Finding of asd and vsd with and without ductus arteriosus in newborn
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
ASD, VSD, and Patent Ductus Arteriosus in the Newborn
These three defects are the most common left-to-right shunt congenital heart lesions (acyanotic defects). Together they account for the majority of congenital cardiac malformations. The diagram below illustrates all three:
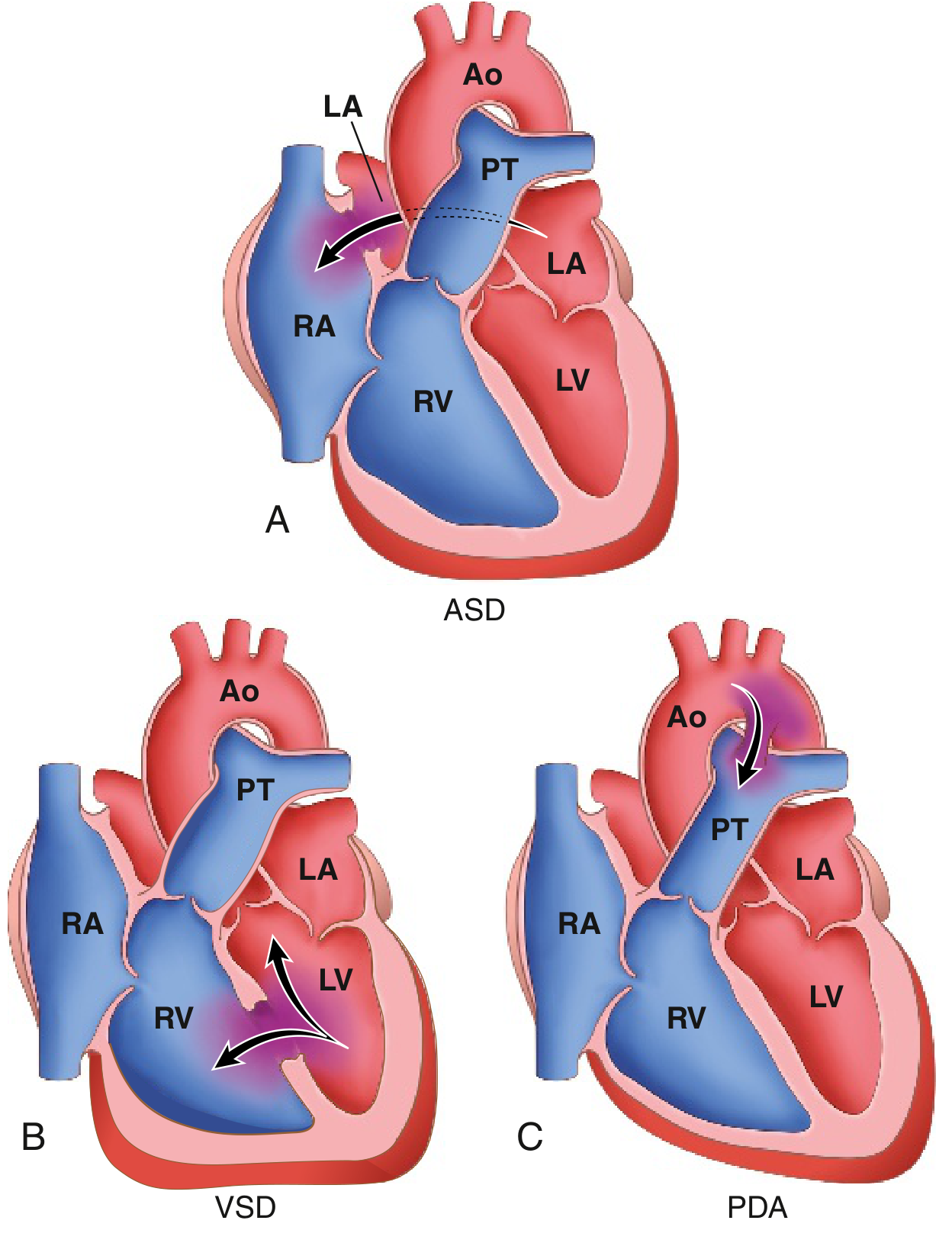
Fig. 9.2 - Common congenital causes of left-to-right shunts: (A) ASD, (B) VSD, (C) PDA. Arrows show direction of blood flow.
Atrial Septal Defect (ASD)
What It Is
An ASD is an abnormal fixed opening in the atrial septum allowing unrestricted blood flow between the atrial chambers. It must be distinguished from a patent foramen ovale (PFO), which is a valve-like flap rather than a true defect.
Types:
- Ostium secundum ASD (90%) - smooth-walled defect near the foramen ovale; insufficient growth of septum secundum. Most common type, rarely associated with other anomalies.
- Ostium primum ASD - located in the inferior atrial septum, near the atrioventricular valves; often associated with a cleft anterior leaflet of the mitral valve (part of AV canal defect spectrum). ECG shows left axis deviation + incomplete RBBB.
- Sinus venosus ASD - near the orifice of the superior or inferior vena cava; commonly associated with anomalous pulmonary venous return; easily missed on transthoracic echo.
Physiology
- Creates a left-to-right shunt (pretricuspid shunt) - volume loading of the right ventricle and pulmonary circulation only (not pressure loading)
- Well tolerated in childhood; symptoms typically emerge after the 3rd-4th decade
- Over 70% of patients are impaired by the 5th decade
Clinical Findings in the Newborn/Child
- Usually asymptomatic in infancy and early childhood
- ASD is the most common defect first diagnosed in adulthood (because VSDs and PDAs present earlier)
- Auscultation: Wide and fixed splitting of S2 (hallmark) - doesn't vary with respiration; soft midsystolic pulmonary ejection murmur (2nd left interspace); mid-diastolic murmur at lower left sternal border (if large shunt, from increased tricuspid flow)
- ECG: Incomplete right bundle branch block (rSr' in V1); right axis deviation (ostium secundum); left axis deviation (ostium primum)
- CXR: Pulmonary vascular plethora, dilated pulmonary artery, right atrial and right ventricular dilation
- Echo: Diagnostic - identifies type and quantifies shunt ratio; color Doppler shows LA-to-RA flow
Complications (if untreated)
- Pulmonary hypertension (less common than with VSD/PDA since it is a pretricuspid lesion)
- Right-sided heart failure
- Atrial arrhythmias (flutter, fibrillation)
- Paradoxical embolism (right-to-left flow during Valsalva)
Ventricular Septal Defect (VSD)
What It Is
VSD is the most common congenital cardiac anomaly diagnosed at birth, constituting defects in the interventricular septum that allow left-to-right shunting.
Anatomic locations:
| Type | Proportion | Location |
|---|---|---|
| Perimembranous (infracristal) | ~80% | Membranous septum beneath aortic valve; may extend into inlet or outlet |
| Infundibular (supracristal/outlet) | Less common | Conal septum above crista supraventricularis, below pulmonary valve |
| Inlet defects | Less common | Crux of heart between tricuspid and mitral valves; associated with AV canal anomalies |
| Muscular (trabecular) | Variable | Multiple defects possible; distal to tricuspid septal attachment toward apex |
The basal (membranous) region is the last to develop and is the site of ~90% of VSDs.
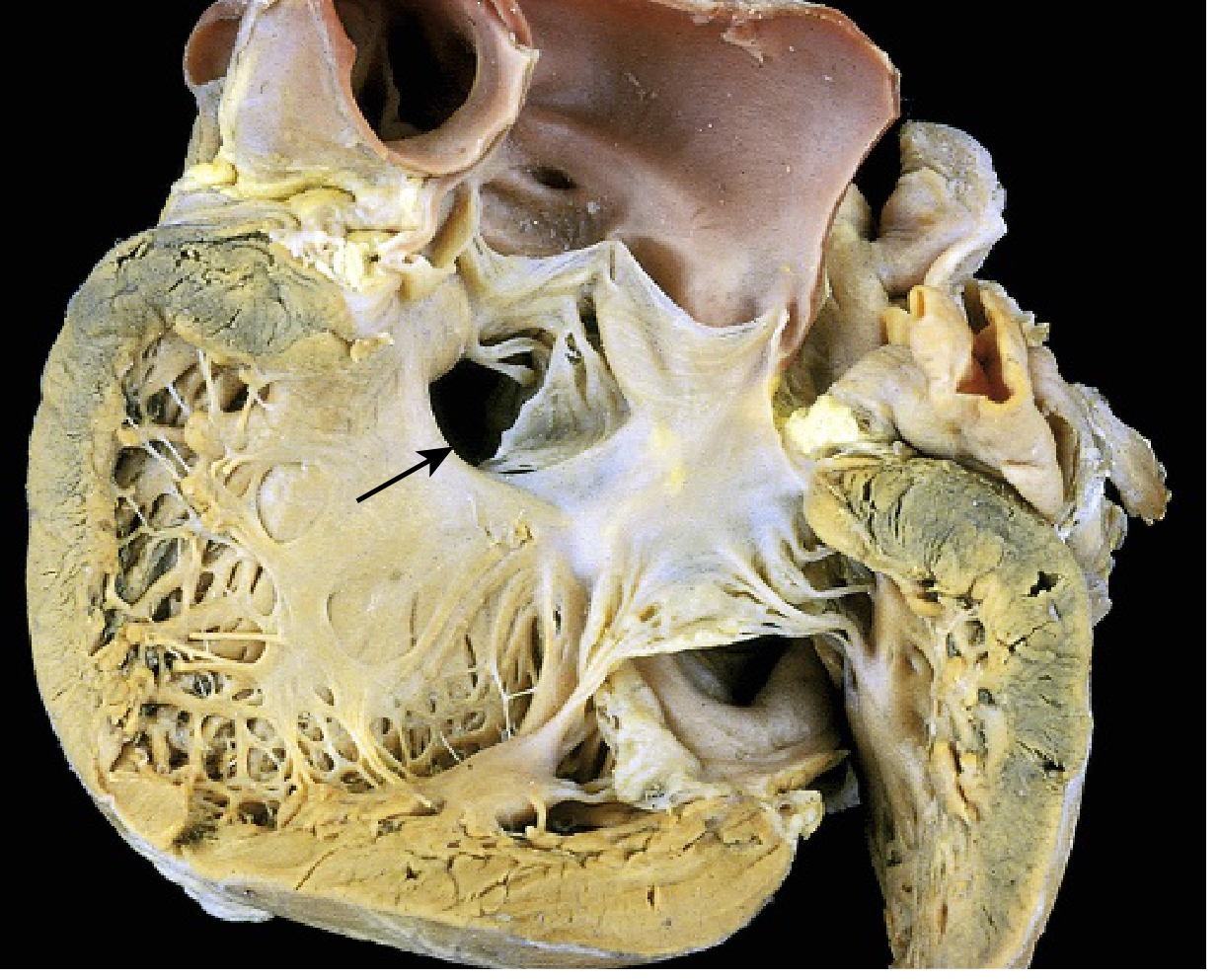
Fig. 9.3 - VSD of the membranous type (arrow). The defect is visible in the dissected heart specimen.
Physiology
- A posttricuspid shunt - causes both volume AND pressure loading of the right ventricle and pulmonary circulation (more hemodynamically significant than ASD of equivalent size)
- Shunting occurs predominantly during systole (when LV pressure exceeds RV pressure)
- ~50% of all native VSDs are small; more than half of small VSDs close spontaneously (highest closure rates in the first decade)
- Moderate or large VSDs rarely close spontaneously (~10%)
Clinical Findings in the Newborn/Infant
- Small VSD: Often asymptomatic; detected by a loud, harsh holosystolic murmur at the left sternal border; no hemodynamic significance
- Large VSD: Symptoms develop in weeks to months - failure to thrive, frequent respiratory infections, tachypnea, diaphoresis with feeds, signs of congestive heart failure
- Auscultation: Grade 4+ harsh, widely radiating holosystolic murmur (lower left sternal border); palpable thrill
- ECG: Biventricular hypertrophy (large VSDs); right ventricular hypertrophy as pulmonary pressure rises
- CXR: Cardiomegaly, increased pulmonary vascularity (plethora), prominent pulmonary artery
- Echo: Diagnostic; defines location, size, and Qp:Qs ratio; Doppler shows systolic LV-to-RV jet
Complications
- Pulmonary hypertension develops earlier and more frequently than with ASD (due to higher flow volumes and pressures in the pulmonary circulation)
- Eisenmenger syndrome in ~10% (reversal of shunt - cyanosis, clubbing, polycythemia): closure then contraindicated
- Risk of infective endocarditis (jet lesion causes endothelial damage in right ventricle)
- CHF if defect is large
Patent Ductus Arteriosus (PDA)
Normal Physiology and Closure
The ductus arteriosus connects the left pulmonary artery to the descending aorta just distal to the left subclavian artery. During fetal life, it diverts blood away from the unexpanded, unventilated lungs (pulmonary artery → aorta flow).
At birth, three factors trigger constriction:
- Increased arterial oxygen tension (lungs expand)
- Decreased pulmonary vascular resistance
- Declining local prostaglandin E2 levels
Functional closure occurs within 1-2 days in healthy term infants; complete anatomic obliteration (forming the ligamentum arteriosum) takes several weeks to months.
When PDA Persists
| Condition | Mechanism |
|---|---|
| Prematurity (<28 weeks, <1750 g) | Nearly 100% of very preterm neonates have PDA in first 24 hours; hypoxia + immaturity |
| Hypoxia / respiratory distress syndrome | Low O2 prevents ductal constriction; surfactant deficiency aggravates |
| Congenital rubella infection | Maternal rubella in early pregnancy is a classic cause |
| High altitude | Relative hypoxia |
| Associated cardiac defects (coarctation, TGA, pulmonary atresia) | Large pressure gradients prevent normal constriction |
PDA accounts for approximately 7% of congenital heart lesions; 90% are isolated defects. It is 2-3x more common in females.
Physiology
- A posttricuspid shunt (like VSD): causes both volume and pressure loading
- Direction of shunt reverses if pulmonary pressure exceeds aortic pressure (Eisenmenger)
- In Eisenmenger PDA: lower limb cyanosis and clubbing > upper limbs (differential cyanosis) because deoxygenated pulmonary blood enters the aorta distal to the subclavian arteries
Clinical Findings
- Small PDA: Asymptomatic; detected incidentally; risk of infectious endarteritis (~0.45%/year)
- Moderate/Large PDA: Bounding pulses (wide pulse pressure due to diastolic runoff into pulmonary artery); active precordium; signs of CHF in infancy
- Auscultation (classic): Continuous "machinery" murmur - heard at the 1st or 2nd left intercostal space below left clavicle; peaks at S2; diastolic component shortens as pulmonary pressure rises; murmur disappears with Eisenmenger syndrome
- ECG: Left atrial and left ventricular hypertrophy (volume overload pattern)
- CXR: Dilated ascending aorta and pulmonary artery; enlarged left-sided chambers; calcification at PDA site in older patients
- Echo: May not directly visualize PDA but Doppler identifies continuous aortopulmonary flow signal
Treatment
- Premature infants: Indomethacin or ibuprofen (prostaglandin inhibitors) - accelerates closure; may not eliminate need for intervention
- Surgical ligation: Standard for failed medical therapy or anatomically unsuitable defects
- Percutaneous catheter closure: Preferred in suitable patients (coils, Amplatzer device)
Key Comparison: ASD vs. VSD vs. PDA in the Newborn
| Feature | ASD | VSD | PDA |
|---|---|---|---|
| Prevalence | 2nd most common in adults | Most common at birth | ~7% of CHD |
| Shunt level | Atrial (pretricuspid) | Ventricular (posttricuspid) | Great vessels (posttricuspid) |
| Hemodynamic effect | RV volume load only | RV volume + pressure load | LV volume + pulmonary pressure load |
| Spontaneous closure | Unlikely | ~50% small VSDs | In term infants: yes (1-2 days) |
| Murmur | Soft systolic + fixed split S2 | Harsh holosystolic | Continuous "machinery" |
| ECG | Incomplete RBBB + RAD | RVH or BVH (large defect) | LVH + LAH |
| Cyanosis (late) | Eisenmenger (late, rare) | Eisenmenger (~10%) | Eisenmenger (5%); differential cyanosis lower limbs |
| Pulmonary HTN | Late, less common | Earlier, more common | Variable |
| Medical treatment | None | None | Indomethacin/ibuprofen (preterm) |
Role of the Ductus in Context of ASD/VSD
When an ASD or VSD coexists with a persistent PDA, the combined hemodynamic burden on the pulmonary circulation is substantially greater. A PDA associated with coarctation of the aorta, pulmonary atresia, or transposition of the great arteries (TGA) may actually be life-sustaining - in those situations, the ductus is deliberately kept open with prostaglandin E1 (alprostadil) infusion until surgical repair is possible. This is the fundamental distinction between "ductus-dependent" and "ductus-independent" congenital heart disease.
Sources: Robbins & Kumar Basic Pathology, pp. 348-350 | Goldman-Cecil Medicine, pp. 608-612 | Creasy & Resnik's Maternal-Fetal Medicine, pp. 1250-1256 | The Developing Human (Moore's Embryology), p. 881-882
This is a shared conversation. Sign in to Orris to start your own chat.