HELLP SYNDROME
Reading File
Finding Sources
Searching PubMed
"HELLP syndrome"[MeSH Terms] AND management
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
HELLP syndrome pathophysiology preeclampsia hemolysis liver
Reading File
Reading File
I now have comprehensive data from 6 authoritative textbooks. Let me compile the full answer.
HELLP Syndrome
Definition & Epidemiology
HELLP is an acronym for Hemolysis, Elevated Liver enzymes, Low Platelets. It is a severe form of preeclampsia driven by widespread microvascular injury and thrombotic microangiopathy (TMA).
| Statistic | Value |
|---|---|
| Incidence (all pregnancies) | 0.2–0.9% |
| In severe preeclampsia | 10–20% |
| Maternal mortality | 1–7.4% (up to 34% in severe cases) |
| Perinatal mortality | 7–34% (depends on gestational age) |
| Onset: 3rd trimester | Most common |
| Before 28 weeks | ~20% of cases |
| Postpartum onset | ~20–30% of cases |
| Without prior recognized preeclampsia | ~20% of cases |
— Harrison's Principles of Internal Medicine 22E (2025), p. 2490; Sleisenger & Fordtran, p. 40
Pathophysiology
HELLP shares the fundamental pathophysiology of preeclampsia — abnormal placentation leads to widespread endothelial dysfunction. Key mechanisms:
- Microvascular injury → platelet activation and consumption → thrombocytopenia
- Microangiopathic hemolytic anemia (MAHA) → RBC fragmentation (schistocytes) as cells shear through damaged microvasculature
- Hepatic ischemia → periportal hemorrhage, sinusoidal fibrin deposition, cellular necrosis → elevated transaminases, RUQ pain
- Complement pathway dysfunction is common (30–40% of patients have complement gene mutations)
- Elevated inflammatory markers: CRP, IL-1Ra, IL-6, and soluble HLA-DR (higher than preeclampsia alone)
- Elevated FLT1 (VEGF receptor 1) and endoglin (antiangiogenic factors)
— Harrison's 22E, p. 2490; Brenner & Rector's The Kidney
Clinical Features
Symptoms (often nonspecific — easily misdiagnosed as cholecystitis, hepatitis, gastroenteritis):
- Epigastric or right upper quadrant pain (most classic)
- Nausea and vomiting
- Headache, blurred vision
- Malaise ("viral syndrome" appearance)
- Shoulder/back pain (from hepatic subcapsular hematoma irritating the diaphragm)
Signs:
- Hypertension — may be absent in up to a subset of patients
- Edema
- Jaundice (in hemolysis-dominant cases)
- Tenderness on RUQ palpation
⚠️ A pregnant woman at >20 weeks of gestation OR up to 7 days postpartum with abdominal pain must be evaluated for HELLP syndrome. — Tintinalli's Emergency Medicine
Diagnostic Criteria
ACOG Task Force Criteria (Recommended Standard)
- Hemolysis + at least 2 of:
- Schistocytes and burr cells on peripheral smear
- Serum bilirubin ≥ 1.2 mg/dL
- Low serum haptoglobin
- Severe anemia unrelated to blood loss
- Elevated liver enzymes: AST > 70 IU/L or > 2× upper limit of normal
- Thrombocytopenia: Platelet count < 100,000/μL
Tennessee Classification
| Criterion | Threshold |
|---|---|
| Hemolysis (MAHA) | Abnormal smear, low haptoglobin, elevated LDH |
| LDH | > 600 IU/L or > 2× ULN |
| AST | > 70 IU/L or > 2× ULN |
| Bilirubin | > 1.2 mg/dL |
| Platelets | < 100,000/μL |
"Incomplete HELLP" = only 1–2 of these abnormalities present.
Mississippi Triple-Class Classification (by platelet nadir)
| Class | Platelet Count Nadir |
|---|---|
| Class I (most severe) | ≤ 50,000/mm³ |
| Class II | > 50,000 and ≤ 100,000/mm³ |
| Class III | > 100,000 and ≤ 150,000/mm³ |
— Sleisenger & Fordtran GI and Liver Disease, p. 40
Key Laboratory Investigations
| Test | Finding |
|---|---|
| CBC + peripheral smear | Schistocytes (microangiopathic picture) |
| Platelet count | < 100,000/μL (< 150,000 suspicious) |
| LDH | > 600 U/L (hemolysis marker) |
| AST/ALT | Elevated (< 500 U/L typical; can reach > 1000 U/L) |
| Serum bilirubin | > 1.2 mg/dL (total) |
| Haptoglobin | Low (consumed by hemolysis) |
| Serum creatinine / BUN | Normal to elevated |
| Coagulation profile (PT, aPTT, fibrinogen) | Abnormal in DIC |
| ADAMTS13 | Reduced 30–60% (but NOT < 10% as in TTP) |
| Urine protein | Proteinuria present in 86–100% |
Differential Diagnosis
HELLP must be distinguished from other thrombotic microangiopathies of pregnancy:
| Feature | HUS/TTP | HELLP | AFLP |
|---|---|---|---|
| Hemolytic anemia | +++ | ++ | ± |
| Thrombocytopenia | +++ | ++ | ± |
| Coagulopathy | − | ± | + |
| CNS symptoms | ++ | ± | ± |
| Renal failure | +++ | + | ++ |
| Hypertension | ± | +++ | ± |
| Proteinuria | ± | ++ | ± |
| Elevated AST | ± | ++ | +++ |
| Elevated bilirubin | ++ | + | +++ |
| Ammonia | Normal | Normal | High |
| Effect of delivery | None | Recovery | Recovery |
| Management | Plasma exchange | Supportive + delivery | Supportive + delivery |
Key distinguishing points:
- TTP: ADAMTS13 < 10% (vs. 30–60% reduction in HELLP)
- AFLP: hepatic failure + encephalopathy + coagulopathy + hyperammonemia — rare in HELLP
- Antiphospholipid syndrome: elevated risk of HELLP; check aPL antibodies
- Antithrombin III: decreased in HELLP, not in TTP
- LDH:AST ratio: 13:1 in HELLP + preeclampsia vs. 29:1 without preeclampsia
— Brenner & Rector's The Kidney, Table 48.4; Harrison's 22E
Complications
Maternal
| Complication | Approximate Frequency |
|---|---|
| Renal failure (AKI) | 5–50% |
| Eclampsia | ~6% |
| Placental abruption | ~10% |
| Pulmonary edema | ~10% |
| DIC | ~8% |
| Subcapsular hepatic hematoma | ~1% of HELLP cases |
| Spontaneous hepatic rupture | Rare but catastrophic |
| Cerebral infarction / hemorrhage | Rare |
| Purtscher-like retinopathy | Rare |
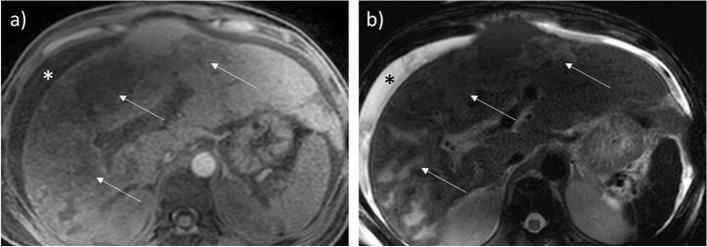
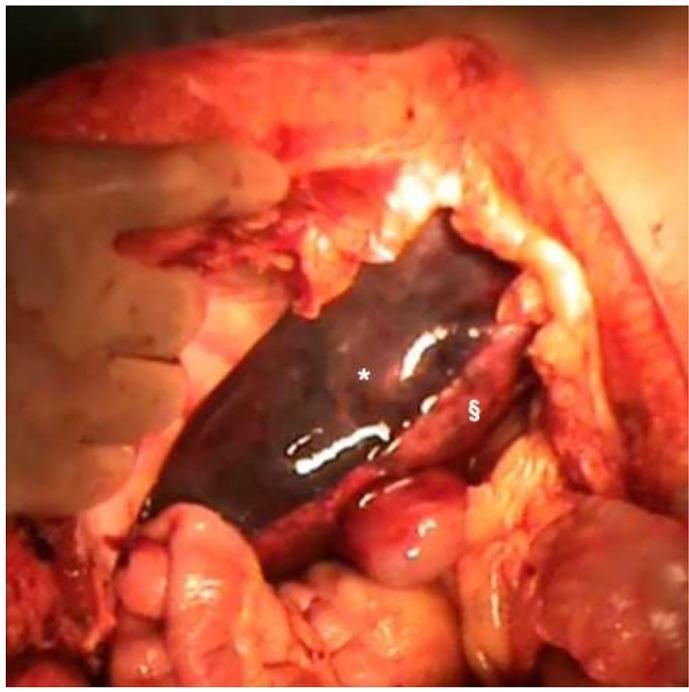
Hepatic Rupture — Special Consideration
-
95% of liver ruptures in pregnancy involve HELLP
- Right lobe predominantly affected
- Presents with RUQ pain → hemorrhagic shock
- Shoulder pain from diaphragmatic irritation by hemoperitoneum
- Imaging: bedside US → CT/MRI for confirmation
- May require surgical intervention or even liver transplantation
Fetal/Neonatal
- Preterm birth
- Fetal growth restriction
- Fetal demise
- Neonatal thrombocytopenia
Management
Immediate Stabilization (Emergency Setting)
- IV Magnesium Sulfate — seizure prophylaxis (4–6 g bolus over 20–30 min, then 2 g/hr infusion)
- Monitor: patellar reflexes, respiratory rate, urine output
- Antidote for toxicity: calcium gluconate 1 g IV
- Antihypertensive therapy for BP > 160/110 mmHg:
| Drug | Mechanism | Onset | Dose |
|---|---|---|---|
| Labetalol | α + β blockade | 5 min | 20 mg IV, then 40–80 mg q10min (max 300 mg) |
| Hydralazine | Arterial vasodilator | 20 min | 5 mg IV, repeat q20min (max 20 mg IV) |
| Nifedipine | Calcium channel blocker | 10–20 min | 10 mg PO, repeat in 30 min |
- Correct coagulopathy — transfuse platelets/FFP as clinically indicated
- Transfer to tertiary center with high-risk obstetrics if not available locally
Definitive Treatment: Delivery
- ≥ 34 weeks gestation: prompt delivery is the definitive treatment
- < 34 weeks without serious complications: consider antenatal corticosteroids (betamethasone) to accelerate fetal lung maturity, then deliver
- Serious maternal/fetal complications at any gestational age: prompt delivery regardless
Postpartum
- Laboratory abnormalities typically resolve within 48–72 hours after delivery (may worsen before improving)
- Continue magnesium sulfate for ≥ 24 hours postpartum
- Monitor LFTs, CBC, creatinine until definite improvement
- HELLP may develop de novo postpartum (up to 30% of cases) — maintain vigilance
Treatments with Limited/No Evidence
- Plasma exchange: no benefit in HELLP itself; use only if TTP cannot be excluded
- Eculizumab: reported effective in small numbers; dosing/indications undetermined
- Maternal corticosteroids: therapeutic role remains controversial (not routinely recommended per nephrology guidelines)
Renal Involvement
Renal failure occurs in ~50% of HELLP patients. Histology shows TMA with endothelial cell swelling and capillary lumen occlusion (luminal thrombi typically absent, but become more common in severe eclampsia). AKI etiology involves both preeclamptic glomerulopathy and acute tubular necrosis.
— Harrison's 22E, p. 2490; Comprehensive Clinical Nephrology 7E
Recurrence Risk
Women with HELLP have elevated risk in future pregnancies. Combination first-trimester screening (maternal risk factors + uterine artery Doppler + PlGF + sFlt-1) can predict high-risk pregnancies; low-dose aspirin prophylaxis is recommended for high-risk women.
Imaging: Hepatic Complications of HELLP

Key Takeaways
- HELLP = Hemolysis + Elevated Liver Enzymes + Low Platelets — a severe TMA of pregnancy
- 20% of cases have no preceding hypertension or proteinuria — do not miss it
- 30% develop postpartum — maintain vigilance after delivery
- Distinguished from TTP by ADAMTS13 (30–60% reduction, not < 10%), and from AFLP by absence of encephalopathy/hyperammonemia
- Definitive treatment = delivery; magnesium sulfate + antihypertensives are stabilizing measures
- Hepatic rupture is a rare but life-threatening complication requiring emergency surgery
- In < 34 weeks with stable mother: corticosteroids first, then deliver
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Brenner & Rector's The Kidney | Creasy & Resnik's Maternal-Fetal Medicine | Sleisenger & Fordtran's GI and Liver Disease | Tintinalli's Emergency Medicine | Comprehensive Clinical Nephrology 7E
This is a shared conversation. Sign in to Orris to start your own chat.