Leprosy
Reading File
Finding Sources
Searching PubMed
leprosy Hansen disease
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough response. Here is a comprehensive overview of leprosy.
Leprosy (Hansen Disease)
Etiology & Epidemiology
Leprosy is a chronic infectious disease caused most often by Mycobacterium leprae and, less frequently, by M. lepromatosis (proposed name since 2008). Despite low communicability, it remains endemic with approximately 200,000 new infections per year, concentrated in Southeast Asia, East Africa, and Brazil. India alone accounts for ~78% of cases worldwide. In the United States, 100-200 cases occur annually, predominantly in immigrants and in a few southern states (Louisiana, Arkansas, Texas, Mississippi).
The Organism
M. leprae is a weakly acid-fast, obligate intracellular pathogen that:
- Cannot be cultured in vitro
- Proliferates best at 32-34°C (human skin temperature) - explaining why the CNS and visceral organs are spared
- Secretes no toxins; virulence is based on cell wall properties, particularly lipid PGL-1, which is critical for host cell invasion
- Inhibits mitochondrial energy metabolism to evade immune responses
- Is sufficiently similar to M. tuberculosis that BCG vaccination confers partial protection
Transmission: Primarily via nasal secretions with close, prolonged contact (years). Zoonotic transmission from armadillos occurs rarely.
Spectrum of Disease: The Ridley-Jopling Classification
The disease spans a tuberculoid-to-lepromatous spectrum determined entirely by the host's T-lymphocyte response:
| Feature | Tuberculoid (TT) | Borderline (BT/BB/BL) | Lepromatous (LL) |
|---|---|---|---|
| Immune response | Strong Th1 + Th17 | Mixed | Weak Th1; Th2/Treg dominant |
| Bacterial load | Paucibacillary | Variable | Multibacillary |
| Skin lesions | Few, well-defined, anaesthetic | Intermediate | Numerous, symmetric |
| Nerve involvement | Asymmetric, early | Variable | Symmetric, late |
| Lepromin test | Positive | Variable | Negative |
| Antibody production | Low | Variable | High (but non-protective) |
WHO field classification simplifies this into two groups:
- Paucibacillary (PB): up to 5 skin lesions, no organisms on smear
- Multibacillary (MB): 6 or more lesions, smear-positive
Immunopathogenesis
- Tuberculoid leprosy: Classically activated (M1) macrophages with a Th1/Th17 response, producing IL-2 and IFN-γ. IFN-γ mobilizes effective macrophage killing, so bacillary burden is low. This mirrors the immune response in tuberculosis.
- Lepromatous leprosy: Weak Th1 response; relative increase in regulatory T cells and Th2 activity. LILRA2 expression is increased in lesions, blocking TLR-directed antimicrobial activity, reducing IL-12 production, and enhancing immunosuppressive IL-10 by monocytes. The result is an inability to control bacterial replication.
- Immune complex disease: In lepromatous leprosy, antibodies against M. leprae antigens form immune complexes that can cause erythema nodosum leprosum (ENL), vasculitis, and glomerulonephritis.
Clinical Features
Tuberculoid Leprosy
- Flat, red skin lesions that enlarge with indurated, elevated, hyperpigmented margins and depressed pale centers (central healing)
- "Leprids" - anaesthetic, hypopigmented, or erythematous macules with elevated edges, dry/rough surface
- Asymmetric peripheral nerve involvement - nerves become palpably thickened and tender
- Nerve destruction causes skin anesthesia, muscle atrophy, chronic ulcers, contractures, and potentially autoamputation
Lepromatous Leprosy
- Symmetric widespread disease involving skin, peripheral nerves, anterior eye, upper airways (to larynx), testes, hands, feet
- Pale macules → plaques → nodules ("lepromas")
- Leonine facies: nodular coalescing lesions of the face
- Nasal bridge collapse and upward lifting of the nasal tip due to destruction of lateral cartilages and septum
- Loss of eyebrows (madarosis)
- Claw hand: from ulnar nerve involvement at elbow + median nerve at wrist
- Foot drop: lateral popliteal nerve involvement (nerve palpably thickened behind upper fibula)
- Clawing of toes: posterior tibial nerve involvement
- Trophic ulceration of feet from anesthesia
- Ocular complications: facial nerve palsy → lagophthalmos → exposure keratitis; iridocyclitis; blindness
- Testicular atrophy → gynecomastia and sterility
- In advanced disease, bacilli present in sputum and blood
Histopathology
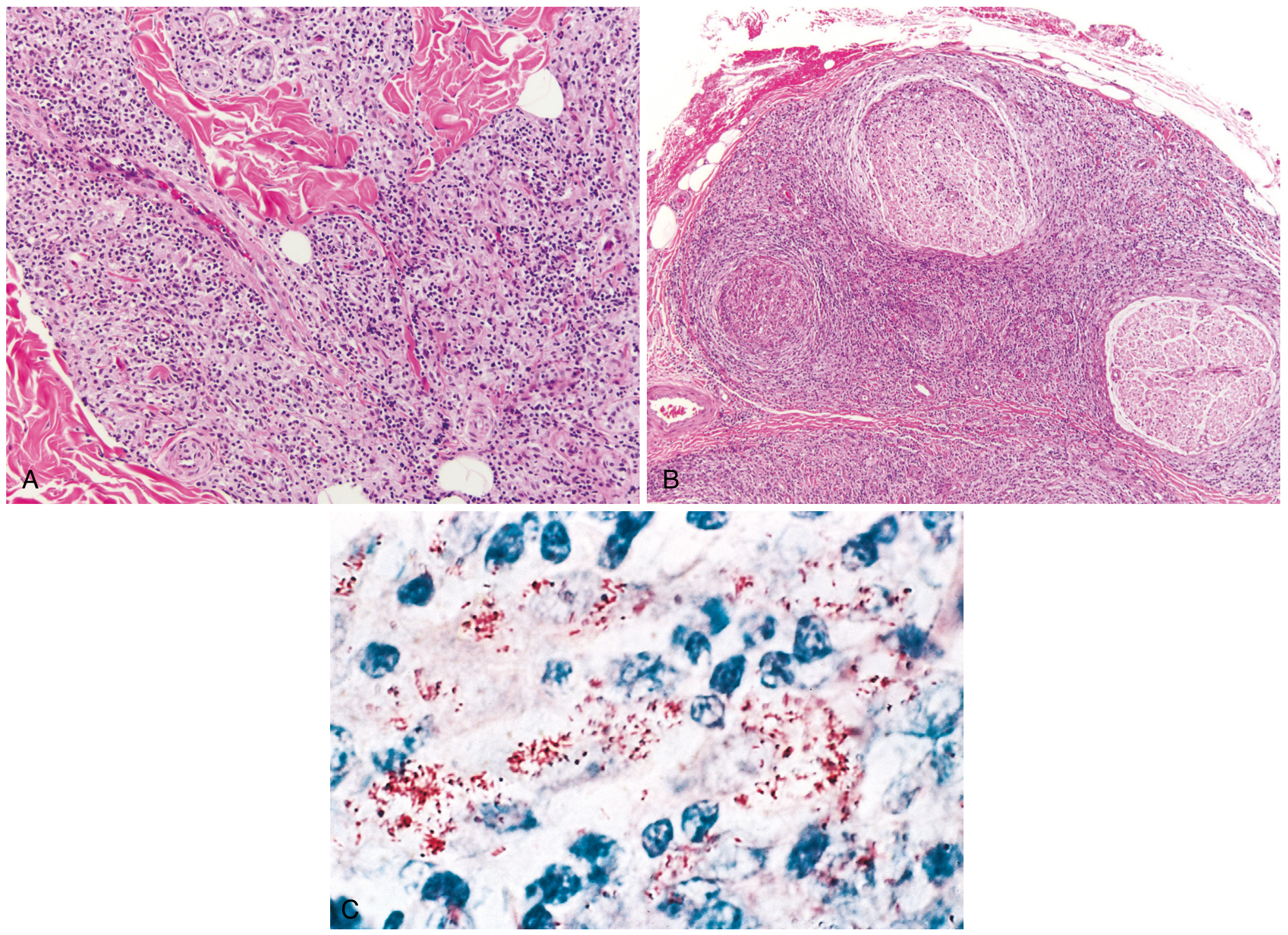
Fig. 8.33 from Robbins Pathologic Basis of Disease - Leprosy histology. (A) Dense dermal macrophage infiltration surrounding adnexa, vessels, and nerves in tuberculoid leprosy. (B) Dense chronic lymphocytic and macrophage infiltration into large nerve bundles in lepromatous leprosy. (C) Acid-fast bacilli (red) within macrophages in the lepromatous form.
- Tuberculoid: Non-caseating epithelioid granulomas resembling TB, giant cells, numerous lymphocytes. Bacilli virtually absent (paucibacillary). Reflects strong T-cell immunity.
- Lepromatous: Large aggregates of lipid-laden macrophages ("lepra cells") filled with masses ("globi") of acid-fast bacilli. Lymph nodes show foamy macrophages in paracortical (T-cell) areas. Testes extensively involved with destruction of seminiferous tubules.
Diagnosis
- Skin smear (slit-skin smear): acid-fast staining to detect bacilli
- Skin biopsy: histology showing granulomas (tuberculoid) or lepra cells/AFB (lepromatous)
- Lepromin (Mitsuda) test: intradermal injection of killed bacilli - positive in tuberculoid, negative in lepromatous
- Clinical diagnosis: the anaesthetic skin patch is the hallmark of tuberculoid leprosy; palpably thickened peripheral nerves are characteristic
- M. leprae cannot be cultured on artificial media - this remains a diagnostic challenge
Lepra Reactions (Immune-Mediated)
Two types of acute inflammatory episodes can occur during or after treatment:
Type 1 (Reversal Reaction):
- Due to sudden increase in cell-mediated immunity
- Occurs in borderline types (BT, BB, BL)
- Skin lesions become red, swollen, painful; acute neuritis with risk of sudden nerve damage
- Treatment: NSAIDs for mild cases; prednisolone 0.5-1 mg/kg/day for 20 weeks for moderate-severe; splinting/rest for affected nerves; surgical nerve decompression if persistent
Type 2 (Erythema Nodosum Leprosum - ENL):
- Immune complex-mediated (deposited in skin and vessels)
- Occurs in BL and LL types
- Tender erythematous nodules, fever, malaise, uveitis, neuritis, orchitis
- Treatment: NSAIDs/analgesics for mild cases; prednisolone ≤1 mg/kg/day for severe cases; thalidomide is highly effective for recurrent/chronic ENL; clofazimine 300 mg/day for steroid-dependent cases
WHO Multidrug Therapy (MDT)
MDT using rifampicin + dapsone + clofazimine has been the standard of care since 1982 and is highly successful for curing all forms of leprosy. MDT is distributed in monthly blister packs.
| Multibacillary | Paucibacillary | |
|---|---|---|
| Duration | 12 months | 6 months |
Adult dosing (WHO 2018 guidelines):
- Rifampicin: 600 mg once monthly
- Clofazimine: 300 mg once monthly + 50 mg daily
- Dapsone: 100 mg daily
Pediatric dosing (10-14 yr):
- Rifampicin 450 mg/month; Clofazimine 150 mg/month + 50 mg on alternate days; Dapsone 50 mg daily
Key Drug Side Effects
| Drug | Major Side Effects |
|---|---|
| Rifampicin | Red/orange body fluids, hepatitis, flu-like syndrome, enzyme inducer (reduces efficacy of oral contraceptives), thrombocytopenia |
| Clofazimine | Orange-brown skin/mucosa discoloration (reversible), crystal enteropathy at high doses, splenic infarction, cardiac arrhythmia |
| Dapsone | Hemolytic anemia (significant in G6PD deficiency), methemoglobinemia; dapsone hypersensitivity syndrome (fever, rash, lymphadenopathy, hepatitis - can be fatal) |
Drug Resistance
Rifampicin-resistant cases are treated with second-line drugs: clarithromycin 500 mg/day, minocycline 100 mg/day, or a quinolone (ofloxacin 400 mg/day, levofloxacin 500 mg/day, or moxifloxacin 400 mg/day) + clofazimine 50 mg/day for 6 months, followed by clofazimine + one second-line drug for a further 18 months.
Prognosis & Social Impact
- Most patients die with leprosy rather than of it, given the extremely slow course spanning decades
- Self-healing has been documented (see PubMed: PMID 39264863, systematic review 2024) but is uncommon
- Deformities are largely preventable with early diagnosis and MDT
- Persistent stigma remains a major public health challenge; the term "leper" is considered derogatory and should not be used
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine (International Ed.); Bailey and Love's Short Practice of Surgery (28th Ed.); Roitt's Essential Immunology; Textbook of Family Medicine (9th Ed.)
Recent evidence note: A 2024 systematic review on leprosy immunopathogenesis (PMID 39308868) is available in Frontiers in Immunology which may provide updated insight on immune mechanisms beyond what is covered in the textbooks above.
This is a shared conversation. Sign in to Orris to start your own chat.