Anatomy of mediastinum for md exams 10 marks answer from fishman only
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the core content from Fishman's. Let me compile the comprehensive MD exam answer.
Anatomy of the Mediastinum
From: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Chapters 80 & 82)
Definition
The mediastinum is defined as the potential space between the two pleural cavities, bounded by:
| Border | Structure |
|---|---|
| Anterior | Sternum |
| Posterior | Vertebral column |
| Superior | Thoracic inlet |
| Inferior | Diaphragm |
| Lateral (×2) | Mediastinal pleural reflections |
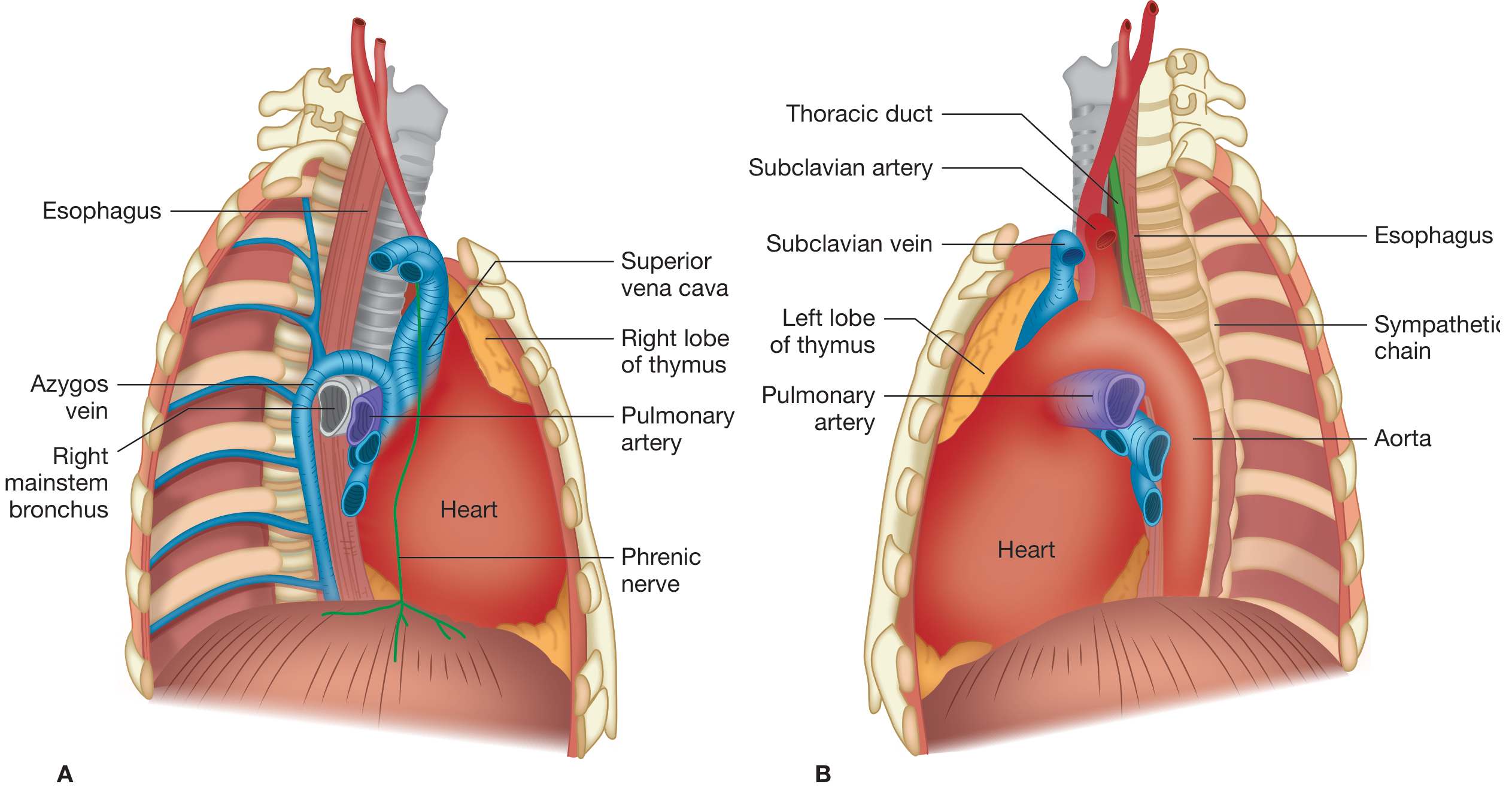
It is a potential space, not a true enclosed compartment - the major mediastinal structures (heart, great vessels, trachea, main bronchi, esophagus) are all closely related and connected by loose connective tissue. Also present are the thymus, lymph nodes, nerves, and fat.
Fishman's Ch. 80 (Tapias & Wright): "The mediastinum constitutes an anatomic space...that houses or borders vital structures of almost every major organ system, including the heart and great vessels of the circulatory system, the esophagus of the digestive system, major airways of the respiratory system, the thymus of the immune system, and the phrenic and vagus nerves of the neurologic system."
Communications
A clinically important feature: the mediastinum communicates freely with:
- The neck (superiorly) via fascial planes
- The retroperitoneum (inferiorly)
This means air, infection, or hemorrhage can track widely - e.g., a neck abscess can descend into the mediastinum causing descending necrotizing mediastinitis, and mediastinal gas can decompress into the neck.
Compartments
There is no consensus on the exact subdivisions, but the most widely used model is the three-compartment model (Shields, 1972), which makes both anatomic and surgical sense. Each compartment extends from the thoracic inlet superiorly to the diaphragm inferiorly.
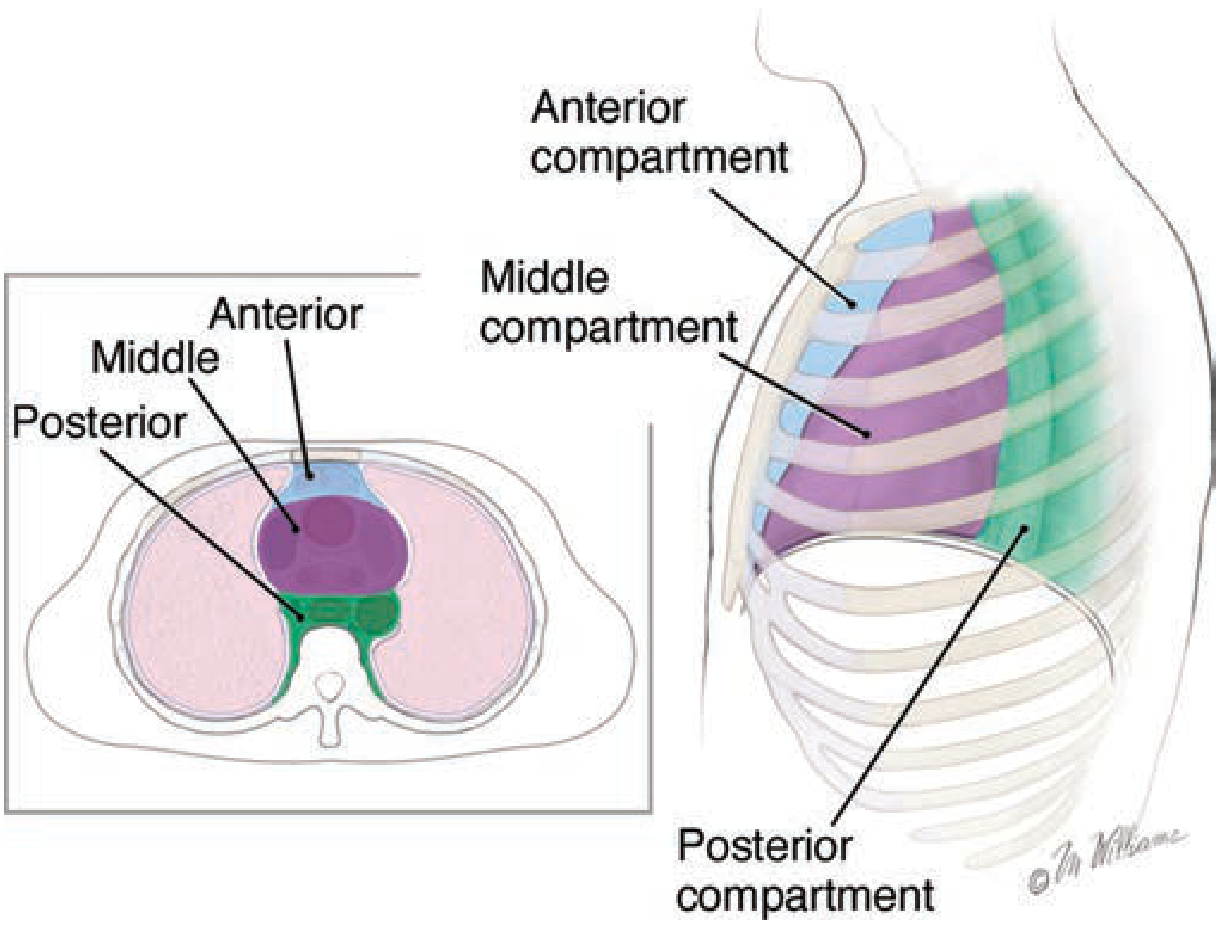
1. Anterior Compartment
- Boundaries: Bounded anteriorly by the sternum; posteriorly by the anterior surface of the pericardium and great vessels
- Contents:
- Thymus gland (most important structure)
- Pericardial fat
- Lymph nodes
- Internal mammary arteries and veins
2. Middle (Visceral) Compartment
- Boundaries: Anteriorly from the posterior limit of the anterior compartment; posteriorly to the anterior surface of the vertebral column (and posterior wall of the trachea). Extends only as high as the pericardial reflection.
- Contents:
- Heart and pericardium
- Superior and inferior vena cavae
- Ascending and transverse aorta
- Trachea and mainstem bronchi
- Esophagus
- Phrenic and vagus nerves
- Lymph nodes
3. Posterior Compartment (Paravertebral Sulcus)
- Boundaries: From the anterior surface of the vertebral column posteriorly to the anterior surface of the paravertebral ribs. Extends thoracic inlet to diaphragm.
- Contents:
- Descending aorta
- Azygos and hemiazygos veins
- Thoracic duct
- Esophagus (posterior portion)
- Sympathetic trunk
- Intercostal nerves (emerging from spinal canal)
- Lymph nodes
- Vagus nerves
Fishman's emphasis: "The pericardial sac is the only true compartment of the mediastinum, and it provides a strong barrier to infection."
Summary Table - Contents of Mediastinal Compartments (Table 80-1, Fishman's)
| Anterior | Middle (Visceral) | Posterior (Paravertebral) |
|---|---|---|
| Thymus gland | Pericardium | Azygos and hemiazygos veins |
| Pericardial fat | Heart | Thoracic duct |
| Lymph nodes | Trachea and main bronchi | Sympathetic trunk |
| Internal mammary vessels | Esophagus | Intercostal nerves |
| Aorta | Descending aorta | |
| Phrenic and vagus nerves | Lymph nodes | |
| Lymph nodes |
ITMIG Classification (CT-based, newer)
Fishman's also notes the International Thymic Malignancy Interest Group (ITMIG) classification based on CT anatomy, which divides the mediastinum into three similar compartments with different terminology:
| ITMIG (CT-based) | Traditional |
|---|---|
| Prevascular | Anterior |
| Visceral | Middle |
| Paravertebral | Posterior |
The thoracic inlet forms the superior border and the diaphragm forms the inferior border in this scheme.
Lymphatics
The mediastinal lymphatic system is complex and variable. Key points (Fishman's Ch. 80):
- Mediastinal lymph nodes are interconnected - involvement of one group frequently leads to involvement of others
- The mediastinum is covered in a dense network of lymphatic vessels and lymph nodes with no predictable anatomic boundaries
- Named nodal stations are somewhat arbitrary - they do not represent discrete, isolated structures
- The Naruke lymph node map (1978) is the widely accepted standard for communication of lymph node involvement, especially in staging of thoracic malignancies (particularly lung cancer)
Naruke Nodal Station Numbering:
- Single-digit stations (1-9): True mediastinal lymph nodes (N2 disease in lung cancer staging)
- Two-digit stations (10 and above): Lymph nodes within the pleural sac - these are extramediastinal (N1 disease)
Clinical Significance of Compartment Anatomy
Fishman's stresses that the primary clinical utility of compartment division is in generating a differential diagnosis for a mediastinal mass:
| Compartment | Most Common Mass ("4 T's of anterior") |
|---|---|
| Anterior | Thymoma, Teratoma/GCT, Thyroid goiter, Terrible lymphoma |
| Middle | Bronchogenic cyst, Pericardial cyst, Lymphoma, Vascular lesions |
| Posterior | Neurogenic tumors (most common in posterior), Foregut cysts |
In adults (combined series of 3017 patients cited in Fishman's Ch. 82):
- Thymomas and thymic cysts: 26.5% (most common)
- Neurogenic tumors: 20.2%
- Germ cell tumors: 13.8%
- Lymphomas: 12.7%
"One of the main advantages of dividing the mediastinum into compartments is the ability to generate a differential diagnosis for a mediastinal mass based on the structures that are contained within the compartment in which it arises." - Fishman's Ch. 82
Important caveat: Because the mediastinal compartments have no true anatomic barriers (except the pericardium), "diseases or masses of the mediastinum often extend from one compartment to another."
Summary for MD Exam
- Definition: Potential space between pleural cavities; sternum (ant) - vertebrae (post) - thoracic inlet (sup) - diaphragm (inf)
- Contents: Heart + great vessels, trachea + bronchi, esophagus, thymus, nerves, lymph nodes, fat - all in loose connective tissue
- Three compartments (Shields model): Anterior (thymus), Middle/Visceral (heart, trachea, vessels), Posterior/Paravertebral (azygos, thoracic duct, sympathetic chain)
- Only true compartment: Pericardial sac (barrier to infection)
- Communications: With neck and retroperitoneum via fascial planes - clinically important for spread of air/infection
- Lymphatics: Complex, interconnected; Naruke map used for lung cancer staging; single-digit = mediastinal (N2); double-digit = extramediastinal (N1)
- ITMIG CT classification: Prevascular / Visceral / Paravertebral
- Fishman's Pulmonary Diseases and Disorders, Ch. 80 (Tapias & Wright) - Nonneoplastic Disorders of the Mediastinum
- Fishman's Pulmonary Diseases and Disorders, Ch. 82 - Primary Benign and Malignant Neoplasms of the Mediastinum
This is a shared conversation. Sign in to Orris to start your own chat.