Explain heart failure to a 4 th year mbbs student include high yeild topics and take reference from standard medicine textbooks
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have all the content needed. Let me compile a comprehensive, high-yield explanation of heart failure for a 4th year MBBS student.
Heart Failure - Comprehensive High-Yield Review
References: Braunwald's Heart Disease (10e), Robbins & Cotran Pathologic Basis of Disease (10e), Goldman-Cecil Medicine, Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung's Basic & Clinical Pharmacology
1. Definition
Heart failure (HF) is a clinical syndrome in which the heart is unable to pump blood at a rate sufficient to meet the metabolic demands of the tissues, OR can only do so at the cost of elevated filling pressures. It is not a single disease but a final common pathway of multiple cardiac insults.
- HFrEF (Heart Failure with Reduced EF, formerly "systolic HF"): EF < 40%
- HFpEF (Heart Failure with Preserved EF, formerly "diastolic HF"): EF ≥ 50%
- HFmrEF (Mid-range EF): EF 40-49%
2. Epidemiology & Etiology
Most common causes globally:
- Ischemic Heart Disease (IHD) - most common cause in developed countries
- Hypertension
- Valvular heart disease (aortic stenosis/regurgitation, mitral regurgitation)
- Dilated cardiomyopathy
- Diabetes mellitus
Less common but exam favorites:
- Alcohol/toxin-induced cardiomyopathy
- Viral myocarditis
- Thyroid disease (both hypo and hyper)
- Haemochromatosis, amyloidosis
- Peripartum cardiomyopathy
- Chagas disease (endemic regions)
3. Pathophysiology
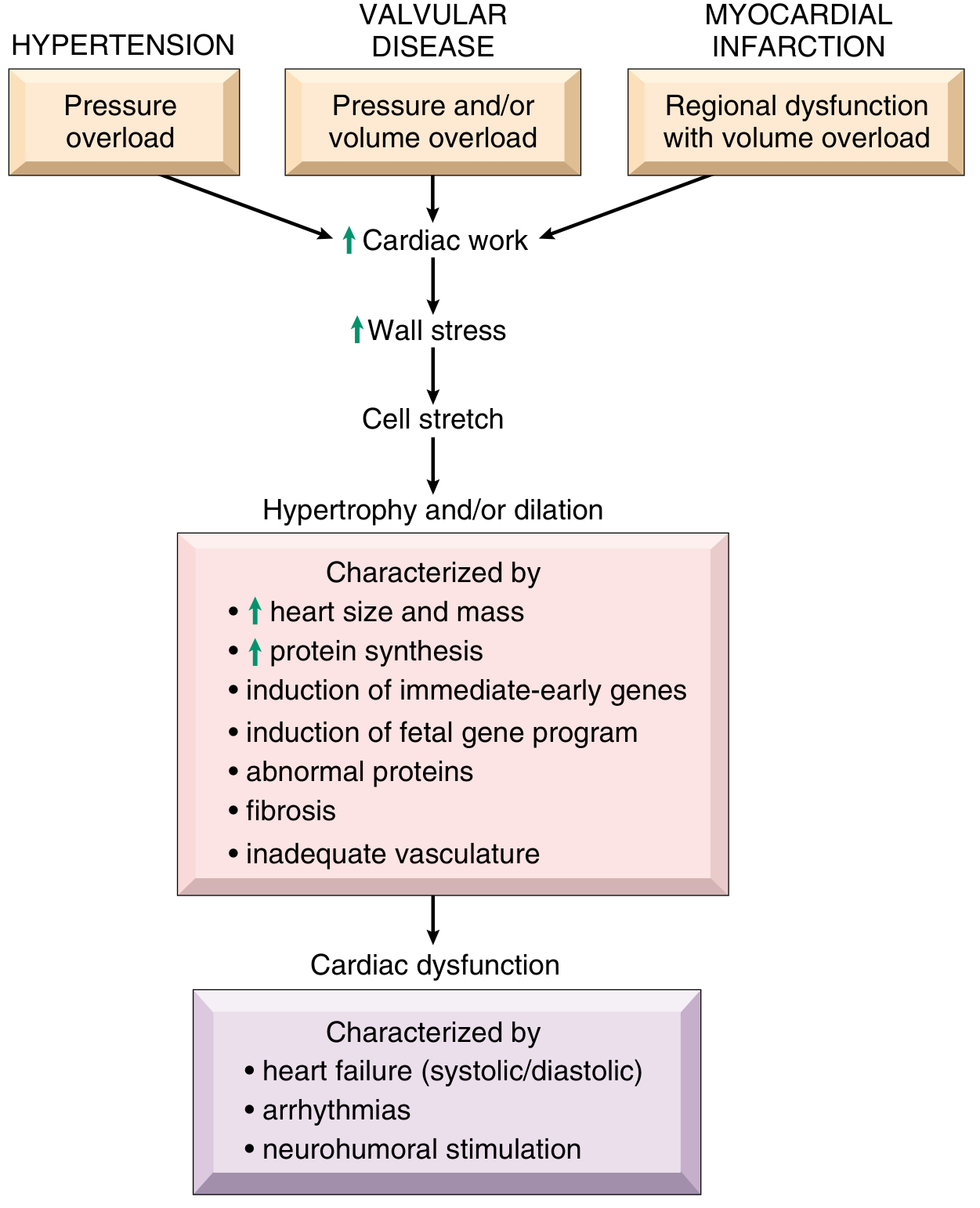
3a. The Central Concept: Cardiac Overload and Hypertrophy
As Robbins explains, a sustained increase in mechanical work from pressure overload, volume overload, or trophic signals (e.g., β-adrenergic activation) forces myocytes to hypertrophy. Hypertrophic myocytes show enlarged/multiple nuclei (increased DNA ploidy without cell division) and require increased protein synthesis for additional sarcomeres.
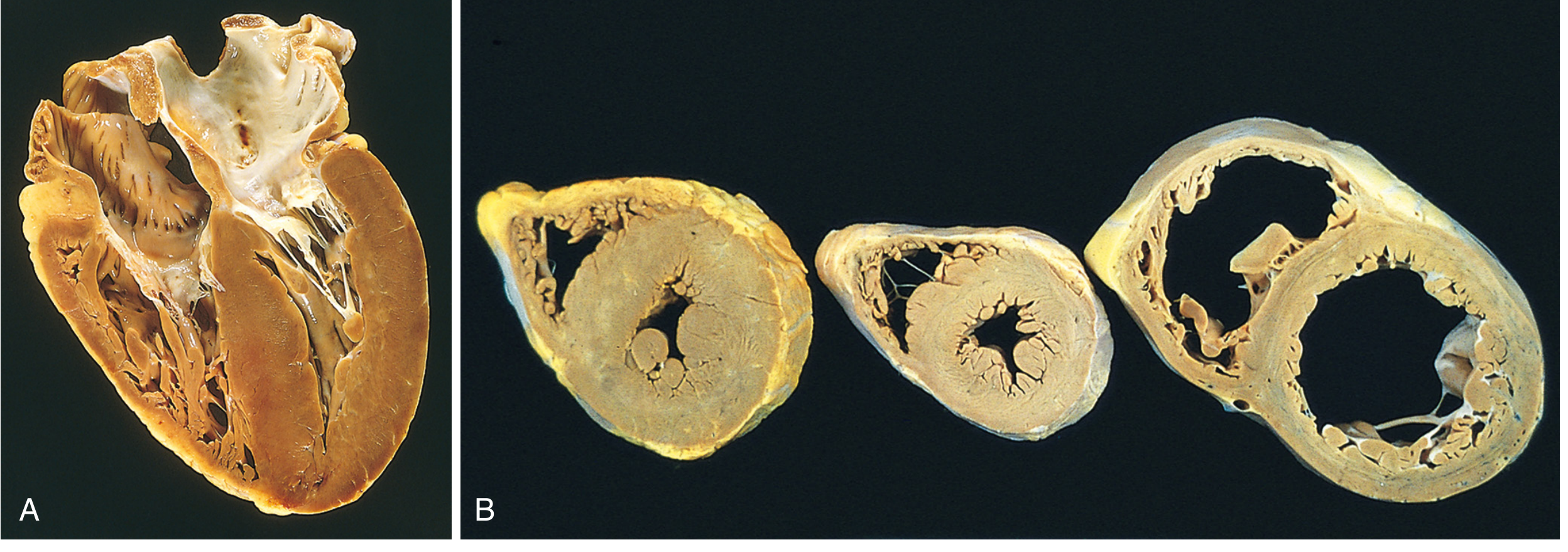
Pattern of hypertrophy:
| Type | Cause | Pattern | Result |
|---|---|---|---|
| Pressure overload | Hypertension, Aortic stenosis | New sarcomeres in parallel | Concentric hypertrophy - thick walls, reduced cavity |
| Volume overload | Mitral/Aortic regurgitation | New sarcomeres in series | Eccentric hypertrophy - dilated thin-walled heart |
Why does hypertrophy fail?
Myocyte hypertrophy is not accompanied by proportional increase in capillary density - the ischemic supply-demand mismatch worsens over time. Additional problems include:
- Interstitial fibrosis
- Induction of fetal gene program (re-expression of embryonic myosin isoforms - less efficient)
- Mitochondrial dysfunction
- Calcium handling abnormalities (impaired SERCA2a activity)
3b. The Four Interrelated Systems (Goodman & Gilman)
The pathophysiology of HF involves:
- The heart itself - loss of muscle mass, overload, genetic cardiomyopathy
- The vasculature - increased afterload, impaired peripheral vasodilation
- The kidney - sodium and water retention, cardiorenal syndrome
- Neurohumoral regulatory circuits - the most clinically important axis
3c. Neurohumoral Activation (HIGH YIELD)
This is the cornerstone of modern HF pathophysiology and treatment rationale:
Initial fall in cardiac output triggers:
-
Sympathetic nervous system activation
- Increases heart rate and contractility (initially compensatory)
- Causes vasoconstriction (maintains BP)
- Chronically: downregulates β1-receptors, causes myocyte apoptosis, promotes arrhythmias
-
RAAS activation (Renin-Angiotensin-Aldosterone System)
- Low renal perfusion → Renin release → Angiotensin I → ACE → Angiotensin II
- Angiotensin II: vasoconstriction, aldosterone secretion, myocardial fibrosis, sympathetic amplification
- Aldosterone: Na+ and water retention, K+ wasting, contributes to myocardial fibrosis
-
ADH/Vasopressin (AVP) release
- Free water retention → hyponatremia in advanced HF
- Vasoconstriction via V1 receptors
-
Endothelin-1 - potent vasoconstrictor, promotes fibrosis
Counter-regulatory (beneficial) system:
- Natriuretic Peptides (ANP, BNP, CNP): released in response to wall stretch
- Cause natriuresis, vasodilation, and oppose RAAS
- BNP levels are used diagnostically (see biomarkers section)
- Nitric Oxide (NO): vasodilatory, impaired in chronic HF
The Vicious Cycle: Reduced CO → Neurohumoral activation → ↑Afterload & ↑Preload → Further wall stress → Further myocardial damage → Further reduced CO
4. Classification (HIGH YIELD - Must Know)
ACC/AHA Staging (emphasizes disease progression):
| Stage | Description | NYHA Equivalent |
|---|---|---|
| A | High risk for HF; no structural disease or symptoms | None |
| B | Structural disease; no symptoms | Class I |
| C | Structural disease; prior or current symptoms | Class I-III |
| D | Refractory HF requiring specialized interventions | Class IV |
NYHA Functional Classification (for therapy eligibility and prognosis):
| Class | Description |
|---|---|
| I | No limitation. Ordinary activity does NOT cause symptoms |
| II | Slight limitation. Comfortable at rest; ordinary activity causes symptoms |
| III | Marked limitation. Comfortable at rest; less-than-ordinary activity causes symptoms |
| IV | Unable to carry out any physical activity without symptoms; OR symptoms at rest |
Key exam point: NYHA class determines eligibility for MRAs (Class II-IV), CRT (Class III-IV), LVAD/transplant (Class IV). The ACC/AHA staging does not go backward - once Stage C, always Stage C.
5. Clinical Features
Left-Sided Heart Failure (Pulmonary Congestion + Low Output)
Symptoms (from Braunwald's Table 48.2):
- Dyspnea - cardinal symptom; initially on exertion, then at rest
- Orthopnea - dyspnea when supine; relieved by sitting up (report by number of pillows)
- Paroxysmal Nocturnal Dyspnea (PND) - sudden dyspnea at night; highly specific for LHF
- Fatigue, reduced exercise tolerance
- Cough (sometimes pink/frothy sputum in severe pulmonary edema)
- Cheyne-Stokes respiration (in advanced HF, often with co-existing sleep apnoea)
- Nocturia (recumbency increases renal perfusion at night)
Signs:
- Tachycardia
- Displaced apex beat (cardiomegaly)
- S3 gallop (ventricular filling sound; highly specific for volume overload/HFrEF; heard best at apex with bell in left lateral decubitus)
- S4 gallop (atrial kick against a stiff ventricle; more common in HFpEF)
- Fine crepitations/crackles at lung bases (pulmonary edema)
- Reduced air entry + dullness (pleural effusion - typically right-sided or bilateral)
- Pulsus alternans (in severe LHF)
- Raised JVP (when LHF has caused RHF)
Morphological changes (Robbins):
- Heart failure cells (hemosiderin-laden macrophages) in alveolar spaces - pathognomonic of previous pulmonary edema
- Heavy, wet lungs
- Perivascular and interstitial edema; alveolar edema
- Left atrial dilation → risk of atrial fibrillation and thrombus (especially in atrial appendage)
Right-Sided Heart Failure (Systemic Venous Congestion)
Most common cause: Left-sided HF (transmitted pulmonary hypertension). Isolated RHF = Cor Pulmonale (from lung disease).
Symptoms:
- Peripheral oedema (pitting; worse at end of day)
- Abdominal distension, ascites
- Right upper quadrant pain/discomfort (liver congestion)
- Loss of appetite, early satiety (gut oedema/bowel wall oedema)
- Anasarca in severe cases
Signs:
- Raised JVP - most reliable sign of RHF; hepatojugular reflux positive
- Pitting pedal/ankle oedema
- Hepatomegaly (tender, pulsatile in tricuspid regurgitation)
- Ascites
- Nutmeg liver on histology - centrilobular congestion (pericentral red-brown zones, periportal tan areas)
- Congestive splenomegaly
- Right ventricular heave (parasternal lift)
- Cardiac cirrhosis in chronic severe RHF
6. HFpEF vs HFrEF - High-Yield Comparison
| Feature | HFrEF (Systolic) | HFpEF (Diastolic) |
|---|---|---|
| EF | < 40% | ≥ 50% |
| Mechanism | Impaired contractility | Impaired relaxation/compliance |
| LV Size | Usually dilated | Normal or slightly enlarged |
| Wall thickness | Decreased (eccentric) | Increased (concentric) |
| Common causes | IHD, DCM, viral myocarditis | Hypertension, DM, obesity, ageing |
| Treatment evidence | Strong (ACEI/ARB/ARNI + BB + MRA + SGLT2i) | Weaker; mostly symptom-based |
7. Investigations
Biomarkers (HIGH YIELD)
- BNP and NT-proBNP: Released from ventricular myocytes in response to wall stretch; supported by ACC/AHA Class I recommendation for diagnosis of acute HF and prognosis in chronic HF
- BNP >100 pg/mL supports diagnosis; NT-proBNP >300 pg/mL (acute) or >125 pg/mL (chronic)
- Both can be elevated by: CKD, AF, PE, sepsis, obesity (falsely low in obesity)
- Useful to guide therapy titration in outpatient setting
ECG
- Usually not normal in HF but non-specific
- LVH pattern, LBBB (associated with dyssynchrony - indicates CRT benefit)
- AF (very common comorbidity)
- Old MI changes (Q waves indicating ischemic etiology)
- Prolonged QRS > 120 ms with LBBB → CRT candidate
Chest X-Ray (CXR)
Classic radiological signs of LHF (remember ABC of pulmonary oedema):
- A - Alveolar oedema ("bat-wing" hilar haziness)
- B - Kerley B lines (horizontal lines in costophrenic angles - interstitial oedema in interlobular septa)
- C - Cardiomegaly (CTR > 0.5 on PA film)
- Upper lobe venous diversion (earliest sign)
- Pleural effusion (blunting of costophrenic angles)
Echocardiography (Most Important Investigation)
- Confirms diagnosis, measures EF, identifies etiology
- Assesses wall motion abnormalities, valvular disease, pericardial disease
- E/A ratio, E/e' ratio for diastolic dysfunction
- Pulmonary artery pressure estimation (TR jet)
Other Investigations
- FBC - anaemia (common, worsens HF)
- Renal function/electrolytes - essential before starting RAAS blockers; CRS
- TFTs - hypo/hyperthyroidism as cause
- LFTs - hepatic congestion (raised bilirubin, ALP, GGT)
- Blood glucose/HbA1c - DM major risk factor/comorbidity
- Iron studies - iron deficiency common, treatable
- Cardiac MRI - gold standard for myocardial characterisation, viability
8. Management (HIGH YIELD)
The "Fantastic Four" - Disease-Modifying Therapy for HFrEF
Current guidelines (2021 ESC, 2022 ACC/AHA) support four drug classes with proven mortality benefit in HFrEF:
| Drug Class | Example | Key Mechanism | Survival Benefit Trial |
|---|---|---|---|
| ARNI (preferred) or ACEi or ARB | Sacubitril/Valsartan; Enalapril; Candesartan | Block RAAS; ARNI also inhibits neprilysin (↑natriuretic peptides) | PARADIGM-HF (ARNI), SOLVD (ACEi) |
| Beta-blocker | Carvedilol, Bisoprolol, Metoprolol succinate | Block chronic sympathetic activation, reverse remodelling | MERIT-HF, COPERNICUS |
| MRA (Mineralocorticoid Receptor Antagonist) | Spironolactone, Eplerenone | Block aldosterone; reduce fibrosis, K+ retention | RALES (spiro), EMPHASIS-HF (eplerenone) |
| SGLT2 inhibitor | Dapagliflozin, Empagliflozin | Glycosuria + osmotic diuresis; reduce hospitalization and CV death | DAPA-HF, EMPEROR-Reduced |
All four should be initiated and up-titrated to maximum tolerated doses. Diuretics provide symptom relief but do NOT improve survival.
Diuretics (Symptomatic Relief)
- Loop diuretics (Furosemide): First-line for decongestion; rapid onset
- Thiazides (Hydrochlorothiazide): Used in combination with loop diuretics in resistant oedema ("sequential nephron blockade")
- Metolazone: Potent; used with furosemide in refractory oedema - monitor electrolytes closely
- Monitor: Hypokalemia, hyponatremia, prerenal azotemia
Contraindicated/Caution in HF
- NSAIDs - cause sodium retention, worsen renal function, block diuretic effect
- Non-DHP Calcium channel blockers (Diltiazem, Verapamil) - negative inotrope; contraindicated in HFrEF
- Class I antiarrhythmics - proarrhythmic
- Thiazolidinediones (Pioglitazone) - cause fluid retention
Device Therapy (HIGH YIELD)
| Device | Indication |
|---|---|
| ICD (Implantable Cardioverter Defibrillator) | EF ≤ 35%, NYHA II-III, on OMT for ≥3 months; primary prevention of sudden cardiac death |
| CRT (Cardiac Resynchronisation Therapy) | EF ≤ 35%, QRS ≥ 150 ms with LBBB, NYHA II-IV; improves dyssynchrony |
| CRT-D | ICD + CRT combined |
| LVAD (Left Ventricular Assist Device) | Stage D refractory HF; bridge to transplant or destination therapy |
| Heart Transplant | Stage D, no contraindications; 1-year survival >85% |
Acute Decompensated Heart Failure (ADHF)
- LMNOP mnemonic: Lasix (furosemide IV), Morphine (with caution), Nitrates, O2, Positioning (sit upright)
- IV loop diuretics - cornerstone of acute management
- Non-invasive ventilation (CPAP/BiPAP) for respiratory failure
- Inotropes (Dobutamine, Milrinone) for cardiogenic shock
- Nitroprusside for hypertensive emergency with acute HF
9. Prognosis and Prognostic Markers
- 5-year mortality ~50% - worse than most cancers
- Poor prognostic markers:
- Very low EF (< 20%)
- NYHA Class IV
- Very high BNP/NT-proBNP
- Hyponatremia (reflects severe neurohumoral activation)
- Renal dysfunction (cardiorenal syndrome)
- Wide QRS / LBBB
- Cardiac cachexia (weight loss > 6% in 6 months)
10. High-Yield Exam Points Summary
- "Heart failure cells" = hemosiderin-laden macrophages in alveoli (from Robbins) - hallmark of old pulmonary oedema
- "Nutmeg liver" = centrilobular congestion in right-sided HF (pericentral red-brown, periportal tan)
- S3 gallop = most specific sign of systolic HF/volume overload (Ken-TUC-KY rhythm)
- Orthopnea and PND are most specific symptoms for left HF
- JVP raised + pedal oedema = systemic venous congestion (right HF)
- First-line FOUR drugs (ARNI/ACEi + BB + MRA + SGLT2i) ALL have mortality benefit in HFrEF
- ICD for EF ≤ 35% (primary SCD prevention); CRT for EF ≤ 35% + QRS ≥ 150 ms LBBB
- BNP rules out HF if very low; elevated in HF, PE, AF, CKD
- NYHA Class III-IV = spiro benefit (RALES); Class II = eplerenone benefit (EMPHASIS-HF)
- Pressure overload = concentric hypertrophy; Volume overload = eccentric/dilated (Robbins)
- HFpEF = normal or near-normal EF, stiff ventricle, mostly elderly women with hypertension and DM
- ACC/AHA Stage A = risk factors only, no structural disease - intervene to prevent progression
- SGLT2 inhibitors now have Class I indication in HFrEF even in non-diabetics
- Cor pulmonale = right HF from LUNG disease (not from left HF)
- Kerley B lines on CXR = interstitial pulmonary oedema (fluid in interlobular septa)
Sources: Braunwald's Heart Disease 10e (Chapters 48, 13); Robbins & Cotran Pathologic Basis of Disease 10e (Chapter 12); Goldman-Cecil Medicine (Chapter 46); Goodman & Gilman's Pharmacological Basis of Therapeutics (Chapter 33); Katzung's Basic & Clinical Pharmacology 16e (Chapter 13)
This is a shared conversation. Sign in to Orris to start your own chat.