/CT/MRI |
| Electrolyte/tubular disorders | Abnormal serum/urine electrolytes, urine pH, glucosuria without hyperglycemia, aminoaciduria, or low-molecular-weight proteinuria |
| Pathologic abnormalities | Biopsy-confirmed kidney damage |
| History of kidney transplantation | Regardless of current GFR |
Criterion 2 - Decreased GFR
- eGFR < 60 mL/min/1.73 m² (GFR stages G3a-G5)
Note: GFR 60-89 (G2) alone, without any marker of kidney damage, does NOT meet CKD criteria. Damage must be documented first for G1/G2 to count.
The 3-Month Chronicity Requirement
Duration >3 months distinguishes CKD from acute kidney injury (AKI). This can be:
- Documented - review of serial labs or records
- Inferred - chronic illness history, small kidneys on imaging, absence of acute oliguria
CKD Staging - "CGA" Classification (KDIGO)
CKD is classified by Cause + GFR category (G) + Albuminuria category (A):
GFR Categories (G)
| Stage | GFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal or high (requires damage marker) |
| G2 | 60-89 | Mildly decreased (requires damage marker) |
| G3a | 45-59 | Mildly to moderately decreased |
| G3b | 30-44 | Moderately to severely decreased |
| G4 | 15-29 | Severely decreased |
| G5 | <15 | Kidney failure (ESKD if on dialysis/transplant) |
Albuminuria Categories (A)
| Category | ACR | Description |
|---|---|---|
| A1 | <30 mg/g | Normal to mildly increased |
| A2 | 30-300 mg/g | Moderately increased (formerly "microalbuminuria") |
| A3 | >300 mg/g | Severely increased (includes nephrotic-range) |
KDIGO Risk Stratification (GFR x Albuminuria grid)
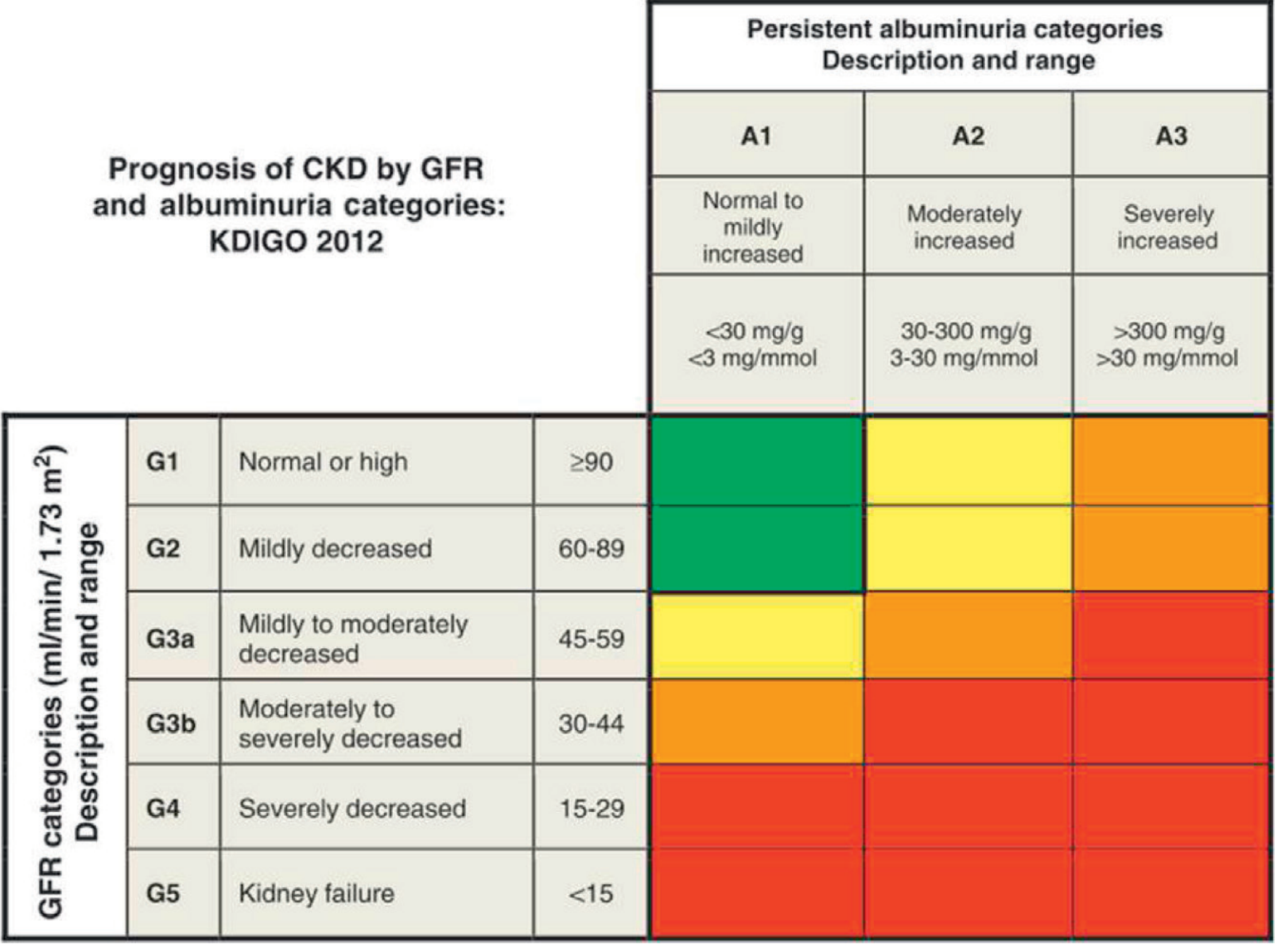
The color-coded grid above shows risk of CKD progression: green = low risk, yellow = moderately increased, orange = high, red = very high.
GFR Estimation
- CKD-EPI creatinine equation is the currently preferred method (more accurate than MDRD at higher GFR values)
- Cystatin C-based or combined creatinine-cystatin C equations can be used for confirmation, especially when creatinine-based estimates may be unreliable (high muscle mass, low meat intake, certain medications like trimethoprim or fenofibrate that block tubular secretion of creatinine)
- The Cockcroft-Gault equation estimates creatinine clearance (not GFR) but is still used for drug dosing
Key Points to Remember
- CKD in G1/G2 requires a damage marker - low GFR alone is not enough at these stages
- CKD in G3a-G5 can be diagnosed on GFR alone, even without an identified damage marker
- Albuminuria is both a diagnostic marker and an independent prognostic factor - higher albuminuria at any GFR stage worsens prognosis
- Always classify by cause (diabetic, non-diabetic glomerular, vascular, tubulointerstitial, cystic/congenital, transplant)
- ESKD = a subset of G5 requiring kidney replacement therapy (dialysis or transplant)
Sources: Goldman-Cecil Medicine (Table 116-4, Table 116-5); Brenner & Rector's The Kidney (Fig. 19.2, CGA staging); Textbook of Family Medicine 9e (Table 40-10) - all referencing KDIGO 2012 Clinical Practice Guideline, Kidney Int Suppl. 2013;3:1-150.
This is a shared conversation. Sign in to Orris to start your own chat.