Tracheo oesophageal fistula in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
tracheoesophageal fistula acquired management
Searching the Web
tracheoesophageal fistula RGUHS ENT 50 marks classification management recent advances
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading Article
PMID: 40892023
TRACHEO-OESOPHAGEAL FISTULA (TOF)
50-Mark Answer | RGUHS Examination Standard
1. DEFINITION
A Tracheo-Oesophageal Fistula (TOF) is an abnormal communication between the trachea and the oesophagus. It may be congenital (arising from failure of embryological separation) or acquired (resulting from pressure necrosis, malignancy, infection, or trauma).
- Scott Brown's Otorhinolaryngology, Vol. 2, p. 557
- Cummings Otolaryngology, p. block46
2. EMBRYOLOGY
The trachea and oesophagus develop from the primitive foregut. The laryngotracheal groove appears in the ventral wall of the pharynx at approximately week 4 of gestation. The lateral mesodermal tracheo-oesophageal ridges grow medially and fuse to separate the ventral respiratory tract from the dorsal alimentary tract.
Failure of this separation at any level results in TOF. The embryologic origin of isolated TOF is similar to that of laryngotracheal clefts; for combined oesophageal atresia (OA) + TOF, the mechanism is less well understood.
- Scott Brown's, Vol. 2, p. 557 - "If the separation of the developing oesophagus and trachea by the lateral mesodermal ridges fails, the result is an isolated TOF"
EMBRYOLOGICAL DEVELOPMENT FLOWCHART
─────────────────────────────────────────────────────────
Primitive Foregut (Week 4)
│
▼
Laryngotracheal Groove (ventral wall of pharynx)
│
▼
Lateral Mesodermal Tracheo-Oesophageal Ridges form
│
┌───┴───┐
Normal FAILURE
Fusion of Fusion
│ │
▼ ▼
Trachea & Tracheo-Oesophageal
Oesophagus Fistula (TOF)
separated ± Oesophageal Atresia
─────────────────────────────────────────────────────────
3. INCIDENCE AND EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Incidence | 1 in 2,500 to 1 in 5,000 live births |
| Sex ratio | Slight male preponderance |
| Associated anomalies | Up to 50% of cases |
| Most common associated anomaly | Cardiovascular (25-30%) |
| Prematurity | Common |
- Cummings Otolaryngology, p. block46 - "EA with or without TEF is the most common congenital anomaly of the esophagus (1 in 3500)"
- Scott Brown's, Vol. 2, p. 557 - "thought to affect between 1 in 2000 and 1 in 5000 live births"
4. CLASSIFICATION
A. Gross / Vogt Classification (Most Commonly Used in RGUHS/Indian Exams)
This is the standard classification used by Dhingra, Hazarika, and Zakir Hussain. The Gross classification (1953) has five types:
GROSS CLASSIFICATION OF OA AND TOF
─────────────────────────────────────────────────────────────────────
TYPE DESCRIPTION INCIDENCE
─────────────────────────────────────────────────────────────────────
A Pure oesophageal atresia (no fistula) 8%
[Upper blind pouch + lower blind pouch]
B OA + proximal TOF 2%
[Upper pouch connects to trachea]
C OA + distal TOF (MOST COMMON) 85-87%
[Upper blind pouch + lower oesophagus
connects to trachea/carina]
D OA + proximal and distal TOF < 1%
[Both pouches connect to trachea]
E H-type / N-type TOF (no atresia) 4%
[Fistula only, oesophagus intact]
─────────────────────────────────────────────────────────────────────
The diagram below from Scott Brown's shows the five types:
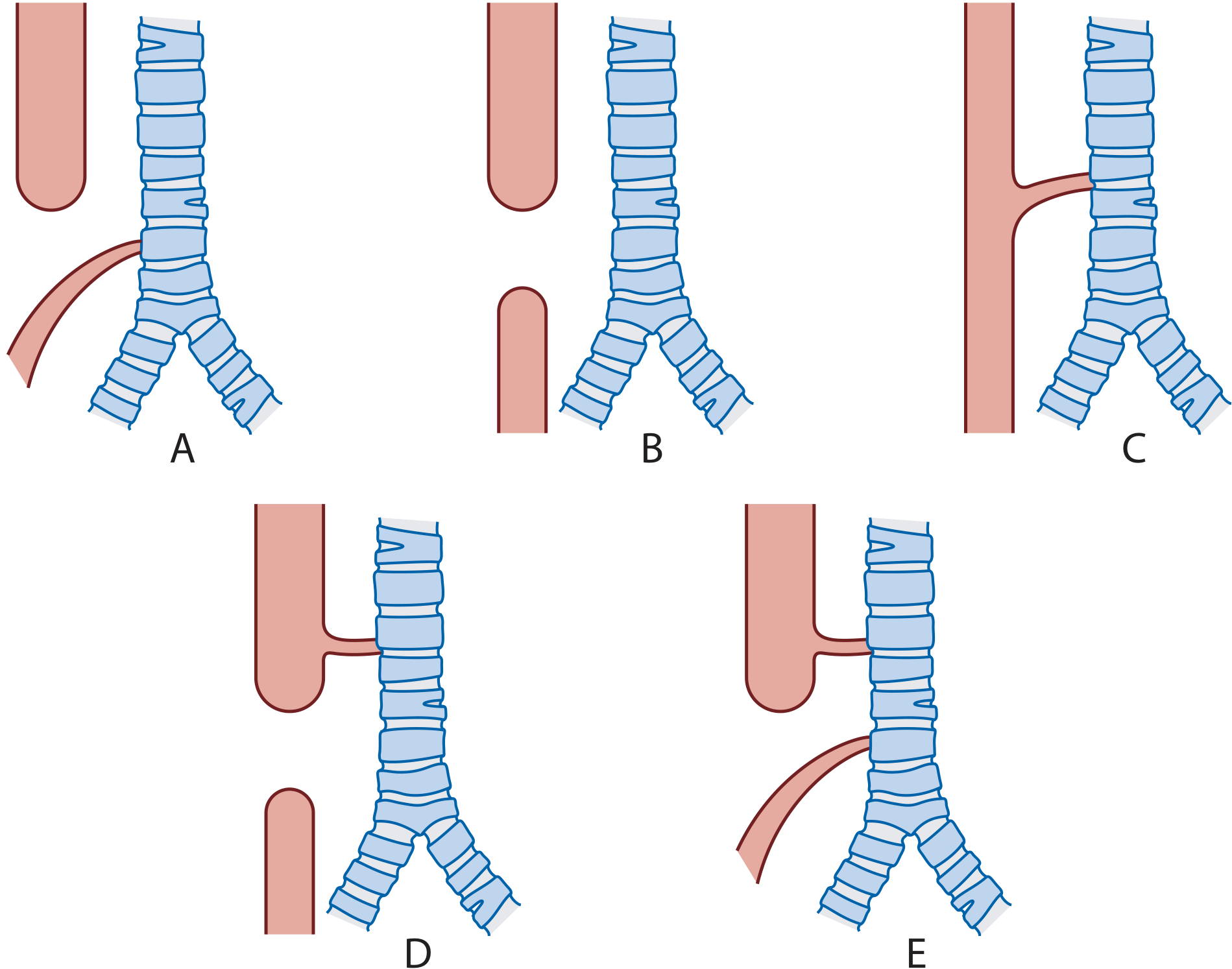
Figure: Types and incidences of oesophageal atresia with or without a tracheo-oesophageal fistula.
- Type A (OA with distal TOF): 85%
- Type B (Isolated OA): 8%
- Type C (Isolated H/N type TOF): 4%
- Type D (OA with proximal TOF): 2%
- Type E (OA with proximal and distal TOF): <1%
(Note: Scott Brown's labels A-E differently from Gross; in Indian textbooks Dhingra/Hazarika use Gross Type I-V or A-E)
- Scott Brown's, Vol. 2, p. 557
- K. J. Lee's Essential Otolaryngology, p. 693
B. Classification by Aetiology (Acquired TOF)
- Benign - Iatrogenic, Infectious, Traumatic
- Malignant - Oesophageal carcinoma (most common), bronchogenic carcinoma, thyroid carcinoma, mediastinal lymphoma
- Current Surgical Therapy (cited in Cummings), p. 1025
5. AETIOLOGY
A. Congenital
- Failure of embryological separation of foregut
- Associated with VACTERL association (Vertebral, Anorectal, Cardiac, TrachEo-Esophageal, Renal, Limb defects)
- Associated with CHARGE syndrome (Coloboma, Heart defects, Atresia choanae, Retardation of growth, Genital/urinary abnormalities, Ear abnormalities)
B. Acquired
AETIOLOGY OF ACQUIRED TOF
──────────────────────────────────────────────────────
ACQUIRED TOF
┌────────┴────────┐
BENIGN MALIGNANT
│ │
┌──────┼──────┐ ┌──────┼──────────┐
│ │ │ │ │ │
Iatro- Infec- Trau- Oeso- Broncho- Thyroid/
genic tious matic phageal genic Lymphoma
Ca Ca
│ │
ETT TB/
cuff Histoplas-
+NGT mosis
──────────────────────────────────────────────────────
Iatrogenic (most common benign cause):
- Prolonged mechanical ventilation: ETT cuff + NG tube cause pressure necrosis at the posterior membranous tracheal wall and anterior oesophagus
- Tracheostomy complications (occurs in <1% of tracheotomy patients)
- Post-surgical anastomotic leak
- Stenting erosion
Infectious:
- Tuberculosis (most common in India)
- Histoplasmosis
- Actinomycosis
Traumatic:
-
Foreign body impaction and erosion
-
Caustic ingestion
-
Penetrating/blunt trauma to neck
-
Cummings, p. block2 - "TEF occurs in less than 1% of patients who undergo tracheotomy. The risk of fistula formation through the 'party wall' is increased when a large-bore nasogastric tube is also in place."
-
Current Surgical Therapy, p. 1025
6. PATHOPHYSIOLOGY
PATHOPHYSIOLOGY OF CONGENITAL TOF (Type C - Gross)
──────────────────────────────────────────────────────────────
Distal oesophagus connected to trachea/carina via fistula
│
▼
Swallowed contents pass
into tracheobronchial tree
│
┌────┴────┐
│ │
ASPIRATION GASTRIC ACID
PNEUMONIA REFLUX into
trachea
│ │
└────┬────┘
▼
Recurrent respiratory
infections / pneumonitis
──────────────────────────────────────────────────────────────
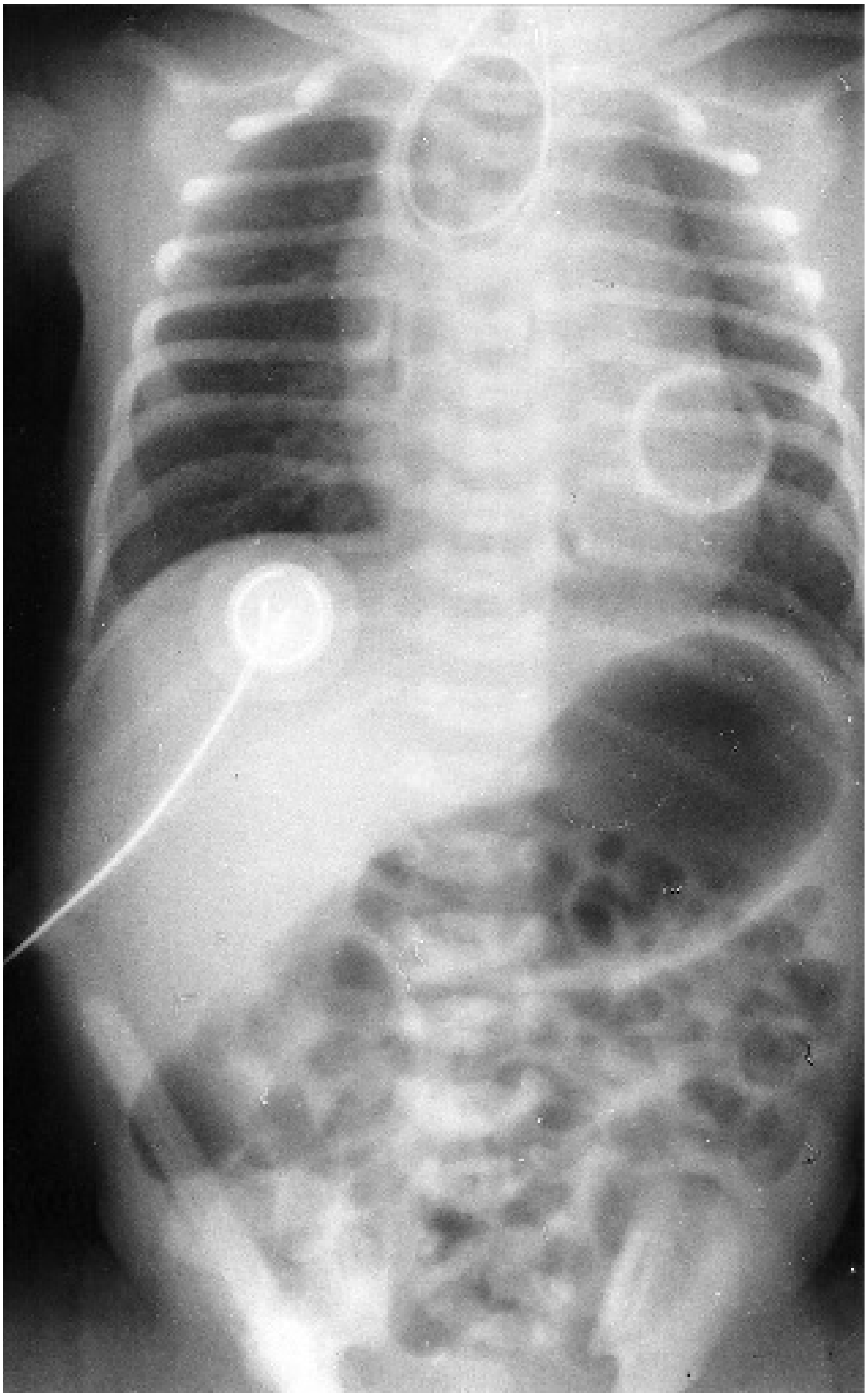
For Type A (Pure OA without fistula):
- Proximal blind pouch fills with saliva → overflow aspiration
- No gas in abdomen (differentiates from Type C on plain X-ray)
For H-type (Type E):
- Small amounts of fluid pass through fistula on swallowing
- Produces recurrent minor aspiration and respiratory symptoms
- Scott Brown's, Vol. 2, p. 387
7. CLINICAL FEATURES
A. Congenital TOF (Antenatal/Neonatal Presentation)
Antenatal clues:
- Maternal polyhydramnios (in ~50% of OA cases) - fetus cannot swallow amniotic fluid
- Absent stomach bubble on antenatal USG after 20 weeks (indicates isolated OA)
Postnatal presentation (Gross Type C - most common):
CLINICAL FEATURES FLOWCHART - NEONATAL TOF
─────────────────────────────────────────────────────────────
Newborn at delivery
│
▼
"The 3 C's + D" (Mnemonic - Hazarika)
│
├── CHOKING on first feed
├── COUGHING (respiratory distress)
├── CYANOSIS (episodes during feeding)
└── DROOLING (excessive salivation)
│
├── Abdominal DISTENSION (air via fistula)
├── PNEUMONIA (right upper lobe - aspiration)
└── INABILITY to pass NG tube > 10 cm from nares
─────────────────────────────────────────────────────────────
Classic test: Inability to pass a 10Fr catheter more than 10 cm from the nares is virtually diagnostic.
B. H-type (Type E) TOF - Presentation in Infancy/Childhood
These patients present to the ENT clinic and are managed by the paediatric otolaryngologist:
- No oesophageal obstruction
- Recurrent chest infections
- Chronic respiratory symptoms mimicking asthma
- Symptoms of bronchospasm
- May be worked up for cystic fibrosis
- Scott Brown's, Vol. 2, p. 387 - "Children who present to the paediatric otolaryngologist are invariably those with an H-type fistula"
C. Acquired TOF (Adult Presentation)
- Chronic cough, worse with oral intake
- Expectoration of food particles
- Recurrent bronchopulmonary infections
- Haemoptysis, fever, frank pneumonia or mediastinitis
- In ventilated patients: inadequate return of tidal volumes, gastric distension, aspiration of tube feeds from airway
8. INVESTIGATIONS
A. Diagnostic Workup Flowchart
DIAGNOSTIC WORKUP FLOWCHART FOR TOF
────────────────────────────────────────────────────────────────────
Suspected TOF (neonatal / adult)
│
┌─────────┴──────────┐
NEONATAL ADULT/ACQUIRED
│ │
▼ ▼
1. CLINICAL TEST: 1. CHEST X-RAY
NG tube (aspiration pneumonitis,
fails at 10 cm gastric bubble)
│ │
▼ ▼
2. PLAIN X-RAY 2. BARIUM SWALLOW
CHEST+ABDOMEN (dilute barium; prone
(tube in pouch; position for H-type)
gas in abdomen │
= fistula present) ▼
│ 3. ENDOSCOPY
▼ (bronchoscopy +
3. ECHOCARDIOGRAM oesophagoscopy)
(pre-op, identify │
cardiac anomalies, ▼
aortic arch position) 4. CT SCAN
│ (malignant TEF only;
▼ assess extent)
4. RENAL USG
(VACTERL screen)
│
▼
5. TRACHEOBRONCHOSCOPY
(identify upper pouch
fistula; confirm position
of TOF before surgery)
────────────────────────────────────────────────────────────────────
Key points (Scott Brown's, Cummings):
- Contrast studies are NOT required in typical neonatal OA+TOF
- If fluoroscopy used: introduce contrast via catheter (to control amount + remove after procedure)
- "Pull-back (tube) oesophagogram" with patient prone/left lateral position: best for H-type TOF
- Barium swallow: small fistulas (<1 cm) best detected with dilute barium
- Bronchoscopy: locates fistula, measures distance from vocal cords and carina, allows biopsy
- A right-sided aortic arch (2% of cases) is important to identify pre-operatively as it changes surgical approach
CXR of newborn with OA+TOF: NG tube curled in upper oesophageal pouch, gas in stomach confirms distal fistula
9. ASSOCIATED ANOMALIES
VACTERL Association (occurs in ~50% of OA+TOF cases):
| Letter | Anomaly |
|---|---|
| V | Vertebral anomalies (extra/missing ribs) |
| A | Anorectal malformations |
| C | Cardiac defects (25-30%, e.g., VSD, ASD, TOF) |
| TE | TrachEo-Esophageal fistula (defining feature) |
| R | Renal or radial limb anomalies |
| L | Limb deformities |
CHARGE Association:
- Coloboma, Heart defects, Atresia choanae, Retardation, Genital/urinary, Ear anomalies
Waterston Risk Classification (preoperative risk stratification - used in Dhingra/Hazarika):
| Group | Criteria | Survival |
|---|---|---|
| A | Birth weight >2.5 kg, well, no major cardiac anomaly | >95% |
| B | Birth weight 1.8-2.5 kg, or uncertain cardiac lesion | ~70% |
| C | Birth weight <1.8 kg, or severe pneumonia, or severe cardiac lesion | ~25-40% |
(Spitz classification has largely replaced Waterston in modern practice)
10. MANAGEMENT
A. Pre-operative / Immediate Management (Neonatal)
IMMEDIATE MANAGEMENT FLOWCHART
────────────────────────────────────────────────────────
Suspected TOF in Newborn
│
▼
1. Nurse PRONE (45° head-up tilt)
│
▼
2. Replogle/Sump suction tube in upper pouch
- Set on continuous aspiration
- Regular air injections to prevent blockage
│
▼
3. AVOID positive pressure ventilation
(causes massive gastric distension through fistula
→ risk of perforation)
│
▼
4. IV access + antibiotics (for aspiration pneumonia)
│
▼
5. Correct metabolic acidosis, stabilise temperature
│
▼
6. Pre-operative investigations:
Echo, Renal USG, CXR, Tracheobronchoscopy
│
▼
7. Proceed to SURGERY when stable
────────────────────────────────────────────────────────
- Scott Brown's, Vol. 2, p. 558 - "The baby should be nursed prone with a sump suction (Replogle) tube in the upper pouch set on continuous aspiration"
B. Surgical Management of Congenital TOF
Anaesthetic consideration: Pre-operative bronchoscopy allows the anaesthetist to position the ETT past the fistula to limit passage of ventilated gas into the stomach.
Standard approach (Gross Type C - most common):
- Right extrapleural thoracotomy (4th interspace) or thoracoscopic (VATS) approach
- Identify and dissect the fistula from surrounding structures
- Divide and suture the fistula flush with the trachea (leaving a blind-ending pouch causes airway obstruction)
- Primary end-to-end oesophageal anastomosis (single layer, all-absorbable sutures)
- Oro- or nasogastric tube placed across anastomosis for early feeds
Long-gap OA management (gap > 3 cm or 2 vertebrae):
MANAGEMENT OF LONG-GAP OESOPHAGEAL ATRESIA
────────────────────────────────────────────────────────────────
Long-Gap OA (> 3 cm gap)
│
┌─────┴──────┐
Short gap Very long gap
(<3 cm but (primary anastomosis
challenging) not feasible)
│ │
▼ ▼
Delayed Oesophageal
Primary Replacement:
Repair ├── Colonic interposition
with ├── Gastric interposition
Foker └── Free jejunal graft
technique
(external
traction
sutures)
────────────────────────────────────────────────────────────────
Foker Technique: Lengthening the oesophagus by applying traction using two sutures attached to each blind end - allows delayed primary anastomosis.
C. Surgical Management of Acquired TEF (Adult)
Pre-operative optimisation:
- ETT advanced below the level of fistula + cuff inflated (prevent further contamination)
- Jejunostomy feeding + venting gastrostomy (NOT NG tube - avoids further oesophageal trauma)
- Antibiotics for pulmonary sepsis
- Wean mechanical ventilation if possible
Surgical approach (Grillo principles):
SURGICAL PRINCIPLES FOR ACQUIRED TEF (Grillo)
────────────────────────────────────────────────────────────────────
STEP 1: EXPOSURE
Proximal TEF: Anterior collar incision (± sternotomy extension)
Distal TEF: Right posterolateral thoracotomy (4th-5th interspace)
│
▼
STEP 2: DISSECTION
Segmental tracheal resection + distal tracheal intubation
(especially post-intubation TEF - circumferential cuff damage)
Protect recurrent laryngeal nerves in TEF groove
│
▼
STEP 3: OESOPHAGEAL CLOSURE
Two-layer closure over NGT:
Inner layer: interrupted non-absorbable sutures (mucosal inversion)
Outer layer: approximated oesophageal musculature
│
▼
STEP 4: TRACHEAL REPAIR
Stay sutures (2-0 vicryl) proximal + distal to anastomosis
End-to-end tracheal anastomosis
│
▼
STEP 5: TISSUE BUTTRESS
Pedicled flap interposed between trachea and oesophagus:
- Sternohyoid muscle flap
- Strap muscle flap
- Sternocleidomastoid flap
- Pericardial fat pad
- Intercostal muscle (thoracic approach)
────────────────────────────────────────────────────────────────────
- Cummings, p. block2 - "TEF is best managed by interposition of viable tissue between the membranous trachea and the esophagus"
- Current Surgical Therapy, p. 1026
For Malignant TEF: Surgery is rarely feasible. Management is palliative:
- Double stenting (combined oesophageal + airway stent) - preferred
- Single oesophageal stent
- Photodynamic therapy (palliative)
- Nutritional support (percutaneous endoscopic gastrostomy/PEG)
11. POST-OPERATIVE COMPLICATIONS
COMPLICATIONS AFTER TOF REPAIR
───────────────────────────────────────────────────────────
EARLY LATE
───────────────────────────────────────────────────────────
• Anastomotic leak (10-15%) • Anastomotic stricture
• Pneumothorax • Refistulation (recurrent TEF)
• Chylothorax • Gastro-oesophageal reflux (GERD)
• Wound infection • Oesophageal dysmotility
• Vocal cord palsy • Tracheomalacia
(RLN injury) • Impaired pulmonary function
• Aspiration pneumonia (only 20% have normal
• Mediastinitis PFT - Helsinki study)
───────────────────────────────────────────────────────────
Recurrent TOF: If the fistula is not sutured flush with the trachea, a blind-ending pouch causes intermittent airway obstruction and eventual refistulation.
12. PROGNOSIS
- Type C with no cardiac anomaly: survival 95-100% in experienced centres
- Waterston Group A: >95% survival
- Waterston Group C (small weight + severe cardiac): 25-40%
- Associated very low birth weight and major cardiac defects = poor outcome markers
- K. J. Lee's Essential Otolaryngology, p. 693 - "60% to 80% survival except if cardiac or genitourinary abnormalities present, then survival drops to 22%"
13. ROLE OF ENT SURGEON
As emphasised in Scott Brown's and relevant for RGUHS examination:
- H-type fistula (Type E) typically presents to the ENT clinic with chronic respiratory complaints
- The ENT surgeon performs tracheobronchoscopy to confirm diagnosis and identify fistula pre-operatively
- ENT manages complications: tracheomalacia, laryngeal/subglottic stenosis, vocal cord palsy
- Post-laryngectomy TOF: created intentionally for voice rehabilitation (tracheo-oesophageal puncture/TEP); may enlarge pathologically and require surgical closure
- Scott Brown's (single vol.), p. block3 - "Tracheo-oesophageal puncture" for voice rehabilitation after laryngectomy
14. RECENT ADVANCES (2021-2026)
Based on PubMed-indexed reviews and the 2025 Advanced Science review (PMID: 40892023):
A. Minimally Invasive Surgery
- Thoracoscopic (VATS) repair has become the preferred approach at many paediatric surgical centres, replacing open thoracotomy
- Associated with less pain, shorter hospital stay, better cosmesis, reduced adhesion formation
- Long-term outcomes equivalent to open repair
B. Endoscopic Techniques for H-type TOF
- Cauterisation and trichloroacetic acid application to fistula tract under endoscopic guidance
- Fibrin glue/biological glue injection for small fistulas
- Promising early results - "more than one treatment is often needed and long-term results are not known"
- Cummings, p. block46
C. Advanced Stenting for Malignant TOF
- Double-stenting (simultaneous oesophageal + airway stent): improves quality of life vs single stent
- Fully covered self-expanding metal stents (FCSEMS) - allow repositioning/removal
- Biodegradable stents: avoid stent-related migration and erosion
- Y-stents and bifurcated stents for TEF at carina
D. Regenerative Medicine and Tissue Engineering (Li et al., 2025 - Advanced Science)
- Tissue-engineered scaffolds seeded with autologous cells for reconstruction of long-gap defects
- Platelet-rich plasma (PRP) to accelerate wound healing and fistula closure in refractory cases
- Decellularised matrices as biological scaffolds for oesophageal reconstruction
E. 3D Printing and Precision Surgery
- Patient-specific 3D-printed tracheal prostheses for reconstruction after segmental resection
- Computational modelling for pre-operative planning of complex repairs
- AI-assisted endoscopic detection and characterisation of fistulas
F. Flap-Based Closure Advances
- Free flap and pedicled flap reconstruction for refractory/recurrent acquired TEF
- Sternocleidomastoid, pectoralis major, deltopectoral, and anterolateral thigh free flaps
- PMID 38466164 (Laryngoscope, 2024) - Flap-based closure of acquired TEF
G. Changing Causes of Acquired TEF
- PMID 40047082 (Ann Surg, 2025) - Over 40 years of follow-up: aetiology has shifted from infectious/benign to post-oncological/radiation-induced TEF; single-stage repair success rates have improved with better perioperative care
15. SUMMARY TABLE FOR QUICK REVISION
| Feature | Type C (OA+distal TEF) | H-type (Type E) |
|---|---|---|
| Incidence | 85% | 4% |
| OA present | Yes | No |
| Presents | At birth | Infancy/childhood |
| Symptoms | Drooling, choking, cyanosis | Recurrent chest infections |
| Key investigation | CXR + failed NG tube | Pull-back oesophagogram; bronchoscopy |
| Surgery | R thoracotomy / thoracoscopy | Neck exploration |
| ENT relevance | Pre-op bronchoscopy | Presents to ENT clinic |
SOURCES CITED
- Scott Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 (9781138094634) - Chapter 45, Oesophageal disorders in children, pp. 557-559
- Scott Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1 (9781138094611) - Paediatric airway, p. 387
- Cummings Otolaryngology Head and Neck Surgery (9780323612173) - Tracheotomy complications (block2); Imaging (block21); Paediatric airway/oesophagus (block46)
- K. J. Lee's Essential Otolaryngology (9781260122237) - p. 693
- Current Surgical Therapy, 14e - Acquired TEF management, pp. 1025-1026
- Li G et al. Adv Sci (Weinh). 2025. PMID: 40892023 - Comprehensive review with future directions
- Walker B, Axtell AL. Thorac Surg Clin. 2025 Feb. PMID: 39515897 - Management of TEF and tracheoinnominate fistula
- Fadel G et al. Ann Surg. 2025. PMID: 40047082 - Changing causes and surgical methods over 40 years
- Cohen WG et al. Laryngoscope. 2024. PMID: 38466164 - Flap-based closure of acquired TEF
RGUHS Examination Tip: For a 50-mark question on TOF, the examiner expects: definition + embryology (5 marks), classification with Gross diagram (10 marks), clinical features + investigations with flowchart (15 marks), management with pre-op/surgical/post-op (15 marks), and recent advances (5 marks). Always mention the ENT relevance of H-type TOF, the Replogle tube, VACTERL association, and at least two recent advances (VATS repair + endoscopic techniques). The Waterston risk classification is specifically asked in RGUHS/Karnataka/Indian PG exams.
This is a shared conversation. Sign in to Orris to start your own chat.