Heart
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from Guyton and Hall to provide a thorough answer on cardiac physiology. Let me compile the full response.
Heart Physiology & Function
Source: Guyton and Hall Textbook of Medical Physiology
Overview: The Heart as a Pump
The heart functions as a dual pump, with the right and left ventricles working in series. The right ventricle pumps blood through the pulmonary circulation (low-pressure system, ~8 mm Hg), and the left ventricle pumps blood through the systemic circulation (high-pressure system, ~80-120 mm Hg). The right ventricle's work output is about one-sixth that of the left ventricle due to this pressure difference.
The Cardiac Cycle
The cardiac cycle describes the complete sequence of events from one heartbeat to the next. It consists of two main phases: systole (contraction) and diastole (relaxation).
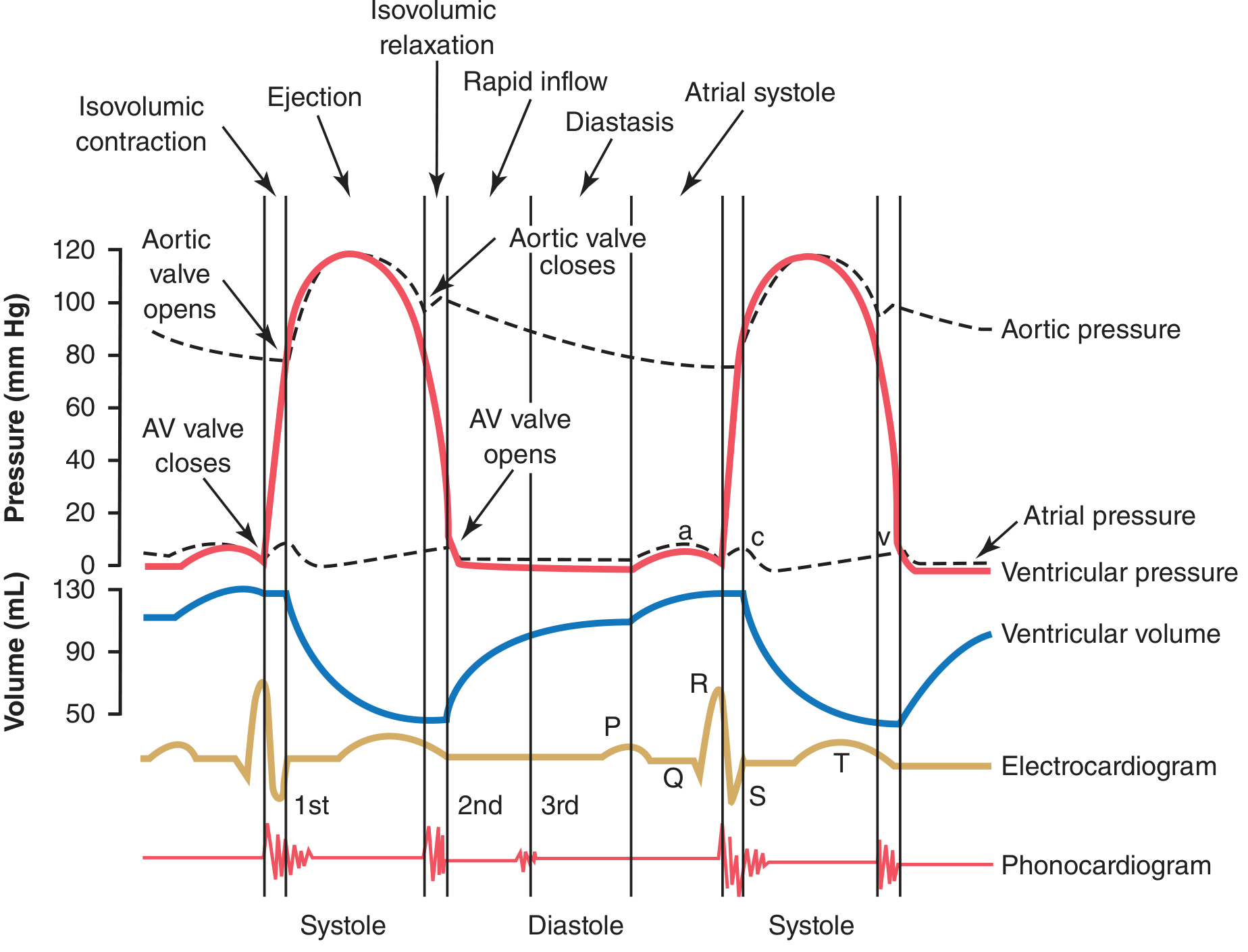
Events of the cardiac cycle (Guyton and Hall, Fig. 9.8): Atrial pressure (dashed), ventricular pressure (red), aortic pressure (dashed), ventricular volume (blue), ECG (gold), and phonocardiogram (red, bottom).
Phases of the Cardiac Cycle
1. Ventricular Filling (Diastole)
- After systole ends, AV valves open as ventricular pressure drops below atrial pressure.
- First third of diastole - rapid filling: ~70-80% of blood flows passively from atria into ventricles.
- Middle third - diastasis: slow passive filling from veins.
- Last third - atrial contraction ("atrial kick") contributes an additional 20-30% filling, acting as a "booster pump."
The atria serve three roles: reservoir (blood accumulates during systole), conduit (passive flow into ventricles), and contractile (active "kick"). If the atria fail, cardiac output is still maintained at rest, but may fall short during exercise.
2. Isovolumic (Isometric) Contraction
- Ventricular contraction begins; pressure rises sharply, closing the AV valves (producing S1 - first heart sound).
- No blood is ejected yet - both AV and semilunar valves are closed.
- Duration: ~0.02-0.03 seconds, until pressure exceeds aortic (~80 mm Hg) and pulmonary (~8 mm Hg) pressures.
3. Ejection
- Left ventricular pressure exceeds ~80 mm Hg → aortic valve opens.
- Right ventricular pressure exceeds ~8 mm Hg → pulmonary valve opens.
- Rapid ejection phase (first third): ~70% of the ejected volume is pumped out.
- Slow ejection phase (last two-thirds): remaining 30% is ejected.
- Ejection fraction (EF): normally about 60% of end-diastolic volume is ejected per beat.
4. Isovolumic Relaxation
- Systole ends; ventricular pressure drops suddenly.
- Aortic pressure pushes blood back toward the ventricle, snapping the aortic and pulmonary valves shut → S2 - second heart sound.
- AV valves remain closed during this brief period (~0.03-0.06 seconds).
5. Rapid Inflow (Early Diastole)
- When ventricular pressure falls below atrial pressure, AV valves reopen and the cycle begins again.
Atrial Pressure Waves (a, c, and v Waves)
| Wave | Cause | Approximate Pressure Rise |
|---|---|---|
| a wave | Atrial contraction | Right atrium: 4-6 mm Hg; Left atrium: 7-8 mm Hg |
| c wave | Bulging of AV valves back into atria at onset of ventricular contraction | Small elevation |
| v wave | Passive filling of atria from veins while AV valves are closed during systole | Small elevation; disappears when AV valves open |
ECG Correlation with the Cardiac Cycle
| ECG Event | Mechanical Event |
|---|---|
| P wave | Atrial depolarization → atrial contraction |
| QRS complex | Ventricular depolarization → ventricular systole begins |
| T wave | Ventricular repolarization → ventricular muscle begins to relax |
Heart Sounds
- S1 (first heart sound): Low-pitched, long sound from AV valve closure at the start of systole.
- S2 (second heart sound): Short, sharp snap from aortic and pulmonary valve closure at the end of systole.
- S3 and S4 sounds may be heard in certain pathological conditions (e.g., heart failure, stiff ventricles).
Regulation of Cardiac Pumping
Frank-Starling Mechanism
The more the ventricle is stretched by incoming blood (increased preload), the more forcefully it contracts and the more blood it ejects. This is expressed via ventricular function curves: as atrial pressure increases, stroke work output increases until the ventricle reaches its pumping limit.
Autonomic Nervous Control
The heart is richly supplied by both sympathetic and parasympathetic (vagal) fibers:
-
Sympathetic stimulation:
- Increases heart rate (chronotropy): from 70 bpm up to 180-250 bpm.
- Increases force of contraction (inotropy): can double contractile force.
- Can increase cardiac output 2-3 fold above normal.
-
Parasympathetic (vagal) stimulation:
- Decreases heart rate; heavy vagal stimulation can nearly stop the heart transiently.
- Reduces contractile force in the atria.
- Can reduce cardiac output nearly to zero.
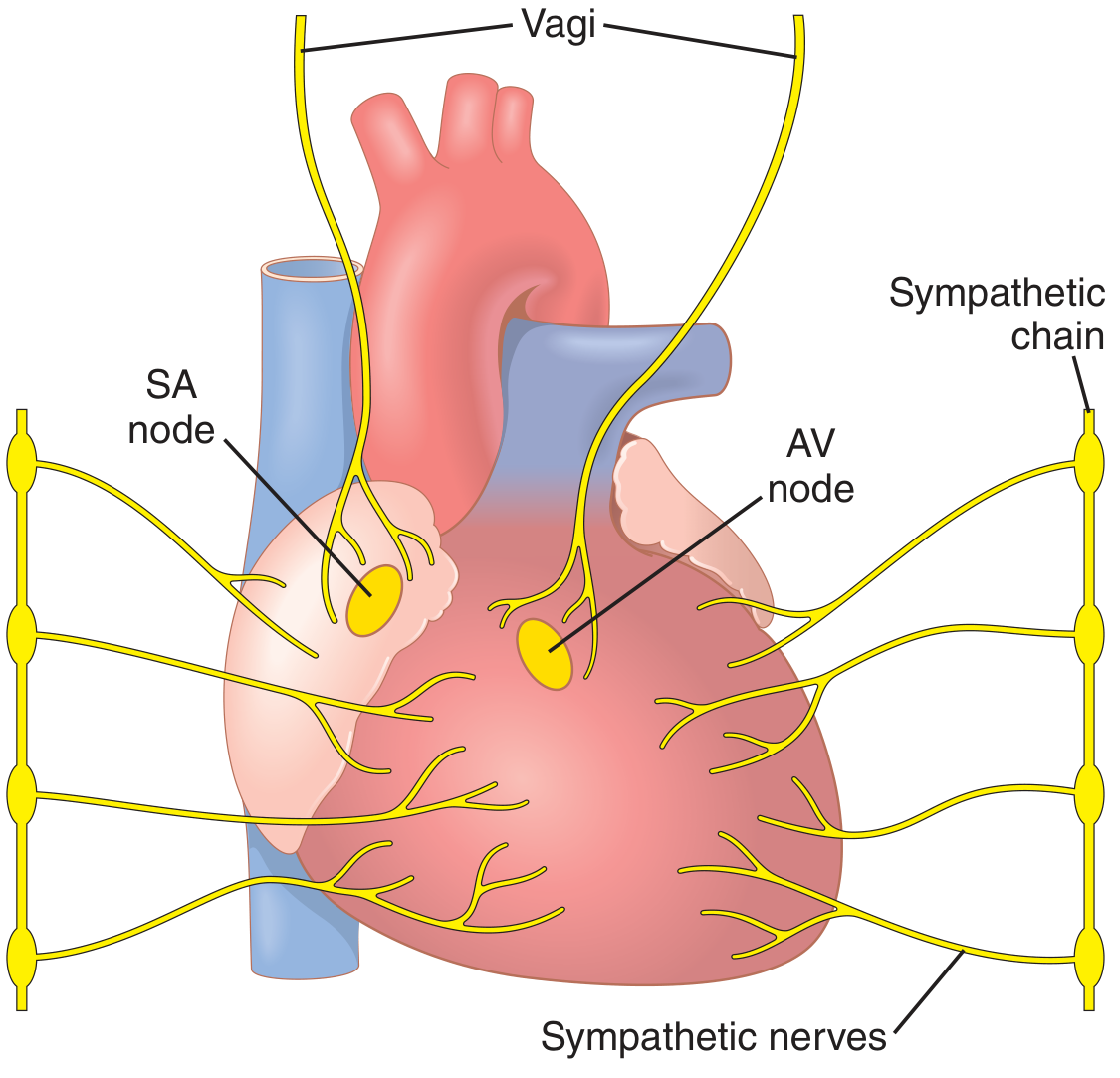
Sympathetic (acceleratory) and parasympathetic vagus nerve supply to the heart (Guyton and Hall, Fig. 9.14)
Volume-Pressure Relationship
- End-diastolic volume (EDV): ~130 mL (normal, at rest).
- End-systolic volume (ESV): ~50 mL (volume remaining after ejection).
- Stroke volume (SV) = EDV - ESV = ~80 mL.
- Cardiac output (CO) = SV × Heart Rate = 80 mL × 70 bpm = ~5.6 L/min at rest.
The diastolic pressure-volume curve is relatively flat below ~150 mL filling; above this, pressure rises steeply due to fibrous tissue and pericardial constraints. The systolic pressure curve is always above the diastolic curve - the enclosed area represents the net external work of each heartbeat.
Work Output
The heart converts chemical energy to two forms of mechanical work:
- Volume-pressure (external) work - the major component; moves blood from low-pressure veins to high-pressure arteries.
- Kinetic energy of blood flow - minor (~1% normally), but rises dramatically in aortic stenosis (>50% of total work).
Key Physiological Concepts Summary
| Parameter | Normal Value |
|---|---|
| Resting heart rate | 70 beats/min |
| Left ventricular systolic pressure | ~120 mm Hg |
| Aortic diastolic pressure | ~80 mm Hg |
| Stroke volume | ~70-80 mL |
| Ejection fraction | ~60% |
| Cardiac output (rest) | ~5-6 L/min |
| Right ventricular systolic pressure | ~20 mm Hg (1/6 of left) |
- Guyton and Hall Textbook of Medical Physiology, pp. 127-133 (Block 2)
This is a shared conversation. Sign in to Orris to start your own chat.