Uvea
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compose the full answer.
The Uvea
The term uvea derives from the Latin word for "grape" - a reference to the grape-like appearance of the pigmented vascular coat of the eye when the sclera is removed. It forms the middle (vascular) tunic of the eyeball, sandwiched between the outer fibrous coat (cornea/sclera) and the inner nervous coat (retina).
Components
The uvea has three anatomically continuous parts:
| Structure | Location | Primary Functions |
|---|---|---|
| Iris | Anterior | Pupillary aperture control; light regulation |
| Ciliary body | Middle | Aqueous humor secretion; lens accommodation |
| Choroid | Posterior | Nutrient supply to outer retina |
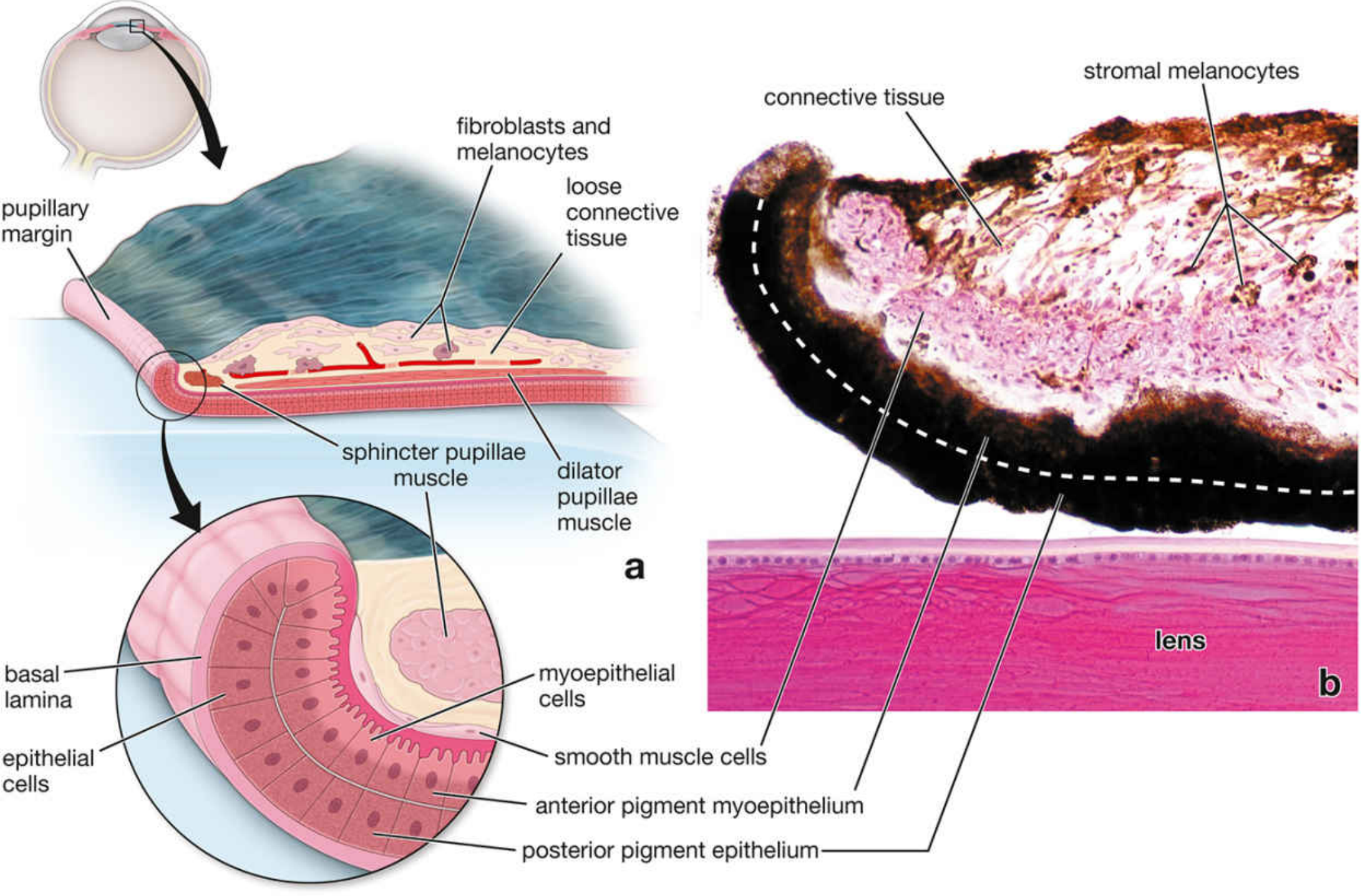
1. The Iris
The iris is the most anterior part of the uvea and forms a contractile diaphragm in front of the lens. The central aperture is the pupil.
Histological layers (anterior → posterior):
- Anterior surface: a discontinuous layer of fibroblasts and stromal melanocytes (no true epithelium)
- Stroma: loose vascularized connective tissue; contains the sphincter pupillae muscle (circumferential smooth muscle near the pupillary margin)
- Anterior pigment myoepithelium: radially-oriented myoepithelial cells whose contractile processes form the dilator pupillae muscle
- Posterior pigment epithelium: densely pigmented cells; so pigmented that nuclei are invisible by light microscopy
Pupillary muscles and innervation:
| Muscle | Type | Innervation | Action |
|---|---|---|---|
| Sphincter pupillae | Circular smooth muscle | Parasympathetic (CN III) | Miosis (constriction) |
| Dilator pupillae | Radial myoepithelial processes | Sympathetic (superior cervical ganglion) | Mydriasis (dilation) |
Eye color is determined by the density of stromal melanocytes. Few melanocytes → blue iris (reflected light from posterior pigment layer). More melanocytes → green, gray, then brown.
Clinical note: Atropine (a muscarinic ACh receptor blocker) paralyzes the sphincter pupillae, producing mydriasis used for ophthalmoscopy. "Fixed and dilated" pupils indicate loss of parasympathetic tone (CN III palsy or brainstem dysfunction).
2. The Ciliary Body
The ciliary body is the thickened anterior portion of the vascular coat, located between the iris root and the choroid (at the ora serrata). It extends about 6 mm and bears approximately 75 ciliary processes anteriorly.
Structure:
- Ciliary muscle (bulk of the body): smooth muscle with three functional groups:
- Meridional (longitudinal) fibers - stretch the choroid; may open the iridocorneal angle to help aqueous drainage
- Radial (oblique) fibers - flatten the lens for distant vision
- Circular (sphincteric) fibers - reduce tension on the zonule, allowing the lens to round up for near vision (accommodation)
- Ciliary processes: finger-like projections that secrete aqueous humor
- Double-layered epithelium: continuation of the retinal pigment epithelium; the non-pigmented inner layer secretes aqueous humor
Aqueous humor:
- Secreted by the ciliary epithelium from blood plasma
- Contains <0.1% protein (vs. 7% in plasma)
- Flows: posterior chamber → between iris and lens → anterior chamber → trabecular meshwork → Canal of Schlemm → scleral veins
- Turnover: approximately every 1.5-2 hours
- Functions: maintains intraocular pressure; nourishes the avascular cornea and lens
Zonule of Zinn (suspensory ligament): fibers arise from grooves between ciliary processes and attach to the lens capsule, transmitting ciliary muscle tension to control lens shape.
3. The Choroid
The choroid is the posterior portion of the uvea, lying between the sclera and the retina. It is among the most richly vascularized tissues in the body - only 0.25 mm thick posteriorly and 0.1 mm anteriorly.
Layers (outer → inner):
- Suprachoroid lamina (lamina fusca): large flat melanocytes, collagen, elastic fibers, fibroblasts, macrophages, lymphocytes; lymphatic channels (epichoroid lymph spaces); long and short posterior ciliary vessels pass through here
- Large and medium vessel layers: mostly veins that drain as vortex veins (pass obliquely through the sclera)
- Choriocapillary layer: single plane of fenestrated capillaries - provides nutrients to the outer retinal layers; denser and thicker at the fovea; ends at the ora serrata
- Bruch membrane (lamina vitrea): 1-4 µm thick; separates the choriocapillary layer from the retinal pigment epithelium; clinically important in age-related macular degeneration
The choroid attaches firmly to the sclera at the optic nerve margin. The potential space between sclera and choroid (perichoroidal space) can accumulate fluid in choroidal detachment.
Pathology of the Uvea
Uveitis
Uveitis is inflammation affecting one or more uveal tissues. Clinically the term is reserved for chronic inflammatory diseases, either systemic or ocular in origin.
Classification by location:
- Anterior uveitis (iritis/iridocyclitis): iris and ciliary body; most common form; associated with HLA-B27 spondyloarthropathies, juvenile idiopathic arthritis
- Intermediate uveitis: vitreous and pars plana
- Posterior uveitis (choroiditis/chorioretinitis): choroid ± retina
- Panuveitis: all components
Causes:
- Infectious: toxoplasmosis (most common cause of posterior uveitis), CMV retinitis (AIDS), Pneumocystis, mycobacteria, herpes viruses
- Granulomatous/idiopathic: sarcoidosis (anterior "mutton-fat" keratic precipitates; posterior "candle wax dripping" retinal vasculitis; choroidal granulomas)
- Autoimmune: sympathetic ophthalmia, Behçet disease, Vogt-Koyanagi-Harada syndrome
Sympathetic ophthalmia is a classic: penetrating eye injury exposes sequestered retinal antigens to conjunctival lymphatics → delayed-type hypersensitivity → bilateral panuveitis even in the uninjured eye. It famously blinded Louis Braille. Histology shows diffuse granulomatous inflammation of the entire uvea with melanin-laden granulomas and eosinophils (but plasma cells are absent). Treatment: systemic immunosuppression. May occur from 2 weeks to many years post-injury.
Uveal Melanoma
Uveal melanoma is the most common primary intraocular malignancy in adults. Incidence: ~5 per million/year.
Key molecular features (distinct from cutaneous melanoma):
- No BRAF mutations (unlike cutaneous melanoma)
- ~85% have gain-of-function mutations in GNAQ or GNA11 (G protein alpha subunits) → activate MAPK pathway
- Common secondary event: loss of chromosome 3 (monosomy 3) - associated with poor prognosis
- No clear link to UV light exposure
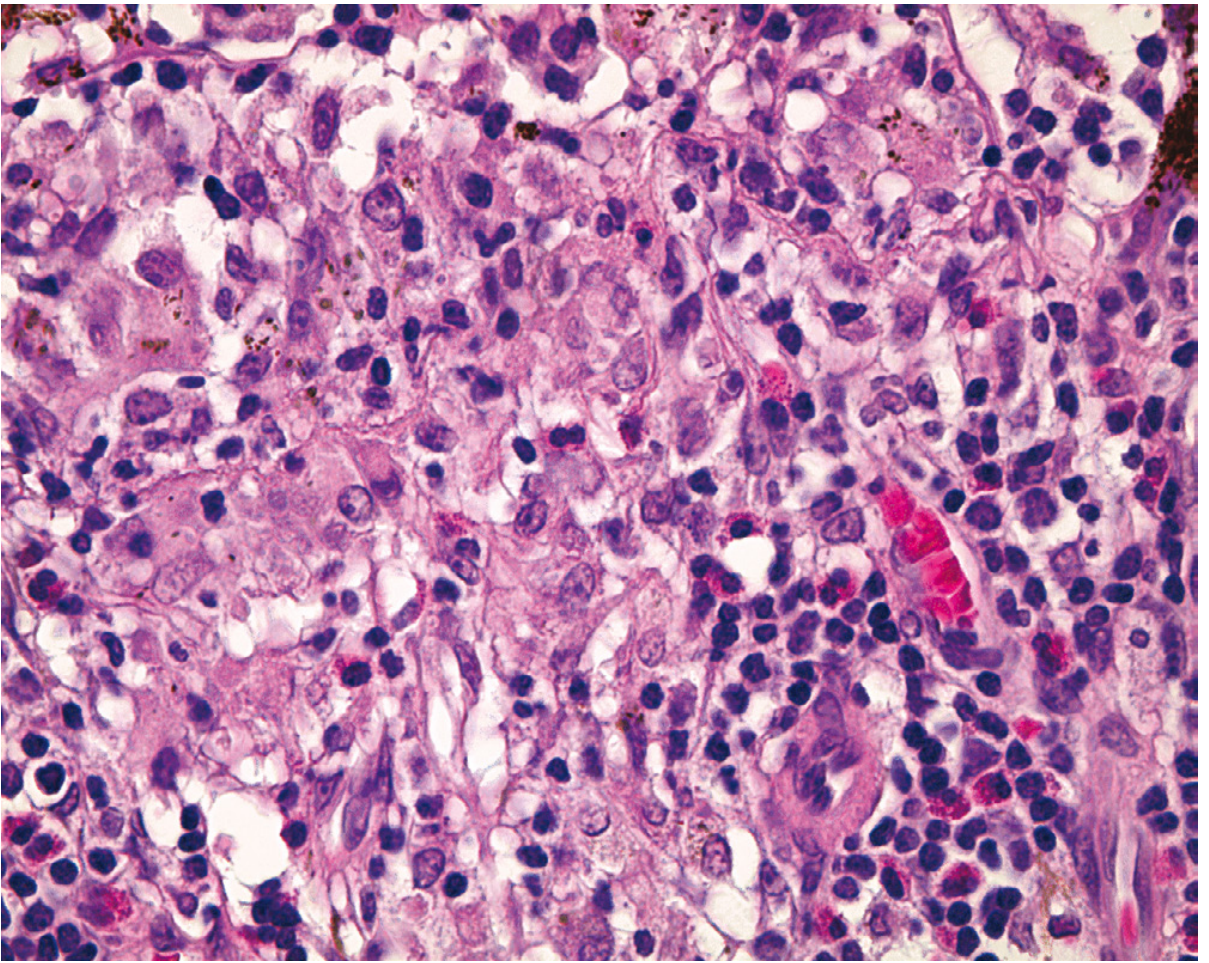
Histology: Two cell types - spindle cells (fusiform, better prognosis) and epithelioid cells (spherical, greater atypia, worse prognosis). Characteristic looping slitlike spaces lined by laminin surround packets of tumor cells, serving as extravascular conduits for plasma transport.
Spread: Almost exclusively hematogenous, with striking tropism for the liver (first site of metastasis in most cases).
Prognosis:
- 5-year survival ~80%
- Cumulative mortality reaches 40% at 10 years, continuing at ~1%/year
- Metastases may appear decades after treatment
Treatment: Radiotherapy (preferred) or enucleation - survival is equivalent between modalities. Iris melanomas are more indolent; ciliary body and choroidal melanomas are more aggressive.
Metastases to the uvea: The most common intraocular tumor overall is a metastasis (typically to the choroid) - lung cancer in males, breast cancer in females. Treatment is palliative (radiotherapy).
Summary Table
| Feature | Iris | Ciliary Body | Choroid |
|---|---|---|---|
| Location | Most anterior | Middle | Posterior |
| Key function | Pupil control | AH secretion, accommodation | Retinal nutrition |
| Key muscle | Sphincter/dilator pupillae | Ciliary muscle | - |
| Blood supply | Anterior ciliary aa. | Anterior ciliary aa. | Long/short posterior ciliary aa. |
| Key pathology | Traumatic mydriasis, iritis | Cyclitis, pars planitis | Choroiditis, melanoma, metastases |
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina), p. 2392-2398; Robbins & Kumar Basic Pathology, p. 870-871; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1213-1214; Firestein & Kelley's Textbook of Rheumatology, p. 4177.
This is a shared conversation. Sign in to Orris to start your own chat.