Describe peritonitis according to 20 marks question from SRB BOOK OF SURGERY
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
I now have all the content needed to write a comprehensive 20-mark SRB-style answer on peritonitis. Note: SRB's Manual of Surgery is not available in the library, but the content from Bailey & Love's Surgery (28th ed.) and other authoritative surgery texts covers all the same topics that SRB covers in this chapter.
PERITONITIS
(20 Marks Answer - SRB Surgery Style)
DEFINITION
Peritonitis is inflammation of the peritoneum (the serous membrane lining the abdominal cavity and covering the viscera). It may be localised or diffuse, acute or chronic, and is categorised most usefully in clinical practice by its extent (localised vs. generalised) and by its underlying aetiology.
CLASSIFICATION
A. By Extent
| Type | Description |
|---|---|
| Localised | Inflammation confined to one region; protective fibrin seals the area |
| Diffuse (Generalised) | Entire peritoneal cavity involved; life-threatening |
B. By Aetiology (Primary / Secondary / Tertiary)
- Primary (Spontaneous) Peritonitis - infection arises without any obvious intraabdominal source; seen in cirrhosis with ascites, nephrotic syndrome, children. Organisms: E. coli, streptococci, enterococci.
- Secondary Peritonitis - most common type; results from perforation or inflammation of an intraabdominal organ (e.g., perforated peptic ulcer, appendix, diverticulum).
- Tertiary Peritonitis - persistent or recurrent infection after treatment of secondary peritonitis, often in immunocompromised patients; typically polymicrobial with resistant organisms.
C. By Cause
Bacterial
- Gastrointestinal: perforated peptic ulcer, appendicitis, diverticulitis, typhoid perforation, colonic carcinoma perforation
- Non-gastrointestinal: pelvic inflammatory disease (Chlamydia, gonococci), haematogenous spread
Chemical
- Bile peritonitis (post-cholecystectomy bile leak)
- Barium peritonitis (barium enema leak)
- Urine peritonitis (bladder or ureteric injury)
Other
- Traumatic (operative handling)
- Ischaemic (strangulated bowel, mesenteric vascular occlusion)
- Allergic (starch peritonitis)
- Miscellaneous (familial Mediterranean fever, fungal peritonitis)
D. Routes of Peritoneal Contamination
- Gastrointestinal perforation (most common)
- Transmural bacterial translocation without perforation (pancreatitis, ischaemic bowel)
- Exogenous contamination (trauma, open surgery, peritoneal dialysis catheters)
- Female genital tract (ascending infection via fallopian tubes)
- Haematogenous spread (rare)
PATHOPHYSIOLOGY
When the peritoneum is contaminated:
- Vascular response - intense hyperaemia and increased capillary permeability; large volumes of protein-rich fluid pour into the peritoneal cavity ("third-space" loss).
- Inflammatory exudate - the fluid is initially serous, becomes turbid with leukocytes and plasma proteins, and may turn into frank pus.
- Fibrin deposition - fibrin is deposited on peritoneal surfaces causing loops of bowel and mesentery to adhere, potentially walling off the infection (localisation). At surgery, the peritoneum appears reddened, thickened with a velvety texture, with yellow/white fibrin plaques.
- Ileus - gut handling, inflammation, and toxins cause paralytic ileus with massive fluid sequestration into the gut lumen (third-space loss).
- Systemic response - massive fluid loss causes hypovolaemia, haemoconcentration, and electrolyte imbalance. The inflammatory cascade triggers SIRS (systemic inflammatory response syndrome), which may progress to septic shock and MODS (multi-organ dysfunction syndrome).
CLINICAL FEATURES
Symptoms
- Abdominal pain - the cardinal symptom; aggravated by movement, coughing, and deep respiration
- Anorexia, malaise, lassitude
- Nausea and vomiting
- Fever and rigors
- Constipation or obstipation (due to ileus)
Signs
General:
- Hippocratic facies - sunken eyes, dry tongue, pinched face; the patient lies still to minimise pain
- Pyrexia (may be absent in elderly/immunosuppressed)
- Tachycardia, hypotension (in advanced cases)
- Rapid shallow breathing
- Confusion and disorientation (advanced)
Abdominal:
- Generalised abdominal tenderness
- Involuntary guarding - reflex contraction of abdominal muscles to reduce peritoneal irritation
- Board-like rigidity - in diffuse peritonitis, the entire abdominal wall becomes rigid; in a thin patient, contracted rectus muscles give a scaphoid abdomen
- Rebound tenderness (Blumberg's sign) - pain worsens when examining hand is lifted off abdominal wall
- Absent or reduced bowel sounds - due to ileus
- Distended abdomen (in late paralytic ileus)
Special Signs:
- Shoulder tip (phrenic) pain - referred pain to C5 dermatome from subdiaphragmatic irritation
- Pelvic tenderness on digital rectal or vaginal examination - in pelvic peritonitis (appendix, salpingitis)
Note: Signs may be limited in obese patients or those on immunosuppressive medications.
INVESTIGATIONS
Laboratory
| Test | Findings |
|---|---|
| CBC | Leucocytosis (or leucopenia in severe sepsis) |
| Serum electrolytes | Hyponatraemia, hypokalaemia (from third-space losses) |
| Serum urea, creatinine | Elevated (pre-renal acute kidney injury) |
| Serum lactate | Elevated in sepsis/shock - important prognostic marker |
| LFTs, amylase, lipase | If hepatobiliary or pancreatic cause suspected |
| Blood cultures | To identify organism and guide antibiotics |
| Urine analysis | To exclude UTI; pregnancy test in females of childbearing age |
Radiology
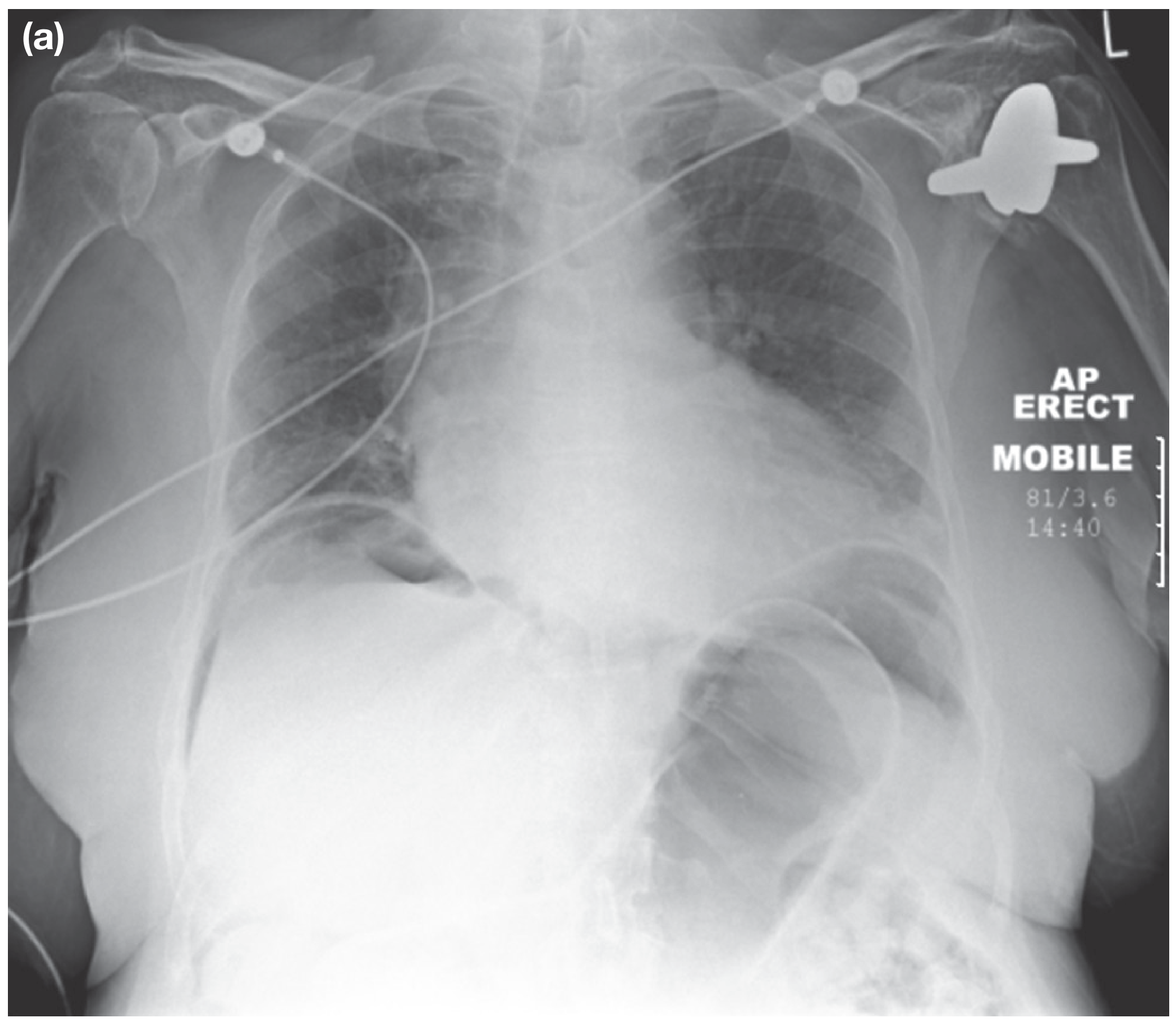
Erect Chest X-ray - the most important initial radiograph:
- Shows free gas (pneumoperitoneum) under the diaphragm - hallmark of viscus perforation
CT Abdomen (investigation of choice):
- Identifies underlying cause with high accuracy
- Shows free fluid, free gas, bowel wall thickening, localised collections, abscesses
- Guides percutaneous drainage

Ultrasound:
- Useful for pelvic pathology (tubo-ovarian), gallbladder, free fluid
- Less specific than CT for most causes
Lateral Decubitus X-ray:
- Alternative to erect CXR when patient is too ill to stand
Laparoscopy:
- When above investigations are inconclusive; allows both diagnosis and treatment
MANAGEMENT
Management follows a simultaneous resuscitation + investigation + operative approach.
I. Resuscitation and General Care ("Drip and Suck")
- IV access - large-bore cannula; aggressive IV fluid resuscitation with crystalloids (normal saline / Hartmann's solution)
- Nasogastric tube - decompresses stomach, reduces vomiting and risk of aspiration; monitors output
- Urinary catheter - monitors hourly urine output (target >0.5 mL/kg/hr as indicator of adequate resuscitation)
- Correction of electrolyte imbalance - particularly potassium, sodium
- Oxygen supplementation
- Monitoring - pulse, BP, temperature, urine output, oxygen saturation
II. Analgesia
- IV opioid analgesia (e.g., morphine) - does NOT mask signs when given judiciously
- Patient should NOT be left in pain while awaiting surgical evaluation
III. Antibiotics
- Broad-spectrum IV antibiotics to be started after blood cultures, and empirically before microbiology results
- Covers Gram-negative organisms, anaerobes, and Gram-positive cocci
- Common regimens:
- Amoxicillin + metronidazole + gentamicin, OR
- Co-amoxiclav + metronidazole, OR
- Third-generation cephalosporin (e.g., cefotaxime) + metronidazole
- In SBP: third-generation cephalosporin alone (avoids aminoglycoside nephrotoxicity)
- Duration guided by source control and clinical response
IV. Surgical Treatment - "Source Control"
Source control is the cornerstone of treatment for secondary peritonitis.
Aims of surgery:
- Remove or exclude the underlying cause (source control)
- Peritoneal lavage to dilute contamination
- Drainage of pus/collections
Specific procedures depending on cause:
| Cause | Operative Treatment |
|---|---|
| Perforated peptic ulcer | Graham patch repair / omental patch |
| Perforated appendix | Appendicectomy + lavage |
| Perforated diverticulum | Hartmann's procedure or primary resection + anastomosis |
| Biliary peritonitis | Laparotomy, lavage; ERCP + stent for localised bile leak |
| Perforated typhoid | Simple closure + lavage |
| Faecal peritonitis | Resection, temporary stoma formation |
Peritoneal lavage:
- Copious warm saline lavage (several litres) to dilute and physically remove bacteria and toxins
- Closed suction drains may be placed
Not all peritonitis requires surgery:
- A patient with localised left iliac fossa peritonitis due to diverticulitis may respond to IV antibiotics alone
- Decisions based on severity, haemodynamic stability, and clinical trajectory
V. Intensive Care / Vital System Support
- ICU admission for organ support (ventilation, vasopressors, renal replacement therapy)
- Management of SIRS, septic shock, and MODS
SPECIAL TYPES
1. Spontaneous Bacterial Peritonitis (SBP)
- Occurs in cirrhotic patients with ascites
- Diagnosis: paracentesis showing ascitic fluid neutrophil count >250/mm³
- Culture positive in only 40% of cases; most common organisms: E. coli, streptococci
- Treatment: third-generation cephalosporin (cefotaxime) IV; no surgery required
- Prophylaxis with norfloxacin in high-risk cirrhotics
2. Primary Pneumococcal Peritonitis
- Rare; mainly in children with nephrotic syndrome or cirrhosis
- Route: haematogenous or via vagina/fallopian tubes in girls
- Presents with sudden pain (lower abdomen), high fever (>39°C), vomiting, then profuse diarrhoea
- Organisms: H. influenzae, Group A streptococci, Gram-negative bacteria
- Treatment: antibiotics + surgery if not resolving
3. Biliary Peritonitis
- Post-cholecystectomy bile leak (clip slippage, accessory cystic duct)
- Investigation: LFTs, ERCP to identify leak source
- Treatment: percutaneous drain + ERCP stent for localised; surgical lavage for diffuse
4. Fitz-Hugh-Curtis Syndrome
- Perihepatitis caused by transperitoneal spread of Chlamydia/gonococci from pelvic infection
- Forms "violin string" adhesions on Glisson's capsule of the liver
COMPLICATIONS
Early:
- Septic shock
- SIRS and MODS
- Acute kidney injury (pre-renal)
- Respiratory failure (ARDS)
- Paralytic ileus
Late:
- Residual abscess formation (subphrenic, pelvic, paracolic)
- Adhesive intestinal obstruction
- Incisional hernia
- Enterocutaneous fistula
- Multi-organ failure and death
PROGNOSIS
- Mortality from secondary peritonitis remains high, particularly in the elderly and critically ill
- Factors worsening prognosis: delay in treatment, faecal contamination, immunosuppression, malignancy, multi-organ dysfunction
- Early aggressive resuscitation, timely source control, and appropriate antibiotics are the key determinants of survival
Sources: Bailey and Love's Short Practice of Surgery 28th Edition (pp.1109-1111); Current Surgical Therapy 14th Edition; Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Note: SRB's Manual of Surgery is not available in this library. The above answer is constructed from Bailey & Love and other authoritative surgery textbooks, and covers all standard headings (definition, classification, pathophysiology, clinical features, investigations, management, complications) as expected in SRB's treatment of this topic for a 20-mark question.
Gibe quick respknse of above question
PERITONITIS - Quick Summary
Definition
Inflammation of the peritoneum - localised or diffuse, acute or chronic.
Classification
- Primary - spontaneous (SBP in cirrhosis)
- Secondary - perforation of viscus (most common)
- Tertiary - recurrent/persistent in immunocompromised
Causes
- Bacterial: perforated peptic ulcer, appendicitis, diverticulitis, typhoid
- Chemical: bile, barium, urine
- Ischaemia, trauma, PID
Clinical Features
| Pain | Diffuse, worse on movement |
| Facies | Hippocratic facies |
| Abdomen | Board-like rigidity |
| Signs | Guarding + rebound tenderness |
| Sounds | Absent bowel sounds |
| Vitals | Tachycardia, fever, hypotension |
Investigations
- Erect CXR - free gas under diaphragm
- CT abdomen - investigation of choice
- Blood - TLC raised, lactate elevated
- Paracentesis - in SBP (neutrophils >250/mm³)
Management ("Drip and Suck")
- IV fluids - aggressive resuscitation
- NGT + catheter - decompress + monitor
- IV broad-spectrum antibiotics - cephalosporin + metronidazole
- Analgesia - IV morphine
- Surgery - source control + peritoneal lavage
Complications
- Early: Septic shock, AKI, ARDS, MODS
- Late: Abscess, adhesions, fistula, death
Search for recent clinical guidelines on peritonitis treatment
Searching PubMed
"peritonitis"[MeSH Terms] AND "guideline"[pt]
Searching the Web
peritonitis treatment guidelines 2024 2025 WSES IDSA intraabdominal infection
Reading Article
PMID: 33942342
Reading Article
PMID: 35264029
Searching PubMed
"intra-abdominal infection" AND "guideline" AND "antibiotic"
Reading Web Page
https://emedicine.medscape.com/article/180234-treatment
Reading Article
PMID: 38990709
Reading Article
PMID: 41083248
Searching the Web
WSES guidelines secondary peritonitis 2023 2024 source control antibiotics
Here is a comprehensive synthesis of the most recent clinical guidelines on peritonitis treatment:
Recent Clinical Guidelines on Peritonitis Treatment
Key Guideline Documents (2022-2025)
| Guideline | Year | Organisation | Focus |
|---|---|---|---|
| SIS Guidelines on IAI Management: 2024 Update | 2024 | Surgical Infection Society | Adult intra-abdominal infection (IAI) |
| IDSA Guideline Update on Complicated IAI | 2024 | IDSA | Risk assessment, imaging, microbiology |
| WSES/GAIS/SIS Source Control Guidelines | 2023 | WSES + multi-society | Source control in emergency surgery |
| ISPD Peritonitis Guideline: 2022 Update | 2022 | Int. Society for Peritoneal Dialysis | PD-associated peritonitis |
| AASLD SBP Guidance | 2021 | American Assoc. for Study of Liver Diseases | Spontaneous bacterial peritonitis |
| SIS Pediatric IAI Guidelines | 2025/2026 | SIS | Paediatric peritonitis [PMID: 41083248] |
1. SOURCE CONTROL (Most Critical Recommendation)
SIS 2024 / WSES 2023 - Strong Recommendation (Grade 1A):
- Source control is the single most important intervention in secondary peritonitis
- Timing: Should be achieved as soon as feasible - ideally within 6-12 hours of diagnosis in haemodynamically unstable patients
- Delayed source control (>12 hours) is independently associated with increased mortality
- Options: surgery, percutaneous drainage (radiologically guided), or endoscopic approaches - choose the least invasive method capable of effective control
- Damage control surgery (abbreviated laparotomy + temporary abdominal closure) is recommended for haemodynamically unstable patients
2. ANTIBIOTIC THERAPY
Risk Stratification (SIS 2024 / IDSA 2024)
Patients are stratified into low-risk vs high-risk before antibiotic selection:
Low-Risk (Community-acquired, no resistant organism risk factors):
| Regimen | Examples |
|---|---|
| Beta-lactam/beta-lactamase inhibitor | Amoxicillin-clavulanate, Piperacillin-tazobactam |
| Cephalosporin + metronidazole | Cefazolin/ceftriaxone + metronidazole |
| Carbapenem (ertapenem) | For mild-moderate community infections |
| Fluoroquinolone + metronidazole | Only if local resistance rates allow |
High-Risk (Hospital-acquired, immunocompromised, resistant organism risk, post-operative):
| Regimen | Examples |
|---|---|
| Anti-pseudomonal carbapenem | Meropenem, imipenem-cilastatin |
| Piperacillin-tazobactam | Broad Gram-negative + anaerobe cover |
| New combinations (MDR) | Ceftolozane-tazobactam, ceftazidime-avibactam |
| NEW (FDA 2025) | Aztreonam/avibactam - approved Feb 2025 for cIAI due to specific resistant Gram-negatives (MDR E. coli, Klebsiella, Enterobacter, Serratia) - reserved for cases with few alternatives |
Antibiotic Duration (SIS 2024 - Major Update)
- Adequate source control achieved: 4 days (96 hours) is sufficient - do not extend beyond this
- This represents a significant shortening from older practice (7-14 days)
- Supported by the STOP-IT trial showing 4 days = 8 days with no difference in outcomes
- If source control is inadequate or not achievable: continue until achieved + 4 days
De-escalation (SIS 2024)
- Review antibiotic choice at 48-72 hours based on culture results
- Narrow spectrum once organism and sensitivities known (antibiotic stewardship)
- Stop antifungals if Candida not confirmed on cultures
Anti-enterococcal Therapy
- Routine empiric anti-enterococcal coverage not recommended for community-acquired infections
- Consider for: healthcare-associated infections, immunocompromised patients, post-operative peritonitis
Antifungal Therapy
- Routine empiric antifungals not recommended for most community-acquired infections
- Indicated for: recurrent bowel perforations, prolonged hospital/ICU stay, immunosuppression
- Drug of choice: Fluconazole (if non-resistant Candida); echinocandin for resistant/invasive candidiasis
3. SPONTANEOUS BACTERIAL PERITONITIS (AASLD 2021)
Diagnosis:
- Ascitic fluid PMN (polymorphonuclear cell) count ≥250 cells/mm³ - diagnostic even without positive culture
- "Culture-negative neutrocytic ascites" treated the same as SBP
Treatment:
- First-line: IV Cefotaxime 2g q8h x 5 days (or ceftriaxone)
- Alternative: Amoxicillin-clavulanate (oral in non-severe cases)
- Albumin infusion: 1.5 g/kg IV at diagnosis + 1 g/kg on day 3 - reduces hepatorenal syndrome risk and mortality
- Avoid aminoglycosides (nephrotoxic in cirrhosis)
Prophylaxis (primary/secondary):
- Norfloxacin 400 mg/day (or ciprofloxacin 500 mg/day) for long-term secondary prophylaxis
- Primary prophylaxis for ascitic protein <1.5 g/dL + impaired renal/liver function
4. PD-ASSOCIATED PERITONITIS (ISPD 2022)
New performance target: Overall peritonitis rate ≤0.40 episodes/patient-year at risk (>80% of patients peritonitis-free per year)
Empiric antibiotics (intraperitoneal preferred):
- Gram-positive cover: Vancomycin (especially MRSA risk) or first-generation cephalosporin
- Gram-negative cover: Third-generation cephalosporin or aminoglycoside
- Oral N-acetylcysteine recommended to mitigate aminoglycoside ototoxicity (new 2022 recommendation)
- Catheter removal for refractory, relapsing, or fungal peritonitis
5. PAEDIATRIC PERITONITIS (SIS 2025/2026 - PMID 41083248)
- Principles same as adults but antibiotic dosing adjusted for weight
- Preferred antibiotics: amoxicillin-clavulanate, ceftriaxone + metronidazole, piperacillin-tazobactam
- Short antibiotic course (4 days) after source control also recommended
Key Takeaways from 2022-2025 Guidelines
| Principle | Current Recommendation |
|---|---|
| Source control timing | As early as possible; <12 hours in septic shock |
| Antibiotic duration | 4 days post-source control (not 7-14 days) |
| De-escalation | Mandatory at 48-72 hours based on cultures |
| Antifungals | Not routine; only in high-risk/confirmed cases |
| Anti-enterococcal | Not routine in community-acquired cases |
| SBP treatment | Cefotaxime + albumin infusion |
| New drug (2025) | Aztreonam/avibactam for MDR Gram-negatives |
Give 20 marks anwer from love and bailey
Reading File
Reading File
I now have all the content directly from Bailey & Love. Here is the complete 20-mark answer drawn exclusively from Bailey & Love's Short Practice of Surgery, 28th Edition (Chapter 65):
PERITONITIS
Bailey & Love's Short Practice of Surgery, 28th Edition - Chapter 65
DEFINITION
Peritonitis is inflammation of the peritoneum. It can be categorised as localised or diffuse, acute or chronic, or according to the primary underlying pathology. In clinical practice, the most useful categorisation is based on whether it is localised or diffuse.
PERITONEAL ANATOMY (relevant background)
The peritoneum has the capacity to absorb large volumes of fluid; however, it can also produce large volumes of fluid (ascites) and an inflammatory exudate when injured. During expiration, intra-abdominal pressure is reduced and peritoneal fluid travels upward toward the diaphragm. Particulate matter and bacteria are absorbed within minutes into the lymphatic network through pores in the diaphragmatic peritoneum. The circulation of peritoneal fluids explains why abscesses can form at sites anatomically remote from the primary disease. The two sites most prone to collection are the pelvis (gravity when standing) and subdiaphragmatic areas (gravity when lying).
CAUSES OF PERITONEAL INFLAMMATION
(Bailey & Love - Summary Box 65.2)
| Category | Examples |
|---|---|
| Bacterial - GI | Perforated appendix, ulcer, diverticulum, typhoid |
| Bacterial - non-GI | PID (Chlamydia, gonococci), haematogenous |
| Chemical | Bile, barium |
| Allergic | Starch peritonitis |
| Traumatic | Operative handling |
| Ischaemic | Strangulated bowel, vascular occlusion |
| Miscellaneous | Familial Mediterranean fever |
ROUTES OF PERITONEAL INFECTION
(Bailey & Love - Summary Box 65.3)
- Gastrointestinal perforation - e.g. perforated ulcer, appendix, diverticulum
- Transmural translocation (no perforation) - e.g. pancreatitis, ischaemic bowel, primary bacterial peritonitis
- Exogenous contamination - e.g. drains, open surgery, trauma, peritoneal dialysis
- Female genital tract infection - e.g. pelvic inflammatory disease
- Haematogenous spread (rare) - e.g. septicaemia
A. LOCALISED PERITONITIS
Definition
A localised area of the peritoneum becomes inflamed. If the parietal peritoneum is involved, the patient complains of somatic pain in the area affected.
Clinical Features
- Vital signs may be normal; tachycardia and pyrexia are common
- Involuntary guarding - reflex abdominal wall contraction to reduce further peritoneal irritation
- Rebound tenderness - worsening of pain on lifting the examining hand off the abdominal wall
- These signs collectively are termed peritonism; the patient is described as peritonitic
Special Features
- Shoulder tip ('phrenic') pain - if inflammation arises under the diaphragm; referred pain to the C5 dermatome
- Pelvic peritonitis (e.g. from inflamed appendix or salpingitis) - abdominal signs may be limited; deep-seated tenderness detected on digital rectal or vaginal examination
- Signs may be limited in obese patients or patients on immunosuppressive medications
Operative Appearance
At surgery, the inflamed peritoneum appears:
- Reddened, thickened with a velvety texture
- Plaques of yellow/white fibrin causing loops of intestine and mesentery to adhere to themselves and to the parietes
- A reactionary serous exudate (rich in leukocytes and plasma proteins) that gradually becomes turbid, transforming to frank pus if not evacuated
Diagnosis
- History and physical examination, supplemented by laboratory and radiological investigations
- Laboratory biomarkers support acute inflammation but are rarely diagnostically specific
- Investigation of choice: CT scanning
- Ultrasound can be used but lacks specificity except for tubo-ovarian pathology
- Laparoscopy may be required if above investigations are inconclusive
Treatment
Aims to remove the underlying cause and to lavage or dilute residual contamination.
B. DIFFUSE (GENERALISED) PERITONITIS
Definition
Regions (not just focal areas) of the parietal peritoneum are inflamed - normally signifies life-threatening pathology.
Causes
- Pressure-related perforation of a viscus (e.g. obstructed colon)
- Large volumes of blood entering the peritoneal cavity abruptly (e.g. ruptured aortic aneurysm)
- Substantial volumes pouring continuously (e.g. perforated duodenal ulcer or anastomotic leak)
Symptoms
- Acute or gradual onset abdominal pain of considerable intensity
- Pain may be localised at first, then become diffuse
Signs
- Patient appears gravely ill (Hippocratic facies) and lies as still as possible to minimise fluid movement
- Entire abdominal musculature undergoes reflex contraction - board-like rigidity on palpation
- In a thin patient, rectus abdominis contraction gives a scaphoid appearance of the abdomen
- Generalised ileus - abdomen may become distended
- Vital signs deranged - hypotension, tachycardia, pyrexia
- Patient may appear confused, drowsy, disoriented; progressing to loss of consciousness if untreated
SUMMARY OF CLINICAL FEATURES
(Bailey & Love - Summary Box 65.4)
- Abdominal pain, worse on movement, coughing and deep respiration
- Constitutional upset: anorexia, malaise, fever, lassitude
- Gastrointestinal upset: nausea ± vomiting
- Pyrexia (may be absent)
- Raised pulse rate
- Tenderness ± guarding/rigidity/rebound of abdominal wall
- Pain/tenderness on rectal/vaginal examination (pelvic peritonitis)
- Absent or reduced bowel sounds
- Septic shock (SIRS and MODS) in later stages
INVESTIGATIONS
- Erect Chest X-ray - identifies subdiaphragmatic free gas (pneumoperitoneum), hallmark of viscus perforation
- CT abdomen - investigation of choice; identifies the underlying cause precisely
- If patient is particularly unwell and CT is unavailable, a lateral decubitus radiograph serves the same purpose as erect CXR (patient must be correctly positioned long enough for gas to rise within the peritoneal cavity)
- Investigation and treatment must be undertaken expediently as the time available to salvage may be limited
MANAGEMENT
(Bailey & Love - Summary Box 65.5)
General Care of Patient
| Step | Detail |
|---|---|
| IV fluid resuscitation | Correct fluid and electrolyte imbalance |
| Nasogastric drainage tube | Decompress stomach, reduce vomiting |
| Urinary catheter | Monitor hourly urine output |
| Broad-spectrum antibiotic therapy | Started empirically and early |
| Analgesia | IV opioids (does not mask signs when given judiciously) |
| Vital system support | ICU monitoring as required |
Surgical Treatment - Source Control
- Surgical treatment of cause when appropriate
- 'Source control' by removal or exclusion of the cause
- Peritoneal lavage ± drainage
"Not all patients with peritonitis require surgery. For example, a patient with localised LLQ peritonitis secondary to diverticulitis may respond to IV antibiotics alone."
SPECIFIC TYPES OF PERITONITIS (Bailey & Love)
1. Acute Bacterial Peritonitis
Most commonly arises from perforation of a viscus of the alimentary tract. Less common forms involve primary 'spontaneous' peritonitis due to streptococcal, pneumococcal, or Haemophilus infection.
2. Non-Gastrointestinal Bacterial Peritonitis
- Pelvic infection via Fallopian tubes - most common offending organisms: Chlamydia spp. and gonococci
- These organisms thin cervical mucus, allow vaginal bacteria to ascend to uterus and oviducts
- Fitz-Hugh-Curtis syndrome - variant of transperitoneal spread causing perihepatitis with scar tissue on Glisson's capsule
- Fungal peritonitis - rare; may complicate severely ill patients
3. Biliary Peritonitis
- Mostly seen after cholecystectomy - from slippage of a clip off the cystic duct, drainage from an accessory cystic duct, or perforation of the common bile or hepatic duct
- Also after hepatectomy or duodenal surgery
- Localised collections: percutaneous drain + ERCP to identify bile leak and place stent
- Diffuse/high-volume contamination: surgical exploration with lavage and drainage
4. Spontaneous Bacterial Peritonitis (SBP)
- Acute bacterial infection of ascitic fluid - often in cirrhosis
- Clinical picture highly variable - patient may be asymptomatic; course can be prolonged
- Diagnosis: paracentesis - ascitic fluid neutrophil count >250/mm³ (even if culture negative)
- Culture positive in only ~40% of patients; most common organisms: Gram-negative bacteria (E. coli), Gram-positive cocci (streptococci, enterococci)
- Treatment: empirical antibiotics immediately after diagnosis
- First-line: third-generation cephalosporin (e.g. cefotaxime) - avoids renal toxicity of aminoglycosides
- Alternatives: amoxicillin/clavulanic acid, quinolones (e.g. ciprofloxacin)
5. Primary Pneumococcal Peritonitis
- Incidence has declined greatly; now rare
- Affects children with nephrotic syndrome or cirrhosis; otherwise healthy children also affected
- Route: vagina and Fallopian tubes in girls; blood-borne secondary to respiratory tract or middle-ear disease
- Symptoms: sudden onset pain (lower abdomen), temperature ≥39°C, frequent vomiting; after 24-48 hours - profuse diarrhoea (characteristic) and increased urinary frequency
- Signs: peritonism usually diffuse but less prominent than in perforated viscus
- Organisms: Haemophilus spp., Group A streptococci, Gram-negative bacteria
- Treatment: antibiotics + correct dehydration/electrolytes; early surgery unless SBP strongly suspected
COMPLICATIONS
Immediate:
- Septic shock (SIRS → MODS)
- Acute kidney injury
- Respiratory failure
Late:
- Subphrenic or pelvic abscess
- Adhesive intestinal obstruction
- Enterocutaneous fistula
- Death
Source: Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 65 - The Peritoneum, Omentum, Mesentery and Retroperitoneal Space, pp. 1109-1112
This is a shared conversation. Sign in to Orris to start your own chat.