Active management of 3rd stage labour
Reading File
Finding Sources
Finding Sources
Searching PubMed
"active management" AND "third stage of labor"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer.
Active Management of the Third Stage of Labour (AMTSL)
Definition of the Third Stage
The third stage of labour spans from delivery of the infant to delivery of the placenta. It normally completes within 5-30 minutes. Beyond 18 minutes, the risk of postpartum hemorrhage (PPH) increases significantly - and is up to six times more likely after 30 minutes. - Rosen's Emergency Medicine, p. 3412
Why Active Management?
Active management is strongly preferred over expectant (physiological) management because it:
-
Decreases the duration of the third stage
-
Reduces maternal blood loss
-
Reduces the incidence of PPH
-
Reduces the need for blood transfusion
-
Reduces the need for additional uterotonic medication
-
Swanson's Family Medicine Review, p. 516; Pfenninger & Fowler's Procedures for Primary Care, p. 1222
The Three Core Components of AMTSL
1. Uterotonic Administration
Oxytocin is the first-line agent, given as soon as the anterior shoulder is delivered (before placental separation).
| Route | Dose | Notes |
|---|---|---|
| IV infusion | 20-40 units in 1 L IV fluid | Run at 10 mL/min initially, then reduce to 1-2 mL/min once uterus is contracted |
| IM | 10 units | Given after placental delivery in some protocols |
Important: Oxytocin should NOT be given as a rapid IV bolus (risk of cardiovascular collapse). It should also not be given before placental delivery if an undetected twin is possible, as it could trap placental fragments.
Alternative/second-line uterotonics:
| Drug | Dose/Route | Special Notes |
|---|---|---|
| Methylergonovine maleate | 0.2 mg IM | Contraindicated in hypertension/pre-eclampsia (vasoconstrictive) |
| Ergonovine maleate | 0.2 mg IM | Same contraindication as above |
| Misoprostol | 600-800 mcg sublingually/rectally | Useful in low-resource settings; causes more nausea/shivering |
| Tranexamic acid | Adjunct IV | Evidence from RCTs supports prophylactic use alongside oxytocin to prevent PPH |
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 3781; Miller's Anesthesia 10e
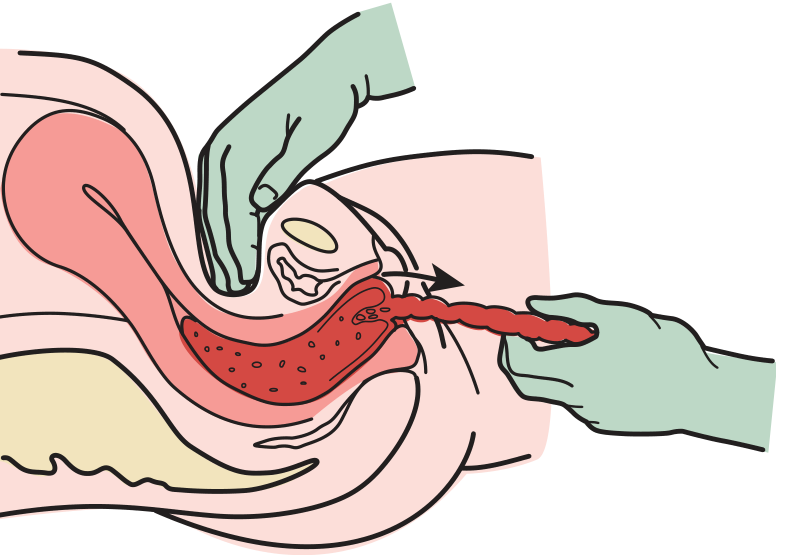
2. Controlled Cord Traction (CCT) - Brandt-Andrews Maneuver
After signs of placental separation appear (see below), CCT is performed:
Signs of placental separation:
- Uterus becomes firmer and rises in the abdomen
- Umbilical cord lengthens by 5-10 cm
- Sudden gush of blood per vaginum
Technique:
- One hand placed suprapubically (over the lower uterine segment) to provide counter-traction - pushing the uterus cephalad and posteriorly to prevent uterine inversion
- The other hand applies firm but gentle traction on the clamped cord
- Ask the mother to bear down to assist with expulsion
- As the placenta reaches the introitus, lift it upward and out; use gentle twisting traction to assist membrane delivery
- Remove any retained membranes with ring forceps
Never apply forceful traction before placental separation - this risks cord avulsion or uterine inversion, a potentially catastrophic complication.
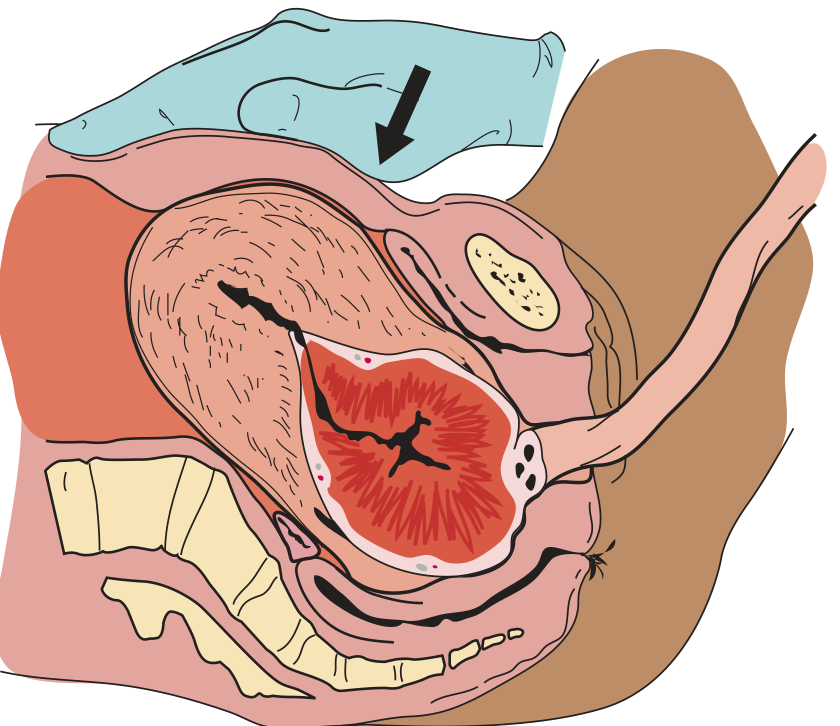
3. Uterine Massage
-
After delivery of the placenta, the uterus is massaged transabdominally to promote and maintain contraction
-
Continuous palpation to monitor for uterine atony
-
Massage is repeated any time signs of uterine relaxation appear
-
Rosen's Emergency Medicine, p. 3412; Swanson's Family Medicine Review, p. 516
Cord Management
- Early cord clamping is part of AMTSL; however, delayed cord clamping (30-60 seconds or more) is recommended by many guidelines (especially for preterm neonates) to allow placento-fetal transfusion
- Before cutting, allow 7-10 mL of cord blood to drain from the placental side - this shortens the third stage
- Check the cord for 3 vessels (2 arteries + 1 vein); a 2-vessel cord occurs in 1:500 deliveries and is associated with fetal anomalies
Management if Placenta Does Not Deliver Within 30 Minutes
If the placenta is retained at 30 minutes:
- The cervical os may have contracted around the placenta (trapped placenta) - try the Brandt maneuver: firm suprapubic pressure plus firm cord traction
- Intra-umbilical vein injection of oxytocin (20 IU in 20 mL normal saline) may stimulate uterine contraction and facilitate delivery
- If these fail → manual removal of the placenta under analgesia/anaesthesia (indicated in ~3% of vaginal deliveries)
Examination After Delivery
Always inspect:
- Placenta: check for completeness - missing cotyledons suggest retained placental fragments
- Cord: count vessels; look for velamentous insertion or accessory lobes
- Perineum, vagina, and cervix: inspect for lacerations at 3 and 9 o'clock positions (cervical), ischial spine level (vaginal), and perineum
Fourth Stage Monitoring
The first hour after placental delivery is the fourth stage - the highest-risk period for PPH (uterine atony accounts for 75-90% of PPH cases). Perform:
- Frequent fundal height and tone checks
- Transabdominal massage if any uterine relaxation
- Continue oxytocin infusion to sustain uterine contraction
Summary Table
| Component | Timing | Action |
|---|---|---|
| Uterotonic (oxytocin) | On delivery of anterior shoulder | 20-40 U in 1L IV, or 10 U IM |
| Early cord clamping | After delivery | 3-4 cm from umbilicus; check 3 vessels |
| Controlled cord traction | After signs of placental separation | Counter-traction suprapubically; gentle traction on cord |
| Uterine massage | After placental delivery | Transabdominal; repeat if relaxation occurs |
| Placenta inspection | Immediately after delivery | Check completeness, cord vessels, anomalies |
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 38700065) on AMTSL knowledge and practice in sub-Saharan Africa, and a 2026 evidence summary on PPH prevention (PMID 42422824), both reaffirm that oxytocin-based AMTSL remains the standard of care globally. No findings contradict current textbook recommendations.
This is a shared conversation. Sign in to Orris to start your own chat.