C2 dermatome distribution
Reading File
Searching the Web
C2 dermatome distribution anatomy
Finding Sources
Loading Image
Reading File
Reading File
Here is a complete overview of the C2 dermatome distribution, drawing from authoritative neurology and physiology textbooks.
C2 Dermatome Distribution
Cutaneous Territory
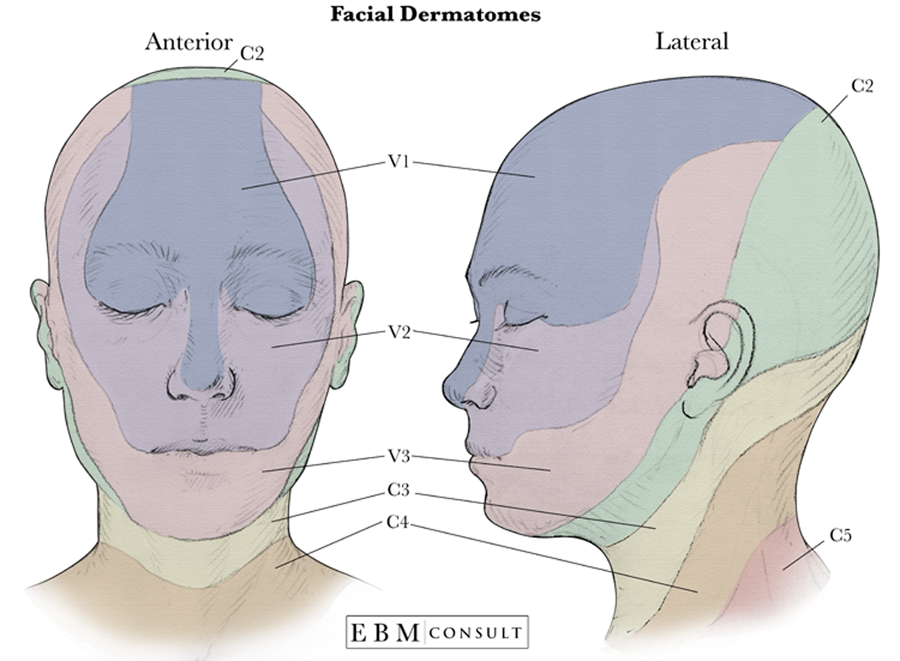
The C2 dermatome covers the scalp posterior to the interaural line - essentially a "skullcap" of skin running from the occiput (subocciput) up to the vertex, about 6-8 cm wide paramedially. On the lateral view, C2 also covers the skin behind the ear and the upper posterior neck.
Key boundaries:
- Anterior: the interaural line (an imaginary line connecting the two ear openings) separates C2 (posterior) from the trigeminal nerve V1 territory (anterior scalp)
- Superior: extends to the vertex of the skull
- Inferior: blends with C3, which takes over at the lower occiput, angle of the jaw, and upper neck
- Lateral: behind the ear (the area in front of and around the ear is covered by the trigeminal and C3)
Unique Clinical Significance
C2 has an important distinction from all other spinal roots: severing the C2 dorsal root alone produces a genuine patch of analgesia on the back of the head, because neither C3 below nor the trigeminal nerve (CN V) above innervates this zone. In virtually every other dermatome, cutting a single root causes only reduced sensation due to overlap from adjacent roots. - Medical Physiology, p. 420
Nerves Carrying C2 Sensation
| Nerve | Branch | Territory |
|---|---|---|
| Greater occipital nerve | Dorsal ramus of C2 | Posterior scalp from occiput to vertex |
| Lesser occipital nerve | Ventral ramus (via cervical plexus) | Posterior auricle, scalp behind ear |
| Greater auricular nerve | Ventral ramus (C2-C3) | Lower auricle, skin over parotid |
Motor Supply at C2
C2 motor fibers help innervate muscles involved in head and neck movement, including:
-
Longus capitis, rectus capitis, obliquus capitis
-
Longissimus capitis and cervicis
-
Semispinalis, multifidi, rotatores, intertransversarii
-
Sternocleidomastoid (C2 contributes alongside the spinal accessory nerve/CN XI)
-
Localization in Clinical Neurology, 8e, p. 227
Clinical Correlation
- A C2 lesion (e.g., atlantoaxial pathology, high cervical disc, foramen magnum tumor) produces:
- Occipital neuralgia - severe pain radiating from the occiput to the vertex, often described as electric-shock or stabbing
- Sensory loss or dysesthesia in the posterior scalp
- The C2 pain dermatome spans an occipital-parietal strip 6-8 cm wide, from the subocciput to the vertex - Bradley and Daroff's Neurology, p. 2882
- C2 pathology must be distinguished from migraine and cervicogenic headache, as it directly contributes to the trigeminocervical complex (convergence of C1-C3 afferents with trigeminal nucleus caudalis)
Summary Map
Vertex of skull
↑
[C2 zone] ← posterior scalp (occiput → vertex)
↓
Subocciput
+ skin behind ear
↓
[C3 zone] → lower occiput, angle of jaw, upper neck
The C2 dermatome is the highest true cutaneous spinal dermatome - C1 has no dorsal root in most individuals and therefore no dermatome.
3rd nerve relation to tentorium
Finding Sources
Searching the Web
CN III oculomotor nerve relationship tentorium cerebelli anatomy uncal herniation
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Here is a detailed account of the CN III relationship to the tentorium cerebelli, compiled from multiple authoritative neurology and neuroanatomy textbooks.
CN III (Oculomotor Nerve) Relation to the Tentorium Cerebelli
Anatomical Course Through/Around the Tentorium
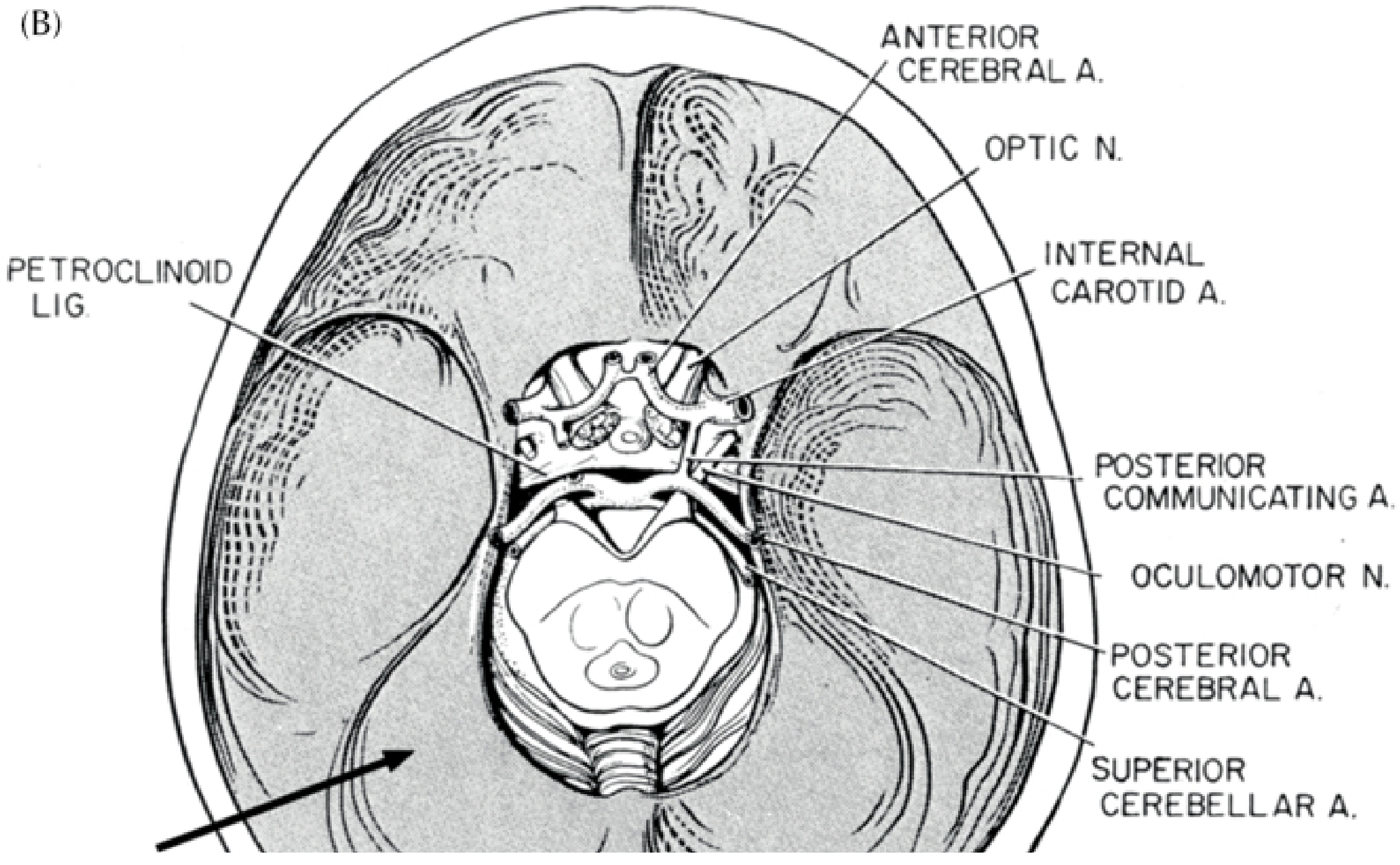
The oculomotor nerve follows a precise path in which the tentorium is a key landmark at two distinct points:
1. Origin at the midbrain
CN III exits the ventral surface of the midbrain (at the level of the interpeduncular fossa) between the superior cerebellar arteries (below) and the diverging posterior cerebral arteries (above).
2. Subarachnoid course along the tentorial edge
After leaving the midbrain, the nerve runs anteriorly in the subarachnoid space, traveling along the medial edge of the temporal lobe - which is the undersurface of the free (inner) edge of the tentorium. It crosses over the posterior cerebral artery and runs alongside the posterior communicating artery.
3. Penetrating the tentorium / entering the cavernous sinus
The nerve then enters the anterior edge of the tentorium cerebelli (pierces the dural roof), passes through the dura at the petroclinoid ligament, and enters the lateral wall of the cavernous sinus - where it runs above CN IV (trochlear nerve).
4. Exit
It leaves the cranial cavity through the superior orbital fissure.
- Gray's Anatomy for Students, p. 1037
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 201
Diagram - CN III and Its Vascular/Tentorial Relations
Why This Relationship Matters: Uncal Herniation
The fact that CN III runs along the medial free edge of the tentorium makes it exquisitely vulnerable to compression when the medial temporal lobe (uncus) herniates downward through the tentorial notch.
Sequence of events in uncal herniation:
- A supratentorial mass (hemorrhage, tumor, edema) increases intracranial pressure
- The uncus of the temporal lobe is pushed medially and downward over the free edge of the tentorium
- CN III is trapped between the uncus above and the tentorial edge below
- The pupillodilator (parasympathetic) fibers run on the dorsal surface of CN III - they are hit first
- This produces an ipsilateral fixed dilated pupil ("blown pupil") - the earliest sign
- As herniation progresses: complete CN III palsy (ptosis, ophthalmoplegia), then midbrain compression, hemiplegia, and coma
The classic clinical triad is: blown pupil + hemiplegia + coma - Neuroanatomy through Clinical Cases, 3rd Ed., p. 171
The dilated pupil is ipsilateral to the lesion in ~85% of cases. The rarer contralateral blown pupil (Kernohan's phenomenon) occurs when the midbrain is pushed so far that it compresses the opposite tentorial edge, injuring the contralateral CN III.
Why Parasympathetic Fibers Are Hit First
The parasympathetic (pupilloconstrictor) fibers from the Edinger-Westphal nucleus travel on the outer dorsal surface of CN III. External compression (by the uncus or a posterior communicating artery aneurysm) damages these superficial fibers before the central motor fibers. This is in contrast to ischemic CN III palsy (e.g., diabetic), which damages the central motor fibers first and spares the pupil.
| Cause | Pupil |
|---|---|
| Compression (uncal herniation, PComm aneurysm) | Dilated, fixed (parasympathetics hit first) |
| Ischemic (diabetes, hypertension) | Pupil-sparing (central motor fibers affected) |
Additional Vascular Vulnerability at the Tentorial Notch
At the same zone, the posterior cerebral arteries pass upward through the tentorial notch, and can be compressed during uncal herniation - causing occipital lobe infarction (homonymous hemianopsia or cortical blindness if bilateral). - Plum and Posner, p. 201
This is a shared conversation. Sign in to Orris to start your own chat.