Ne0hrotic syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have sufficient information to write a comprehensive answer. Let me compile it.
Nephrotic Syndrome
A complete clinical overview drawn from Comprehensive Clinical Nephrology, 7th Edition, Brenner and Rector's The Kidney, Campbell-Walsh-Wein Urology, and Frameworks for Internal Medicine.
Definition
Nephrotic syndrome is a clinical syndrome pathognomonic of glomerular disease, defined by the classic pentad:
| Feature | Threshold |
|---|---|
| Proteinuria | > 3.5 g/24 h in adults; > 40 mg/m²/h or urine protein:creatinine > 2.0 in children |
| Hypoalbuminemia | Serum albumin < 3.0 g/dL (often < 2.5 g/dL) |
| Edema | Periorbital, peripheral, ascites, pleural effusion |
| Hyperlipidemia | Elevated LDL, VLDL, total cholesterol; variable triglycerides |
| Lipiduria | Oval fat bodies, fatty casts in urine (maltese cross pattern) |
Not all patients with proteinuria > 3.5 g/24 h will have the full syndrome - some maintain normal albumin through compensatory hepatic synthesis.
- Comprehensive Clinical Nephrology, 7th Ed., p. 240
Classification
Nephrotic syndrome is divided into primary (idiopathic) and secondary causes:
Primary Causes (by histology)
| Lesion | Key Points |
|---|---|
| Minimal Change Disease (MCD) | Most common in children; podocyte effacement on EM; steroid-responsive (>80% remission); relapses common |
| Focal Segmental Glomerulosclerosis (FSGS) | Most common in Black patients (~50% of their glomerular disease); associated with highest risk of thromboembolism; steroid-resistant patterns common |
| Membranous Nephropathy (MN) | Most common primary cause in white adults; associated with anti-PLA2R antibodies; ~30% spontaneous remission |
| Membranoproliferative GN (MPGN) | Can present with nephrotic syndrome in a subset; low complement |
| IgA Nephropathy | Mainly nephritic but nephrotic presentation possible |
| Mesangial Proliferation | Less common; overlaps with other patterns |
Secondary Causes
| Category | Examples |
|---|---|
| Autoimmune | SLE (membranous pattern), rheumatoid arthritis |
| Infections | Hepatitis B (membranous), Hepatitis C (MPGN), HIV (collapsing FSGS), malaria (quartan) |
| Medications | NSAIDs, penicillamine, gold, captopril, heroin |
| Malignancy | Colon cancer (membranous), lymphoma (MCD), myeloma (amyloid) |
| Metabolic | Diabetes mellitus (diabetic nephropathy), amyloidosis |
| Congenital | Finnish-type (NPHS1/nephrin), podocin mutations (NPHS2) |
FSGS is the most common cause in Black patients; membranous nephropathy is the most common in white adults.
- Frameworks for Internal Medicine, p. 465
Pathophysiology
1. Edema - Two mechanisms
Underfill (especially in MCD):
- Urinary albumin loss → hypoalbuminemia → decreased plasma oncotic pressure → fluid shifts into interstitium → reduced effective circulating volume → RAAS activation → aldosterone-driven sodium retention
Overfill (most common - occurs in most nephrotic patients):
- Primary defect in distal nephron sodium excretion, possibly from proteolytic activation of the epithelial sodium channel (ENaC) by proteinuric enzymes entering the tubular lumen → sodium retention → expanded blood volume → transudation despite low oncotic pressure
- Kidney is also relatively resistant to atrial natriuretic peptide (ANP) in this state
MCD patients tend toward underfill with contracted plasma volume; other causes tend toward overfill with expanded plasma volume and suppressed RAAS.
2. Hypoalbuminemia
- Massive urinary albumin loss exceeds hepatic compensatory synthesis
- Up to 10-20% of lean body mass can be lost (masked by edema)
- Hepatic protein synthesis increases non-discriminately - large molecules (fibrinogen, lipoproteins) rise, while small molecules are lost in urine
3. Hypercoagulability
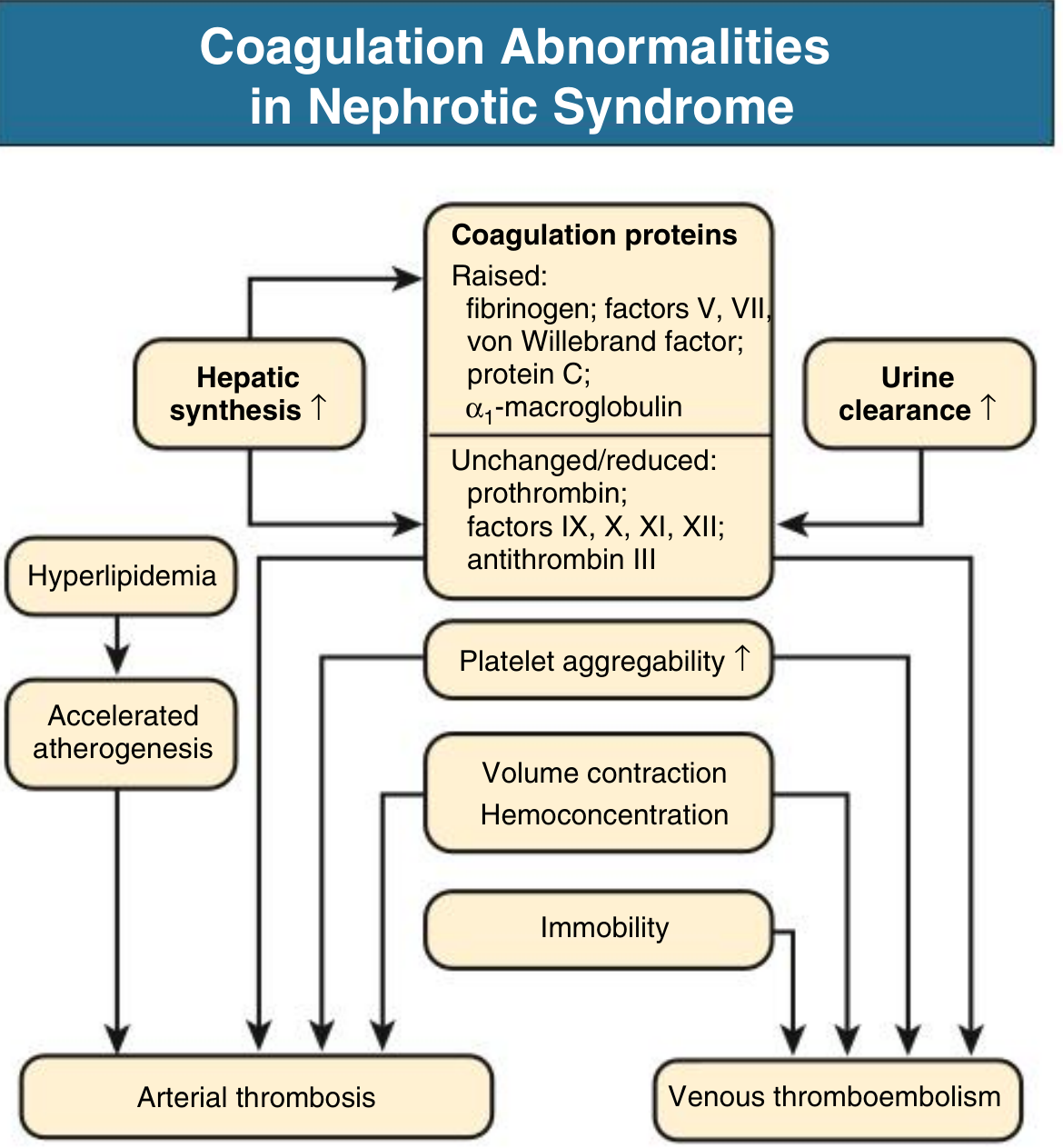
- Raised: Fibrinogen, factors V, VII, von Willebrand factor, protein C, alpha-1-macroglobulin
- Reduced (urinary loss): Antithrombin III, proteins C and S (paradox: despite protein C being raised in synthesis, functional anticoagulants net decrease)
- Platelet aggregability increases
- Compounded by immobility, hemoconcentration, dehydration
- Most common sites: renal veins (10-50% on systematic imaging), lower extremity veins, pulmonary emboli
- Arterial thrombosis (coronary, cerebrovascular) can occur in adults
4. Hyperlipidemia
- Hypoalbuminemia stimulates hepatic synthesis of LDL, VLDL, and lipoprotein(a)
- Defective peripheral lipoprotein lipase reduces VLDL clearance
- Urinary loss of HDL
- PCSK9 overexpression in kidney and liver (emerging therapeutic target)
- Nephrotic patients have ~5-fold increased risk for coronary death, except MCD (transient nephrotic state)
- Cholesterol may exceed 500 mg/dL; xanthelasmas can develop rapidly
5. Susceptibility to Infection
- Loss of IgG in urine → hypogammaglobulinemia
- Reduced complement activity
- Diminished T-cell function
- Common: cellulitis, spontaneous bacterial peritonitis (encapsulated organisms: Streptococcus pneumoniae, E. coli)
6. Other Metabolic Effects
- Hypothyroidism: loss of thyroid-binding globulin and T3/T4 in urine
- Hypocalcemia: loss of vitamin D-binding protein → 25-OH vitamin D deficiency → secondary hyperparathyroidism
- Drug binding alterations: Hypoalbuminemia reduces furosemide protein binding, enlarging volume of distribution; albumin-premixed furosemide administration is not confirmed to enhance diuresis
- Negative nitrogen balance: wasting illness
Diagnosis
Workup
- Urine: Dipstick (proteinuria 3+ to 4+), urine protein:creatinine ratio, urine microscopy (oval fat bodies, fatty casts, Maltese cross under polarized light)
- Blood: Serum albumin, LFTs, lipid panel, renal function (BMP), complement levels (C3, C4), ANA, anti-dsDNA, ANCA, anti-PLA2R, hepatitis B/C serology, HIV, serum protein electrophoresis
- 24-hour urine or spot urine protein:creatinine for quantification
- Renal biopsy: Indicated in adults (necessary to determine etiology); in children with typical presentation, empiric steroid therapy is started first - biopsy reserved for atypical features (age <1 year, macroscopic hematuria, hypertension, hypocomplementemia, steroid resistance)
Management
General / Supportive Measures
| Issue | Intervention |
|---|---|
| Edema | Dietary sodium restriction; loop diuretics (furosemide); add thiazide for synergy; avoid vigorous diuresis in underfill (MCD) |
| Proteinuria reduction | ACE inhibitors or ARBs (also combat coagulopathy, dyslipidemia, and slow CKD progression) |
| Hyperlipidemia | Statins (primarily for cardiovascular prevention; role in slowing CKD progression is inconclusive) |
| Hypercoagulability | Anticoagulation considered for serum albumin < 2.0-2.5 g/dL or documented thrombosis |
| Infection | Pneumococcal vaccination; prophylactic penicillin in children |
| Nutrition | Avoid high-protein diet (worsens proteinuria by increasing GFR); normal or mildly restricted protein |
Disease-Specific Treatment
| Disease | First Line | Steroid-Refractory / Dependent |
|---|---|---|
| MCD (children) | Prednisone 60 mg/m²/day x 4-6 weeks, then alternate-day taper | Cyclophosphamide, CNIs (tacrolimus/cyclosporine), MMF, rituximab |
| MCD (adults) | Systemic glucocorticoids; >80% remission but frequent relapses | Tacrolimus, cyclophosphamide, rituximab |
| FSGS | Corticosteroids (prolonged); ~25-30% complete response | CNIs (cyclosporine, tacrolimus), mycophenolate, rituximab; sparsentan (novel dual endothelin/AT1 antagonist) |
| Membranous nephropathy | Wait-and-watch (30% spontaneous remission); KDIGO recommends cyclophosphamide + steroids or CNIs | Rituximab (anti-CD20) targeting anti-PLA2R |
| Secondary | Treat the underlying cause |
Steroid Response Categories (Pediatric)
- Steroid-sensitive NS (SSNS): Remission within 8 weeks
- Frequently-relapsing NS (FRNS): ≥2 relapses within 6 months, or ≥4 relapses in any 12 months
- Steroid-dependent NS (SDNS): Relapses during or immediately after steroid taper
- Steroid-resistant NS (SRNS): No remission after 8 weeks of adequate steroids - requires biopsy, genetic testing (NPHS1, NPHS2, WT1, TRPC6, etc.)
Complications Summary
| Complication | Mechanism | Clinical Consequence |
|---|---|---|
| Thromboembolism | Antithrombin III loss, hypercoagulability | Renal vein thrombosis, PE, DVT |
| Infections | IgG loss, complement loss | Cellulitis, peritonitis, sepsis |
| Cardiovascular disease | Prolonged hyperlipidemia | 5x coronary death risk |
| Acute kidney injury | Volume depletion, renal vein thrombosis, diuretic excess | Transient or permanent decline |
| Protein malnutrition | Urinary protein losses + catabolism | Wasting, poor wound healing |
| Endocrine/mineral | Loss of carrier proteins | Hypothyroidism, hypocalcemia, osteomalacia |
Recent Evidence (2024-2026)
A 2024 Cochrane meta-analysis on corticosteroids in childhood nephrotic syndrome (PMID 39171624) and a 2025 Cochrane review on steroid-resistant NS in children (PMID 40337980) confirm the current standard-of-care approaches. A 2026 systematic review (PMID 41843217) highlights rituximab-induced hypogammaglobulinemia as a significant adverse effect to monitor in pediatric nephrotic syndrome treated with rituximab.
Sources: Comprehensive Clinical Nephrology 7th Ed., pp. 239-244; Brenner and Rector's The Kidney; Campbell-Walsh-Wein Urology; Frameworks for Internal Medicine, pp. 463-465
This is a shared conversation. Sign in to Orris to start your own chat.