Explain about blood pressure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content from authoritative medical textbooks. Here is the full explanation:
Blood Pressure
What Is Blood Pressure?
Blood pressure is the force exerted by blood against any unit area of the vessel wall. It is almost universally measured in millimeters of mercury (mm Hg) - a standard dating back to Poiseuille's mercury manometer (1846). A reading of 100 mm Hg means the force is sufficient to push a column of mercury 100 mm high against gravity. Pressures can also be expressed in cm H₂O (1 mm Hg = 1.36 cm H₂O).
- Guyton and Hall Textbook of Medical Physiology
The Core Formula
BP = Cardiac Output (CO) × Peripheral Vascular Resistance (PVR)
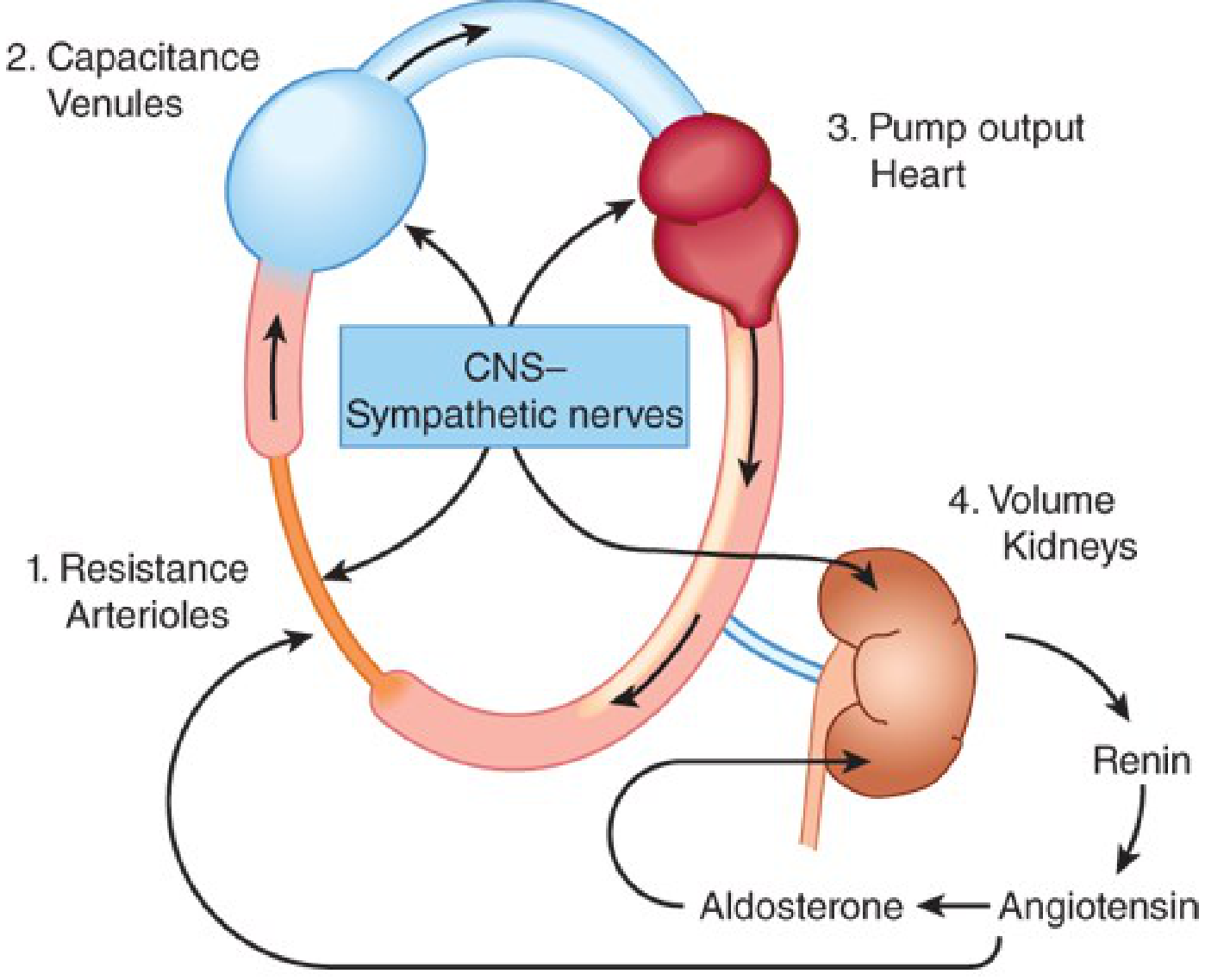
Blood pressure is maintained at every moment by the interaction between cardiac output and peripheral vascular resistance. Four anatomic sites exert control:
- Arterioles - resistance vessels
- Postcapillary venules - capacitance vessels
- The heart - pump output
- The kidneys - intravascular fluid volume regulation
The CNS sympathetic nerves coordinate all four sites. This is illustrated below:
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Systolic, Diastolic, and Mean Arterial Pressure
| Term | Definition |
|---|---|
| Systolic BP (SBP) | Peak pressure during cardiac contraction (ventricular systole) |
| Diastolic BP (DBP) | Lowest pressure during cardiac relaxation (diastole) |
| Pulse Pressure | SBP - DBP |
| Mean Arterial Pressure (MAP) | (Diastolic × 2 + Systolic) ÷ 3 |
MAP is considered more accurate than systolic pressure alone in determining end-organ perfusion.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Classification of Blood Pressure
Based on averages of two or more readings on two or more separate occasions, in adults not on antihypertensive therapy:
| Category | Systolic (mm Hg) | Diastolic (mm Hg) |
|---|---|---|
| Optimal | < 120 | and < 80 |
| Normal | 120-129 | and/or 80-84 |
| High Normal | 130-139 | and/or 85-89 |
| Grade 1 Hypertension | 140-159 | and/or 90-99 |
| Grade 2 Hypertension | 160-179 | and/or 100-109 |
| Grade 3 Hypertension | ≥ 180 | and/or > 110 |
| Isolated Systolic Hypertension | ≥ 140 | and < 90 |
When systolic and diastolic readings fall in different categories, the higher category applies.
- Park's Textbook of Preventive and Social Medicine
Regulation of Blood Pressure
Blood pressure is controlled via two main time-dependent mechanisms:
1. Short-Term (Moment-to-Moment) - Baroreceptor Reflex
Baroreceptors in the carotid sinus and aortic arch detect vessel wall stretch (which reflects arterial pressure). When pressure falls:
- Baroreceptor firing decreases
- CNS sympathetic outflow increases
- This constricts arterioles (raises PVR), stimulates the heart (raises CO), and constricts capacitance veins (raises venous return)
- Blood pressure is restored
When a person stands up, blood pools below the heart, baroreceptors sense the drop in stretch, and this reflex fires within seconds to maintain cerebral perfusion.
2. Long-Term - Renin-Angiotensin-Aldosterone System (RAAS) and Natriuretic Peptides
-
The kidneys release renin when perfusion pressure falls
-
Renin converts angiotensinogen → Angiotensin I → (via ACE) → Angiotensin II
-
Angiotensin II causes vasoconstriction and stimulates aldosterone release
-
Aldosterone promotes Na⁺ and water retention → expands blood volume → raises BP
-
Atrial and brain natriuretic peptides (ANP/BNP) counter this by promoting sodium excretion and vasodilation
-
Frameworks for Internal Medicine; Katzung's Basic and Clinical Pharmacology, 16th Ed.
Role of the Kidneys
The kidney plays a central role in blood pressure regulation. Even mild kidney damage can raise blood pressure through:
- Salt and water retention (volume expansion)
- Sympathetic overactivity
- RAAS activation
- Accumulation of endogenous vasopressors
In turn, hypertension damages the kidney further (arterial hyalinosis, vascular stiffening, declining GFR) - creating a vicious cycle. Data from kidney donors show that each 10 mL/min/1.73 m² reduction in GFR corresponds to approximately a 5 mm Hg rise in systolic BP.
- Brenner and Rector's The Kidney
Factors That Affect Blood Pressure
| Factor | Effect on BP |
|---|---|
| Age | BP rises with age (arterial stiffening) |
| Body position | Lower when supine, higher when standing initially |
| Exercise | Transiently increases SBP |
| Stress/Emotion | Activates sympathetic system, raises BP |
| Obesity | Raises BP (increased CO and RAAS activation) |
| Salt intake | High intake raises BP in salt-sensitive individuals |
| Alcohol and smoking | Both associated with raised BP |
Errors in Blood Pressure Measurement
Three main sources of error exist:
- Observer errors - poor hearing acuity, misinterpretation of Korotkoff sounds
- Instrumental errors - leaking valves, wrong cuff size (too small a cuff gives falsely HIGH readings)
- Subject errors - recent exercise, emotional state, posture, recent caffeine/smoking
- Park's Textbook of Preventive and Social Medicine
Consequences of Abnormal Blood Pressure
High blood pressure (hypertension) is log-linearly associated with:
- Coronary artery disease
- Ischemic and hemorrhagic stroke
- Congestive heart failure
- Chronic kidney disease progression
Organ damage does not always correlate directly with blood pressure level - markedly high pressures can exist without organ damage, and organ damage can occur with only moderately elevated pressures. The presence of organ damage increases cardiovascular risk at any given BP level.
- Brenner and Rector's The Kidney; Park's Textbook of Preventive and Social Medicine
Low blood pressure (hypotension) can result from:
- Volume depletion (hemorrhage, dehydration)
- Reduced cardiac output (heart failure)
- Vasodilation (sepsis, anaphylaxis, certain drugs)
Summary
Blood pressure is a dynamic, tightly regulated physiological variable. Its regulation involves a rapid neural arc (baroreceptors), a slower hormonal arc (RAAS), and the kidney as the ultimate long-term volume and pressure regulator. Both too-high and too-low blood pressure carry serious clinical consequences, making accurate measurement and monitoring central to patient care.
This is a shared conversation. Sign in to Orris to start your own chat.