2 years old child wuth complaints of tightness of limbs,conscoius oritend, recurrent episodes in past as well and required iv calcium Diffrential diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive textbook data. Let me compile the full differential diagnosis.
Differential Diagnosis: 2-Year-Old with Recurrent Limb Tightness (Tetany) + Response to IV Calcium
The clinical picture - recurrent muscular spasms/tightness of limbs, conscious and oriented (not a seizure with loss of consciousness), and response to IV calcium - is a classic presentation of hypocalcemic tetany. The primary differential is built around the causes of hypocalcemia in a toddler.
Most Likely Diagnosis: Hypocalcemic Tetany
The key response to IV calcium strongly localizes the problem to hypocalcemia. The differentials are then organized by underlying etiology.
PRIMARY DIFFERENTIALS (Causes of Hypocalcemia)
1. Vitamin D Deficiency Rickets (MOST COMMON in this age group)
- The most common cause of hypocalcemic tetany in toddlers aged 1-3 years in developing countries
- Results from nutritional vitamin D and calcium deficiency
- Low 25(OH)D, low calcium, low phosphate, elevated PTH (secondary hyperparathyroidism)
- Associated features: bowing of legs, rachitic rosary, widened wrists, delayed dentition, craniotabes
- Look for: exclusive breastfeeding without supplementation, dark skin, limited sun exposure, poor dietary intake
2. Vitamin D-Dependent Rickets Type 1 (VDDR-1 / Pseudovitamin D Deficiency Rickets)
- Autosomal recessive mutation in 1α-hydroxylase (CYP27B1) - cannot convert 25(OH)D to active 1,25(OH)2D
- Presents in infancy-early childhood with severe hypocalcemia and rickets despite adequate vitamin D intake
- Normal 25(OH)D, very low 1,25(OH)2D, high PTH
- Responds only to calcitriol (active vitamin D), not regular vitamin D
3. Vitamin D-Dependent Rickets Type 2 (VDDR-2)
- Mutation in the Vitamin D Receptor (VDR) - end-organ resistance to active vitamin D
- Similar presentation but does not respond to calcitriol
- Classic clue: alopecia totalis (seen in ~50% of cases)
4. Hypoparathyroidism
Low PTH is the hallmark. Subtypes relevant in a 2-year-old:
- Isolated congenital hypoparathyroidism (PTH gene mutations)
- DiGeorge Syndrome (22q11.2 deletion) - developmental failure of 3rd/4th pharyngeal pouch; associated with cardiac defects, immune deficiency, dysmorphic facies
- Autoimmune hypoparathyroidism - isolated or as part of Polyglandular Autoimmune Syndrome Type 1 (APS-1 / APECED) - look for mucocutaneous candidiasis, adrenal insufficiency
- Kenny-Caffey syndrome / Sanjad-Sakati syndrome - hypoparathyroidism with short stature and dysmorphic features
- Lab: low Ca, high phosphate, low/absent PTH, low urinary calcium
5. Pseudohypoparathyroidism (PHP)
- End-organ resistance to PTH (PTH is high, but target organs don't respond)
- Lab: low Ca, high phosphate, high PTH
- PHP Type 1a: Albright hereditary osteodystrophy (short 4th metacarpal, round face, short stature, subcutaneous ossifications)
- PHP Type 1b: normal phenotype, methylation defect at GNAS locus
- Intracranial (basal ganglia) calcifications on CT are a feature
6. Hypomagnesemia
- Magnesium deficiency impairs both PTH secretion and PTH action at target organs
- Can cause hypocalcemia refractory to calcium replacement unless magnesium is repleted
- Causes: malabsorption, chronic diarrhea, Gitelman syndrome, diuretic use, familial hypomagnesemia syndromes
- Key clue: hypocalcemia not responding adequately to calcium alone
7. Malabsorption Syndromes
- Causes secondary vitamin D and calcium deficiency
- Conditions: celiac disease, short bowel syndrome, inflammatory bowel disease
- Low albumin, fat-soluble vitamin deficiencies
8. Chronic Kidney Disease (CKD)
- Impaired 1α-hydroxylation in the proximal tubule → low 1,25(OH)2D → hypocalcemia
- Phosphate retention → hyperphosphatemia → binds Ca and suppresses 1,25(OH)2D
- Lab: elevated creatinine, high phosphate, high PTH (secondary hyperparathyroidism)
- Often co-existing renal osteodystrophy
9. Alkalosis (Respiratory or Metabolic)
- Alkalosis increases protein binding of calcium → reduces ionized (free) calcium
- Total serum calcium may be normal, but ionized calcium is low
- Common in hyperventilation, prolonged vomiting, sepsis
- Tetany without a structural calcium deficit - resolves with correction of pH
SECONDARY / LESS COMMON DIFFERENTIALS
| Condition | Key Feature |
|---|---|
| Neonatal hypocalcemia (residual) | Less likely at age 2 but consider if premature or birth asphyxia history |
| Celiac disease | Malabsorption + failure to thrive + diarrhea |
| Hyperphosphatemia (phosphate enemas, oral supplements) | Elevated PO4 precipitates calcium |
| Hypoalbuminemia (nephrotic syndrome, malnutrition) | Low total calcium but ionized Ca may be normal - "false hypocalcemia" |
| Anticonvulsant use (phenytoin, phenobarbitone) | Accelerates vitamin D catabolism |
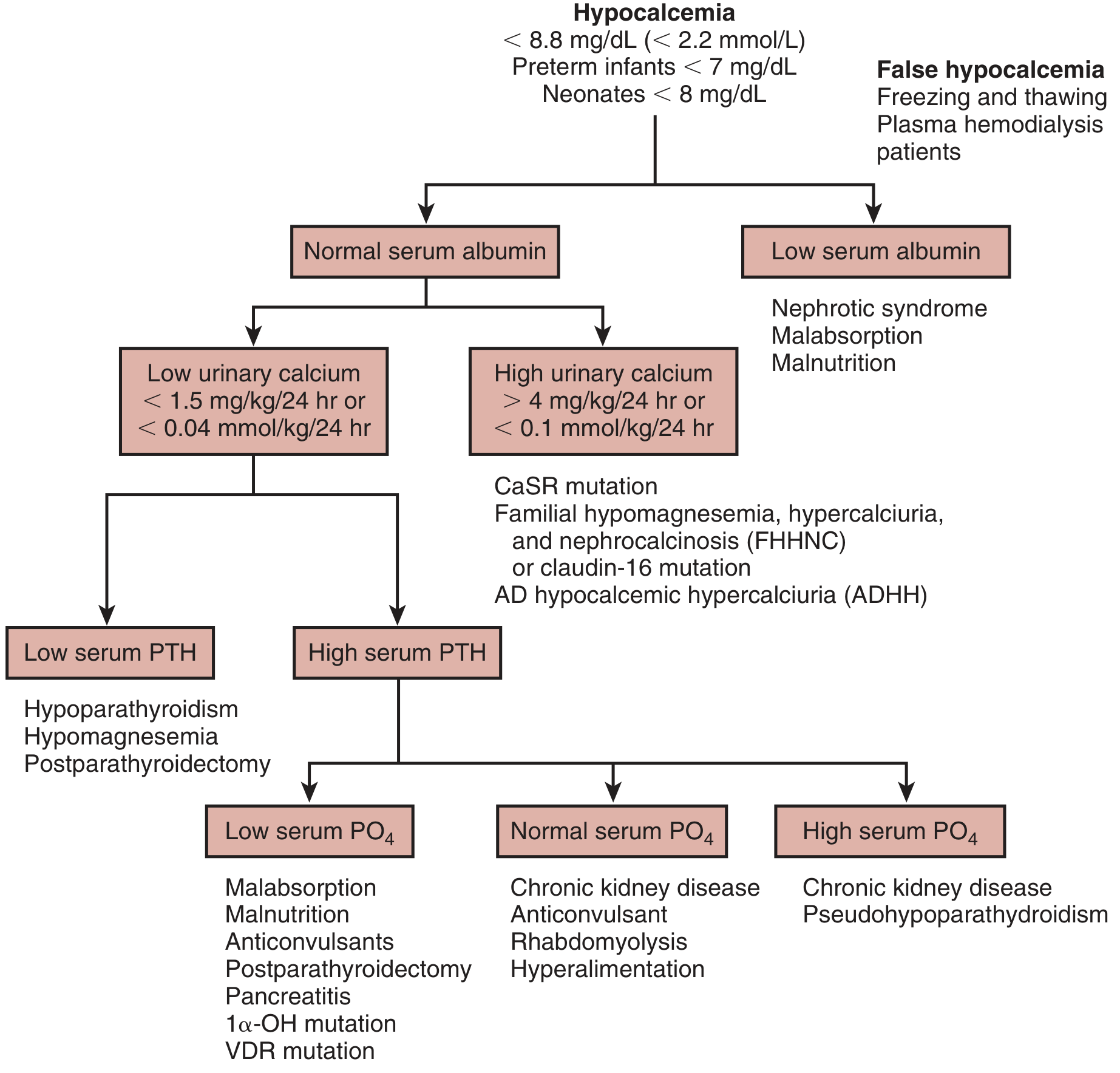
Diagnostic Algorithm (from Brenner & Rector's The Kidney)
Recommended Initial Workup
| Test | Purpose |
|---|---|
| Serum calcium (total + ionized) | Confirm hypocalcemia |
| Serum albumin | Correct total calcium; rule out hypoalbuminemia |
| Serum phosphate | High in PHP, hypoparathyroidism, CKD; low in Vit D deficiency |
| Serum PTH (intact) | Low = hypoparathyroidism; High = resistance or secondary |
| 25(OH)D | Screen for vitamin D deficiency |
| 1,25(OH)2D | Low in CKD, VDDR-1 |
| Serum magnesium | Rule out hypomagnesemia |
| Serum creatinine/BUN | Rule out CKD |
| Urine calcium/creatinine ratio | Low in hypoparathyroidism; high in CaSR mutations |
| X-ray wrists/knees | Rachitic changes |
| ALP (alkaline phosphatase) | Elevated in rickets and metabolic bone disease |
Quick Summary: Most Likely by Age 2
- Nutritional Vitamin D deficiency rickets - most common worldwide
- Hypoparathyroidism (congenital/DiGeorge) - especially if phosphate is high and PTH is low
- Pseudohypoparathyroidism - if PTH is high with dysmorphic features
- VDDR Type 1 - if rickets present but not responding to regular Vit D
- Hypomagnesemia - especially if refractory to IV calcium
Sources: - Brenner and Rector's The Kidney, Chap. 73 (Pediatric Hypocalcemia) and Chap. 18 (Diagnosis of Hypocalcemia) | - Rosen's Emergency Medicine, Chap. 31
This is a shared conversation. Sign in to Orris to start your own chat.