stroke as per harrison
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from Harrison's 22E on stroke. Let me compile the full detailed response.
Stroke - Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Authors: Wade S. Smith, J. Claude Hemphill, III
Definition and Epidemiology
A stroke (cerebrovascular accident) is defined as the abrupt onset of a neurologic deficit attributable to a vascular cause. The definition is clinical; brain imaging supports but does not make the diagnosis.
- Stroke is the second leading cause of death worldwide - 7.1 million deaths in 2020
- Nearly 7 million Americans age 20+ report having had a stroke
- Prevalence is expected to rise by 3.4 million adults (to 4% of the entire adult population) in the next decade
- Age-standardized death rate has fallen ~15% due to better prevention and treatment
- Overall disease burden continues to climb as populations age
Types of Stroke
- Ischemic stroke (~87%) - caused by reduction in blood flow
- Hemorrhagic stroke - bleeding directly into or around the brain
TIA vs. Stroke:
- TIA: all neurologic signs and symptoms resolve within 24 h without evidence of brain infarction on imaging
- Stroke: neurologic signs/symptoms last >24 h or brain infarction is demonstrated on imaging
Pathophysiology of Ischemic Stroke
- Blood flow to zero kills brain tissue (neurons, dendrites, axons, glia) within 4-10 minutes
- CBF <16-18 mL/100 g tissue/min causes infarction
- The ischemic penumbra - surrounding tissue at risk - is the target of acute therapy
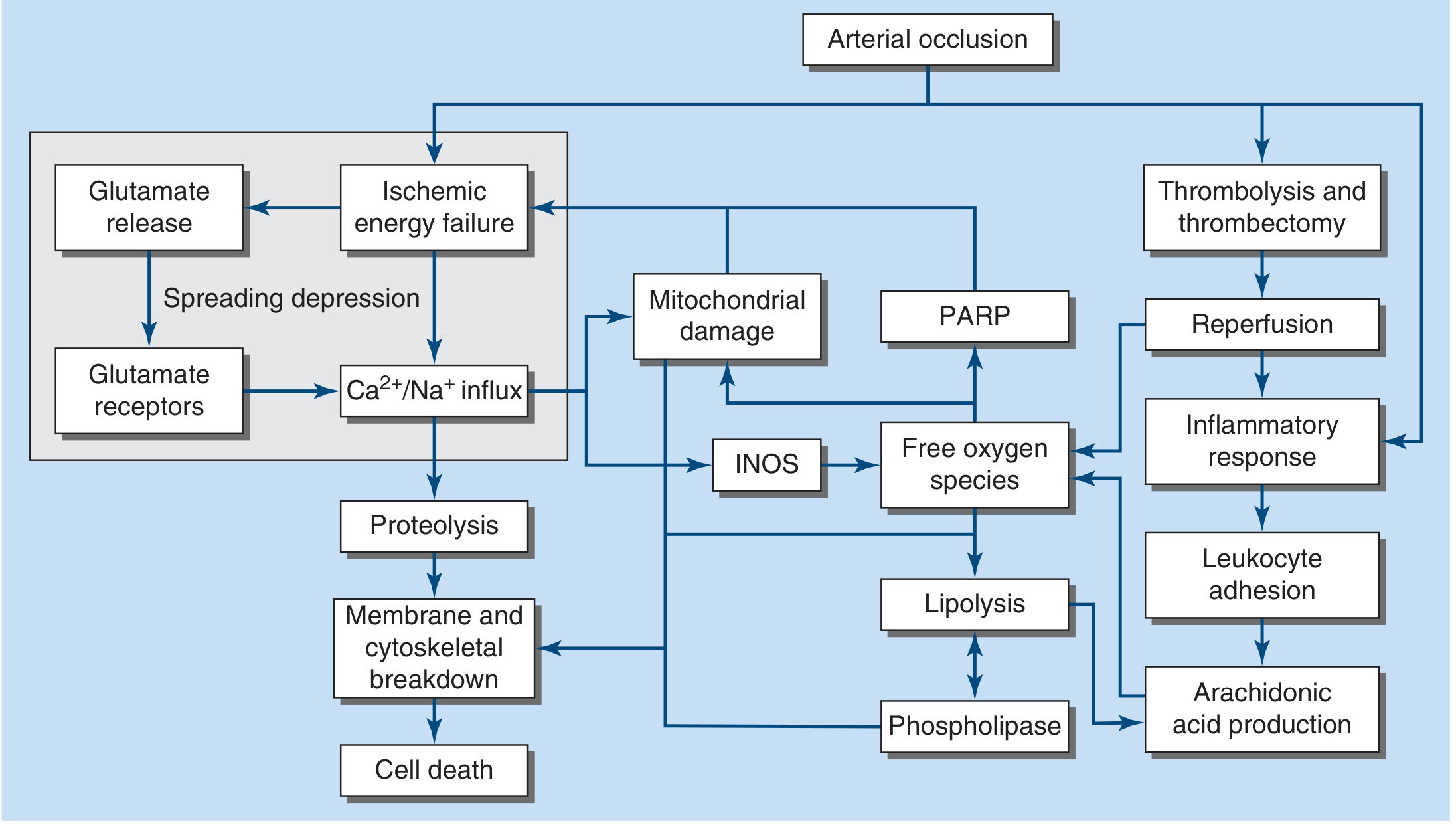
Cascade after arterial occlusion:
- Ischemic energy failure → glutamate release → glutamate receptor activation
- Ca²⁺/Na⁺ influx → proteolysis → membrane and cytoskeletal breakdown → cell death
- Mitochondrial damage → free oxygen species → lipolysis → phospholipase → arachidonic acid production
- iNOS activation → more free oxygen species
- PARP activation
- Reperfusion (after thrombolysis/thrombectomy) → inflammatory response → leukocyte adhesion
Approach to the Patient - FAST
FAST acronym (for the lay public):
- Facial weakness
- Arm weakness
- Speech abnormality
- Time (treatments are highly time sensitive)
Nearly 85% of ischemic stroke patients have hemiparesis.
Mimics to exclude: seizure, intracranial tumor, metabolic derangements (hypoglycemia, hyponatremia), sepsis, encephalitis, multiple sclerosis, migraine.
Stroke Syndromes
Anterior Circulation
Middle Cerebral Artery (MCA)
- Most common cause: embolus (artery-to-artery, cardiac, or cryptogenic)
- M1 segment gives rise to lenticulostriate arteries supplying putamen, globus pallidus, posterior limb of internal capsule, caudate
- Complete MCA occlusion: contralateral hemiplegia, hemianesthesia, homonymous hemianopia, ipsilateral gaze preference
- Dominant hemisphere: global aphasia
- Non-dominant hemisphere: anosognosia, constructional apraxia, neglect
- Superior division: Broca's (non-fluent) aphasia + right arm weakness
- Inferior division: Wernicke's (fluent) aphasia + right homonymous hemianopia
Anterior Cerebral Artery (ACA)
- Supplies medial frontal and parietal lobes
- Occlusion: contralateral leg > arm weakness, frontal lobe signs (abulia, incontinence)
Posterior Circulation
Posterior Cerebral Artery (PCA)
- Supplies midbrain, thalamus, temporal and occipital lobes
- P1 occlusion (proximal): thalamic syndromes, midbrain signs
- P2 occlusion: contralateral homonymous hemianopia (macular sparing), cortical blindness if bilateral
Basilar Artery
- "Locked-in syndrome" with bilateral ventral pontine infarction
- Occlusion: coma, quadriplegia, cranial nerve palsies
Vertebral Artery / PICA
- Lateral medullary (Wallenberg) syndrome: ipsilateral facial numbness, Horner syndrome, ataxia; contralateral limb pain/temperature loss; dysphagia, hoarseness
Small-Vessel (Lacunar) Stroke
- Accounts for ~20% of all strokes
- Caused by atherothombotic or lipohyalinotic occlusion of 30-300 µm penetrating branches of MCA, circle of Willis, basilar artery
- Principal risk factors: hypertension and age
- Infarct size: 3 mm to 2 cm
Classic lacunar syndromes:
- Pure motor hemiparesis - infarct in posterior limb of internal capsule or pons (face + arm + leg all involved)
- Pure sensory stroke - infarct in ventral thalamus
- Ataxic hemiparesis - infarct in ventral pons or internal capsule
- Dysarthria-clumsy hand - infarct in ventral pons or genu of internal capsule
Recovery from small-vessel strokes tends to be more rapid and complete than large-vessel strokes. However, large-vessel sources can initially present as small-vessel infarction, so carotid/cardiac workup should not be completely abandoned.
Etiology of Ischemic Stroke
Three major mechanisms (Fig 438-4):
- Embolism - cardiac sources (AF, mural thrombus, valvular disease) or artery-to-artery (carotid plaque)
- In-situ thrombosis - typically small penetrating arteries
- Hypoperfusion - flow-limiting stenosis causing "watershed" ischemia
| Common Causes | Uncommon Causes |
|---|---|
| Lacunar (small vessel) | Protein C/S deficiency |
| Large-vessel thrombosis | Antiphospholipid syndrome |
| Dehydration | Factor V Leiden mutation |
| Atrial fibrillation | Sickle cell anemia |
| Mural thrombus (post-MI) | Homocysteinemia |
| Dilated cardiomyopathy | TTP, DIC |
| Mitral stenosis | Vasculitis |
| Mechanical heart valve | CADASIL |
| Bacterial endocarditis | Fabry disease |
| Carotid atherosclerosis | Migraine with aura |
Cardioembolic stroke accounts for ~20% of ischemic strokes. The most important causes are atrial fibrillation and carotid atherosclerosis.
Acute Treatment of Ischemic Stroke
Step 1: Imaging
- Emergency noncontrast CT head to differentiate ischemic vs. hemorrhagic stroke
- Features favoring hemorrhage: depressed consciousness, very high BP, worsening after onset
- Features favoring ischemia: maximal deficit at onset, or deficit that remits
6 Treatment Categories:
- Medical support
- IV thrombolysis
- Endovascular revascularization (thrombectomy)
- Antithrombotic treatment
- Neuroprotection
- Stroke centers and rehabilitation
Medical Support
- Optimize cerebral perfusion in ischemic penumbra
- Prevent complications: pneumonia, UTI, skin breakdown, DVT/PE
- DVT prophylaxis: subcutaneous heparin or pneumatic compression stockings
- BP management:
- Reduce if BP >220/120 mmHg
- Reduce if BP >185/110 mmHg before thrombolysis
- Avoid routine lowering below these thresholds (risks worsening outcome)
- β-blockers (e.g., esmolol) useful when managing competing cardiac demands
- Treat fever (detrimental to outcomes)
IV Thrombolysis (tPA)
- Alteplase (rt-PA) 0.9 mg/kg IV (max 90 mg); 10% as bolus, rest over 60 min
- Window: within 3-4.5 hours of symptom onset
- Benefit is strongly time-dependent: "time is brain"
- Contraindications include hemorrhage on CT, recent surgery, coagulopathy, and BP >185/110 (must be controlled before giving)
Endovascular Thrombectomy
- For large-vessel occlusion (MCA, ICA, basilar)
- Extended window up to 24 hours with perfusion imaging selection
- Combined with tPA when eligible
Antithrombotic Therapy (Acute)
- Aspirin 160-325 mg within 48 h of ischemic stroke (reduces recurrence risk by ~1%)
- Not a substitute for thrombolysis
Stroke Prevention
Antiplatelet Agents
- Aspirin: acetylates platelet COX → irreversibly inhibits thromboxane A2 (platelet aggregating) while transiently inhibiting prostacyclin; low-dose preferred
- Clopidogrel: blocks ADP receptor (P2Y12) → inhibits glycoprotein IIb/IIIa activation; CAPRIE trial showed marginal superiority over aspirin
- Aspirin + extended-release dipyridamole: combination option
- Ticagrelor + aspirin: shown to reduce secondary stroke risk; not superior as monotherapy
Dual antiplatelet therapy (DAPT) - short term:
- Clopidogrel 300 mg load then 75 mg/d + aspirin 75 mg/d for the first 21 days after TIA or minor ischemic stroke → superior to aspirin alone (8.2% vs 11.7% 90-day stroke risk); benefit limited to non-CYP2C19 poor metabolizers
- Long-term DAPT is NOT recommended (increased hemorrhage and mortality in SPS3, MATCH, CHARISMA trials)
Anticoagulation
- Warfarin (or DOAC) for cardioembolic stroke due to atrial fibrillation
- Target INR 2-3 for warfarin
- DOACs (dabigatran, rivaroxaban, apixaban) preferred over warfarin in non-valvular AF
- Not routinely recommended for non-cardioembolic stroke
Risk Factor Modification
- Hypertension control: most important modifiable risk factor
- Statin therapy (LDL reduction)
- Smoking cessation
- Diabetes management
- Carotid endarterectomy or stenting for high-grade symptomatic carotid stenosis (>70%)
Stroke Centers and Rehabilitation
- Stroke units improve outcomes compared to general medical wards
- Multidisciplinary teams (neurology, nursing, PT, OT, speech therapy)
- Early rehabilitation initiated within 24-48 h
- Rehabilitation goals: maximize recovery in the ischemic penumbra that has not yet infarcted, and compensatory strategies for infarcted tissue
Less Common Causes
- Hypercoagulable states: protein C/S deficiency, antiphospholipid syndrome - more commonly cause cortical vein/sinus thrombosis than arterial stroke
- CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy): hereditary small-vessel disease
- Vasculitis (CNS, systemic)
- Arterial dissection (carotid, vertebral): especially in young patients with neck trauma or spontaneous; Horner syndrome + ipsilateral neck pain is a clue
- Fabry disease: X-linked lysosomal storage disorder; stroke in young patients
- Sickle cell disease
- Drug use: cocaine, amphetamines (vasospasm, accelerated atherosclerosis)
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 438 - Cerebrovascular Diseases. Authors: Wade S. Smith, J. Claude Hemphill, III.
This is a shared conversation. Sign in to Orris to start your own chat.