
Screenshot_20260620-061057.png
Explain trphoblastic tumor with gross and morphology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have all the content needed for a comprehensive answer. Let me compile it.
Gestational Trophoblastic Disease (GTD) - Complete Overview
GTD encompasses a spectrum of tumors and tumor-like conditions characterized by proliferation of placental (trophoblastic) tissue, both villous and non-villous. All types elaborate human chorionic gonadotropin (hCG) to varying degrees, which serves as both a diagnostic and follow-up marker.
Major disorders:
- Hydatidiform Mole (Complete and Partial)
- Invasive Mole
- Choriocarcinoma
- Placental Site Trophoblastic Tumor (PSTT)
- Epithelioid Trophoblastic Tumor (ETT)
1. Hydatidiform Mole
Genetics & Pathogenesis
The key abnormality in all moles is an excess of paternal genetic material:
| Feature | Complete Mole | Partial Mole |
|---|---|---|
| Karyotype | Diploid (46,XX or 46,XY) | Triploid (69,XXY or 69,XXX) |
| Villous edema | ALL villi | SOME villi |
| Trophoblast proliferation | Diffuse; circumferential | Focal; slight |
| Serum hCG | Markedly elevated (>100,000 IU/L) | Less elevated |
| Fetal parts | Absent | May be present |
| Risk of choriocarcinoma | 2.5% | Rare |
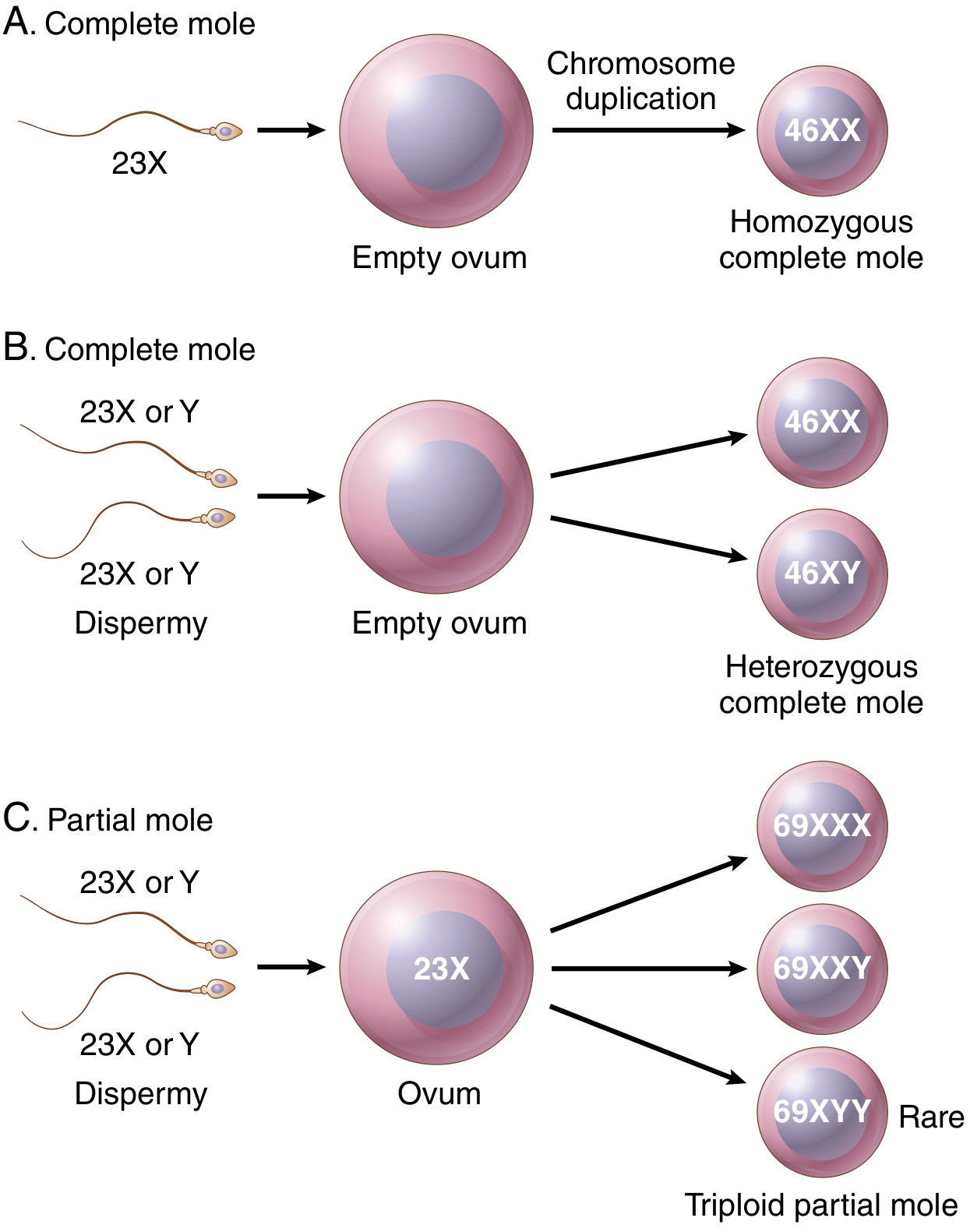
- Complete mole: fertilization of an "empty" egg by one sperm that duplicates (androgenesis, monospermic, 46,XX) or by two sperm (dispermic, 46,XX or 46,XY). No embryonic development occurs.
- Partial mole: normal egg fertilized by two sperm; triploid (69,XXY). Fetal development may occur but fetus is growth-restricted with lethal anomalies.
- Incidence: ~1 in 1,000-2,000 pregnancies in the USA; twice as common in Southeast Asia.
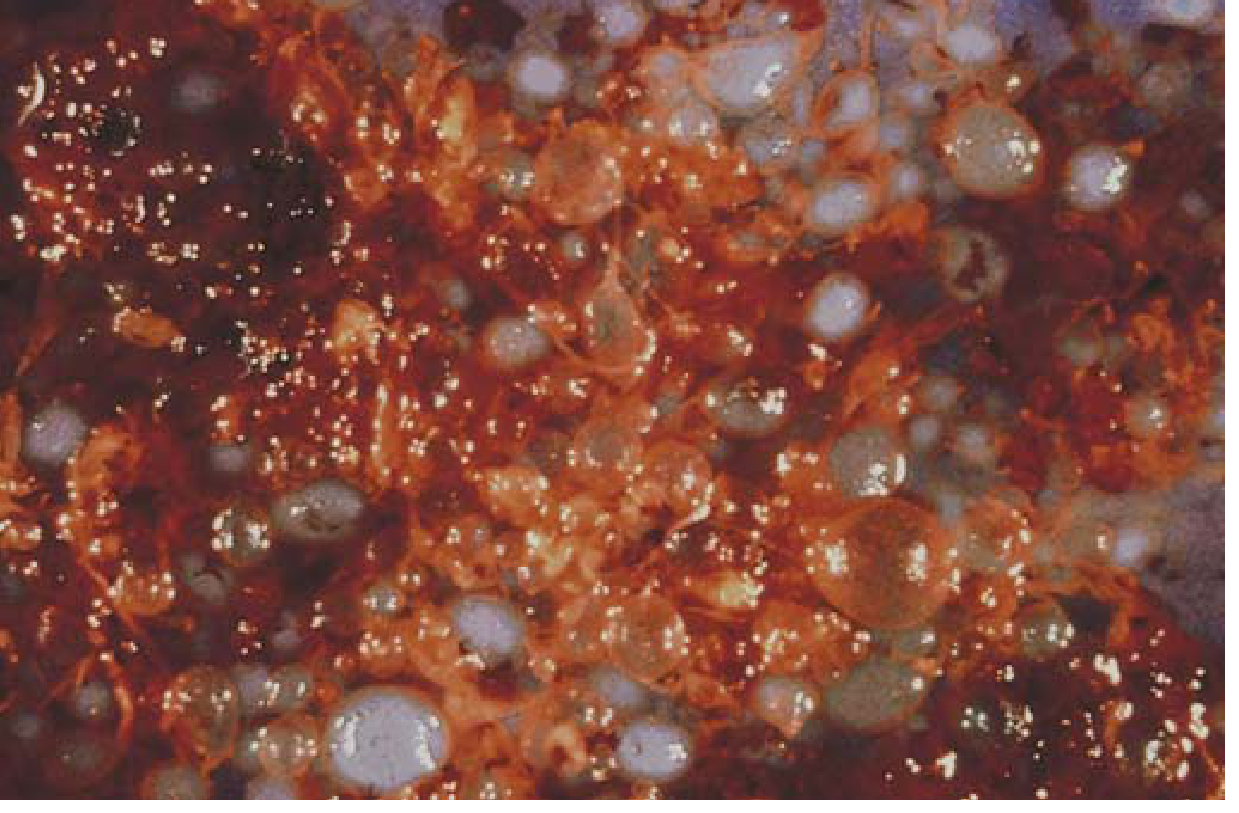
Gross Morphology
The uterine cavity is expanded by a delicate, friable mass of thin-walled, translucent, cystic, grape-like structures - swollen edematous (hydropic) villi. Fetal parts are absent in complete moles but may be present in partial moles.
Microscopic Morphology
- Complete mole: ALL or most villi are abnormal - enlarged, smooth, oval, with central cavitation (cisterns) and myxomatous edematous stroma. Covered by diffuse circumferential trophoblastic hyperplasia involving both cytotrophoblasts AND syncytiotrophoblasts. No fetal vasculature.
- Partial mole: Only a fraction of villi is enlarged and edematous; trophoblastic hyperplasia is focal and limited to syncytiotrophoblasts; villi have irregular/scalloped outlines with prominent trophoblastic inclusions.
2. Invasive Mole
Key Features
- A complete mole that becomes locally aggressive
- Hydropic villi penetrate deeply into or perforate the myometrium, causing life-threatening hemorrhage
- Retains hydropic villi (unlike choriocarcinoma)
- Villi may embolize to lungs or brain, but these emboli do not grow and regress spontaneously
- Lung metastases occur in ~5% of complete moles
Morphology
- Microscopically: hydropic villi + proliferation of both cytotrophoblasts and syncytiotrophoblasts invading myometrium
- Distinguished from choriocarcinoma by the presence of chorionic villi
3. Choriocarcinoma
Pathogenesis
- Malignant neoplasm of trophoblastic cells arising from a previously normal or abnormal pregnancy
- Incidence: 1 in 20,000 to 30,000 pregnancies in the USA
- 50% arise after a complete hydatidiform mole
- 25% follow spontaneous abortions
- ~22% follow normal pregnancies
- Remainder after ectopic pregnancies
Gross Morphology
- Soft, fleshy, yellow-white tumor with large pale areas of necrosis and extensive hemorrhage
- Destructive, hemorrhagic invasion of the myometrium
- May appear as a grossly identifiable mass or present with widespread metastasis
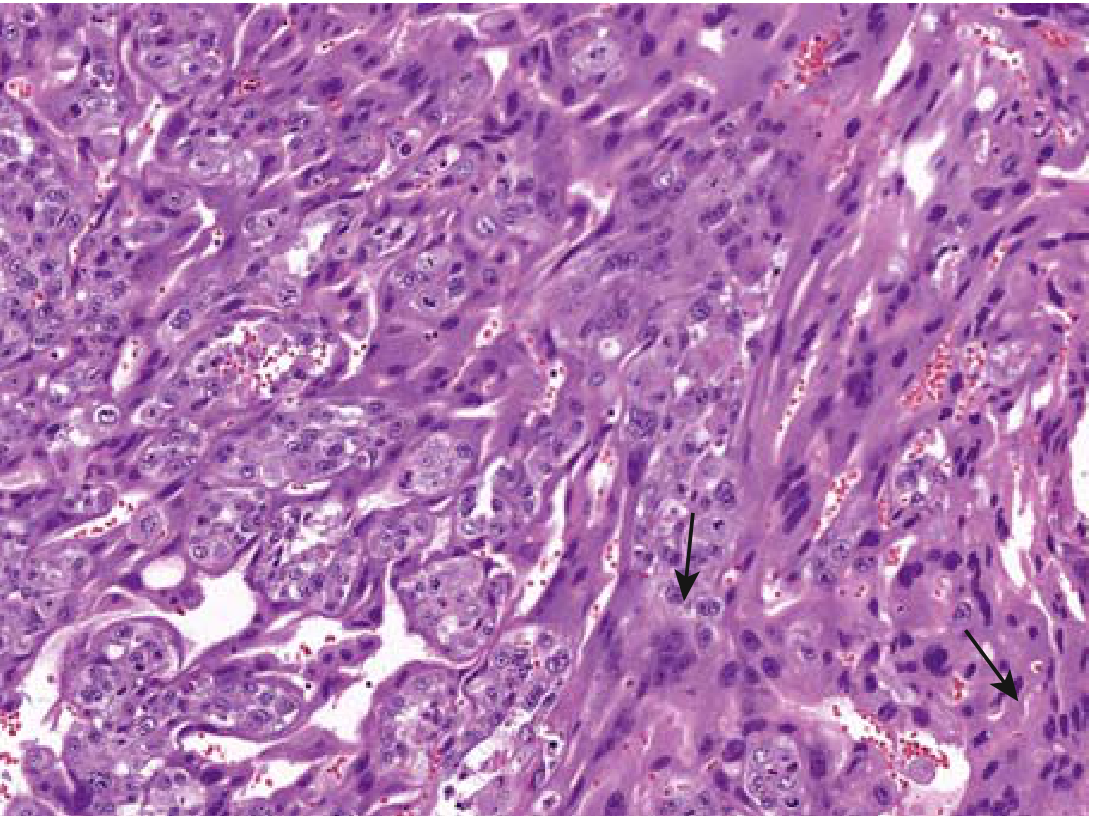
Microscopic Morphology
- Composed of proliferating syncytiotrophoblasts and cytotrophoblasts (both components must be present)
- Chorionic villi are ABSENT - this is the critical distinguishing feature from moles
- Mitoses are abundant and sometimes abnormal
- Tumor invades the underlying myometrium, frequently penetrates blood vessels
- May extend to uterine serosa and adjacent structures
Clinical Features & Spread
- Hematogenous spread is characteristic: lungs (50%) > vagina (30-40%) > brain > liver > bone > kidney
- Lymphatic invasion is uncommon
- Despite being extremely aggressive, gestational choriocarcinoma is remarkably sensitive to chemotherapy - nearly 100% cure rate even with metastases
- Non-gestational choriocarcinomas (from gonads/ovary/testis) have a relatively poor response to chemotherapy
4. Placental Site Trophoblastic Tumor (PSTT)
Pathogenesis
- Neoplastic proliferation of extravillous (intermediate) trophoblasts - cells that migrate from the cytotrophoblast of the placenta and invade the maternal decidua and myometrium
- Intermediate trophoblasts have features overlapping cytotrophoblasts AND syncytiotrophoblasts
- They produce human placental lactogen (hPL) rather than large amounts of hCG - so serum hCG levels are LOW
- Diploid tumors (often 46,XX karyotype), arise months after pregnancy
- Comprise less than 2% of gestational trophoblastic neoplasms
Gross Morphology
- Well-circumscribed, firm nodule in the myometrium or endometrium
- Cut surface is tan-white
Microscopic Morphology
- Sheets and cords of mononuclear intermediate trophoblasts infiltrating between individual smooth muscle fibers of the myometrium
- Cells are large with abundant clear to eosinophilic cytoplasm
- Nuclear atypia and mitotic figures present
- No chorionic villi
- Fibrinoid material often deposited around individual cells
- Immunohistochemistry: HPL positive, hCG focally positive, cytokeratin positive
Clinical Course
- Generally indolent course with favorable outcome if confined to endometrium/myometrium
- NOT as sensitive to chemotherapy as other trophoblastic tumors
- Prognosis is poor once it spreads to extrauterine sites
- Treatment: hysterectomy is typically required
5. Epithelioid Trophoblastic Tumor (ETT)
- Rare variant arising from chorionic-type (implantation site) intermediate trophoblasts
- Presents as a nodule in the endometrium, lower uterine segment, or endocervix
- Microscopically: uniform, mononuclear epithelioid cells in nests surrounded by necrosis (giving a "geographic" necrosis pattern); cells are smaller than PSTT cells
- Low hCG; hPL negative; p63 positive (helpful for distinction from PSTT)
- Treatment: hysterectomy; less responsive to chemotherapy than choriocarcinoma
Summary Table
| Feature | Complete Mole | Partial Mole | Invasive Mole | Choriocarcinoma | PSTT |
|---|---|---|---|---|---|
| Villi | All hydropic | Some hydropic | Hydropic, invade wall | Absent | Absent |
| Trophoblast | Diffuse hyperplasia | Focal hyperplasia | Both types | Both types | Intermediate type |
| hCG | Very high | Elevated/normal | Elevated | Very high | Low |
| hPL | - | - | - | - | Positive |
| Malignancy | No | No | Locally invasive | Yes, metastatic | Low-grade |
| Chemo response | - | - | Good | Excellent | Poor |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528), pp. 956-958
- Robbins & Kumar Basic Pathology (9780323790185), pp. 702-706
This is a shared conversation. Sign in to Orris to start your own chat.