General anaesthesia premedication complete topic
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have comprehensive content from multiple authoritative anaesthesia textbooks. Let me compile the complete answer.
General Anaesthesia - Premedication: Complete Topic
Definition and Historical Background
Premedication refers to drugs administered before anaesthesia to facilitate induction and maintenance, improve patient comfort, reduce risks, and achieve a number of specific pharmacological goals. It was originally introduced in the 19th century to reduce the amount of chloroform required and speed the onset of surgical anaesthesia. Morphine derivatives combined with an anticholinergic antisialagogue (atropine) were the original combination - reducing anxiety and facilitating anaesthesia.
With the advent of faster-acting anaesthetics and the rise of day-case surgery and same-day admissions, sedative premedication has largely fallen out of favour in modern practice. However, several premedication categories remain clinically important for safety and facilitation.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
Goals of Premedication
The goals of premedication administration include:
- Anxiolysis - reduction of preoperative anxiety and fear
- Sedation - calming effect before transport to the operating theatre
- Amnesia (anterograde) - preventing recall of preoperative events and procedures
- Vagolysis / sympathicolysis - attenuating autonomic responses
- Reduction of PONV (postoperative nausea and vomiting)
- Analgesia - pre-emptive pain management
- Antisialagogue effect - drying secretions, particularly before airway manipulation
- Aspiration prophylaxis - reducing risk and severity of pulmonary aspiration
- Reduction in anaesthetic requirements (reducing MAC)
- Minimising sympathetic activation - important in patients with CAD, hypertension
- Miller's Anesthesia, 10e
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Classes of Premedicant Drugs
1. Benzodiazepines (Most Commonly Used)
Benzodiazepines are the most commonly administered drugs for premedication. They achieve anxiolysis, sedation, amnesia, and PONV reduction. Amnestic effects are anterograde - retrograde memory is not affected.
Key Agents and Doses
| Drug | Oral Dose (Adults) | Special Notes |
|---|---|---|
| Midazolam | 7.5-15 mg | Most frequently used in adults AND children; rapid onset; minimal respiratory effects |
| Diazepam | 5-10 mg | Longer acting; useful for preoperative night sedation |
| Temazepam | 10-20 mg | Short-acting; commonly used in day-case settings |
| Lorazepam | 2-4 mg orally, 2h pre-op | Used when prolonged/intense anxiolysis is required (e.g. cardiac surgery) |
Midazolam is the most frequently used benzodiazepine for premedication in both adults and children. It has minimal effects on respiration and oxygen saturation even at doses up to 1.0 mg/kg.
Paediatric note: For children, midazolam 0.025 mg/kg produces sedation and anxiolysis in 10-20 minutes. It is available in oral, intranasal, and IV preparations.
Duration considerations:
- Midazolam and diazepam: similar early plasma decay (redistribution) - similar recovery
- Lorazepam: slower onset, longer and unpredictable amnesia - undesirable when patients need recall in the immediate postoperative period
Safety: Administration of benzodiazepines for premedication is well tolerated with no evidence of increased mortality, including in patients aged 80 or older.
- Miller's Anesthesia, 10e
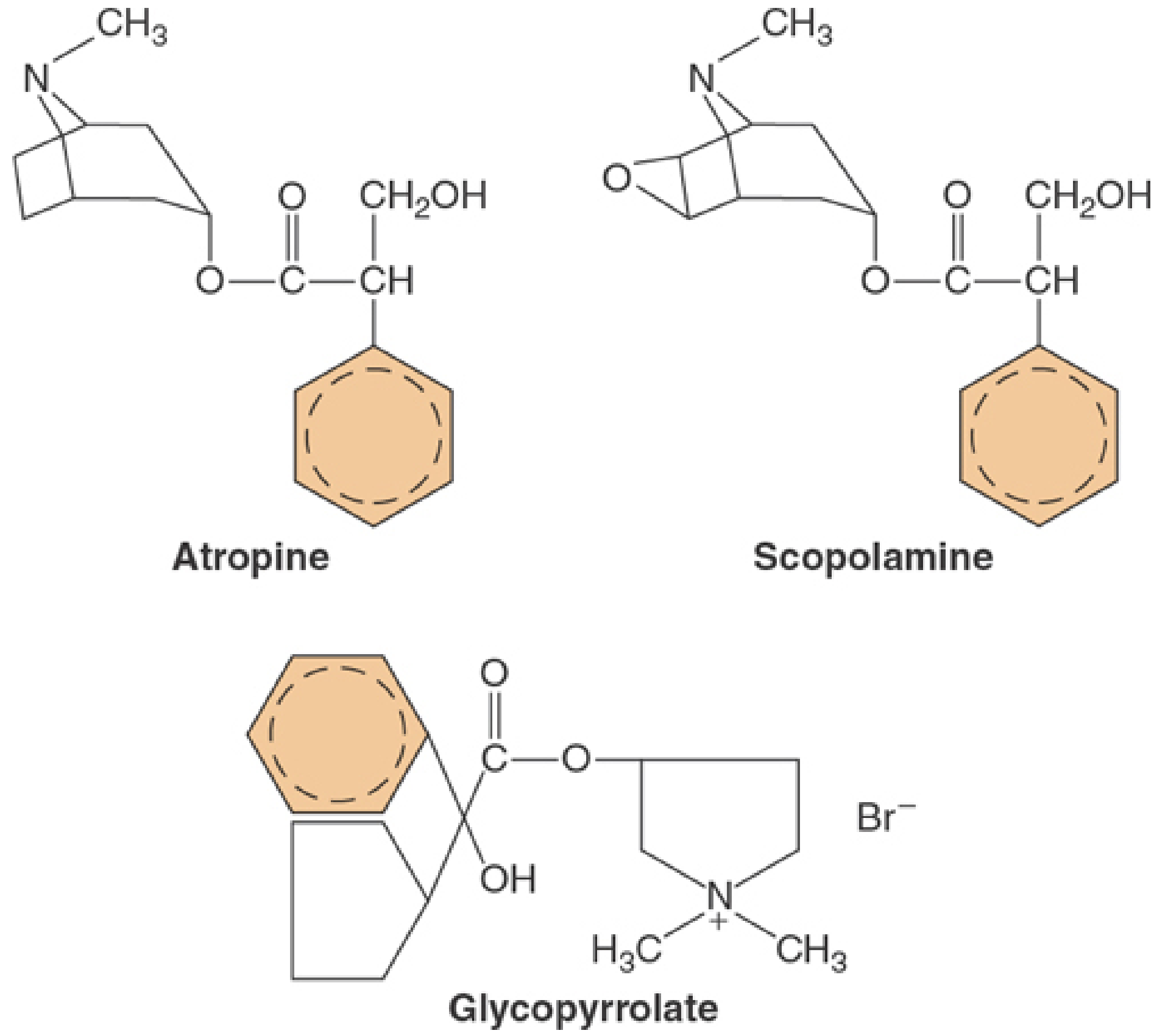
2. Anticholinergic (Antimuscarinic) Agents
Three agents are used: atropine, scopolamine (hyoscine), and glycopyrrolate.
Mechanism
Competitive inhibitors of ACh at parasympathetic muscarinic receptors. Actions include:
- Inhibition of salivary, bronchial, pancreatic, and GI secretions (antisialagogue)
- Increased heart rate
- Bronchodilation
- Reduced GI motility
- Attenuation of gastric acid production
- Antagonism of muscarinic side effects of anticholinesterases (neuromuscular reversal)
Historically introduced to prevent excessive secretions and vagal bradycardia during open-drop ether/chloroform anaesthesia.
Comparison Table
| Property | Atropine | Scopolamine | Glycopyrrolate |
|---|---|---|---|
| Drug type | Tertiary amine (belladonna alkaloid) | Tertiary amine (belladonna alkaloid) | Quaternary amine (synthetic) |
| Crosses BBB? | Yes | Yes | No |
| Crosses placenta? | Yes | Yes | No |
| Duration IV | 15-30 min | 30-60 min | 2-4 h |
| Duration IM | 2-4 h | 4-6 h | 6-8 h |
| CNS effects | Mild stimulation (low dose); delirium (high dose) | Sedation, amnesia, euphoria | None |
| Antisialagogue | + | +++ | ++ |
| Heart rate increase | +++ | + (minimal IM) | + |
Clinical Notes:
-
Scopolamine was historically used for premedication in cardiac/major surgery (sedation + amnesia + antisialagogue). It is now used mainly for motion sickness and PONV prophylaxis (transdermal patch).
-
Glycopyrrolate is now the preferred agent in anaesthesia because it: (1) does not cross the BBB (no CNS side effects), (2) has longer duration, (3) is a better antisialagogue. Particularly important before fibreoptic intubation where a dry airway is essential.
-
Atropine: preferred for symptomatic bradyarrhythmias; use with extreme caution when tachycardia is deleterious (coronary artery stenosis, HOCM, aortic stenosis, phaeochromocytoma, thyroid storm).
-
Caution in elderly: Centrally acting anticholinergics (atropine, scopolamine) may contribute to postoperative confusion. Glycopyrrolate is preferred in older patients.
-
Paradox: Very low doses of atropine (<0.1 mg) may paradoxically decrease heart rate via blockade of presynaptic M1 receptors.
-
Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
-
Morgan and Mikhail's Clinical Anesthesiology, 7e
3. Opioids
Morphine and its derivatives were among the original premedicant drugs. In modern practice, opioid premedication is used in specific contexts:
- Cardiac surgery patients: narcotics reduce anxiety and pain preoperatively; commonly fentanyl IV given with midazolam before invasive catheter placement
- Patients with significant pain requiring analgesic premedication
- To blunt the haemodynamic response to intubation (given at induction rather than as true premedication)
Caution: In patients with low cardiac output from congestive heart failure or significant pulmonary hypertension, opioid sedation must be judicious - avoid myocardial depression, hypercapnia, and hypoxia from respiratory depression.
- Miller's Anesthesia, 10e (cardiac surgery chapter)
- Morgan and Mikhail's Clinical Anesthesiology, 7e
4. Aspiration Prophylaxis Agents
Pulmonary aspiration of gastric contents can cause severe Mendelson's syndrome (chemical pneumonitis). High-risk patients include those with:
- Diabetes mellitus
- Renal impairment
- Obesity
- Gastro-oesophageal reflux disease (GORD)
- Pregnancy
- Full stomach / emergency surgery
Agents Used:
| Drug Class | Examples | Mechanism / Purpose |
|---|---|---|
| H2 blockers | Ranitidine | Reduce gastric acid secretion |
| Proton pump inhibitors | Omeprazole | Reduce gastric acid secretion (more potent) |
| Gastric alkalinizers | Sodium citrate (0.3M) | Raises gastric pH immediately; used for rapid sequence |
| Prokinetics | Metoclopramide | Accelerates gastric emptying; increases lower oesophageal sphincter tone |
The combination of a non-particulate antacid (sodium citrate) + H2 blocker or PPI + metoclopramide is often used in high-risk patients (e.g., obstetric patients for caesarean section).
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1
5. Analgesics (Pre-emptive Analgesia)
Paracetamol and NSAIDs can be administered orally prior to surgery for pre-emptive analgesia. These are well absorbed and cost-effective.
Evidence note: Evidence that pre-emptive oral analgesia is superior to similar treatment initiated post-surgery is weak, despite widespread use.
Caution with NSAIDs:
-
Elderly patients
-
Patients with dyspeptic symptoms
-
Renal impairment
-
Altered platelet function and coagulation - consideration in certain surgeries
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1
6. Antiemetics
Antiemetic premedication is indicated in high-risk PONV patients. Transdermal scopolamine patch is one option; ondansetron and dexamethasone may also be given prophylactically.
7. Continuation of Regular Medications
A fundamental principle: patients should generally continue their usual long-term medications on the day of surgery, with some exceptions:
| Drug | Perioperative Policy |
|---|---|
| Beta-blockers | Continue - abrupt withdrawal can precipitate rebound ischaemia/tachycardia |
| Statins | Continue - perioperative benefit |
| ACE inhibitors | Use caution - may increase propensity for intraoperative hypotension if given on day of surgery |
| Aspirin | Elective cases: discontinue pre-op to reduce bleeding/transfusion requirements (STS guidelines); continue if acute coronary syndrome |
| P2Y12 inhibitors (e.g., clopidogrel) | Discontinue before operative coronary revascularisation; interval based on pharmacodynamics (≥3 days for irreversible inhibitors) |
| Antianginal drugs / nitrates | Continue beta-blockers; prophylactic IV nitrates provide no benefit unless ongoing ischaemia |
Special Populations
Cardiac Surgery Patients
- Premedication (narcotic ± anxiolytic) is indicated before transport to OR
- Supplemental IV midazolam ± fentanyl commonly given during radial artery cannulation before induction
- Oversedation must be avoided in low CO states (CHF) - may cause myocardial depression and hypotension
- In pulmonary hypertension: avoid respiratory depression causing hypercapnia/hypoxia
Hypertensive Patients
- Anxiolytic premedication (e.g., midazolam) resolves mild-to-moderate "white coat" hypertension
Coronary Artery Disease Patients
- Premedication goal: minimise sympathetic activation (adverse effect on myocardial O2 supply-demand balance)
- Limit to small doses of IV midazolam (± small opioid dose) immediately before invasive procedures
- Overmedication is equally detrimental - hypoxaemia, respiratory acidosis, hypotension
Elderly Patients
- Avoid centrally acting anticholinergics (risk of postoperative confusion)
- Use glycopyrrolate if anticholinergic required
- Caution with NSAIDs (renal function, GI risk)
Paediatric Patients
-
Oral/intranasal midazolam widely used
-
Parental presence at induction reduces anxiety and may be preferred over pharmacological premedication
-
Miller's Anesthesia, 10e
-
Morgan and Mikhail's Clinical Anesthesiology, 7e
-
Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
Modern Trends and Practical Considerations
- Sedative premedication is seldom used in modern anaesthetic practice, especially with the growth of day-case surgery - patients require early ambulation and discharge
- Antiemetic and antacid prophylaxis remain important for high-risk patients
- The original morphine-atropine combination still has occasional use before anticipated difficult/fibreoptic intubation (antisialagogue + analgesia/sedation)
- Patient education and reassurance is recognised as the first step in reducing anxiety - thorough explanation of anticipated anaesthetic techniques reduces the need for pharmacological anxiolysis
- Pre-operative oral simple analgesics remain cost-effective despite weak evidence for pre-emptive benefit
Summary Table
| Drug Category | Primary Goal | Key Agents | Route | Timing |
|---|---|---|---|---|
| Benzodiazepines | Anxiolysis, amnesia, sedation | Midazolam, temazepam, lorazepam | PO, IV | 30-60 min pre-op (PO) |
| Anticholinergics | Antisialagogue, vagolysis | Glycopyrrolate, atropine, scopolamine | IM, IV | 30-60 min pre-op |
| Opioids | Analgesia, sedation | Morphine, fentanyl | IM, IV | Variable |
| Antacids/H2/PPI | Aspiration prophylaxis | Sodium citrate, ranitidine, omeprazole, metoclopramide | PO | 1-2 h pre-op |
| Analgesics | Pre-emptive analgesia | Paracetamol, NSAIDs | PO | 1 h pre-op |
| Antiemetics | PONV prophylaxis | Scopolamine (transdermal), ondansetron | Transdermal, IV | Night before / 1 h pre-op |
Sources: Miller's Anesthesia 10e | Morgan and Mikhail's Clinical Anesthesiology 7e | Barash, Cullen and Stoelting's Clinical Anesthesia 9e | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 | Bailey and Love's Short Practice of Surgery 28e
Please give explanation of the terminology of hard words on this topic
Here is a plain-language explanation of every hard or technical term used in the premedication topic above:
Terminology Explained - General Anaesthesia Premedication
A
Amnesia (Anterograde)
Loss of ability to form new memories after a drug is given. The patient cannot recall what happened during the procedure. Retrograde amnesia = forgetting what happened before the drug - benzodiazepines do NOT cause this.
Analgesic
A painkilling drug. "Pre-emptive analgesia" means giving a painkiller before surgery to reduce post-operative pain.
Anxiolysis / Anxiolytic
Anxiety relief. An anxiolytic drug reduces fear and worry without necessarily causing deep sleep.
Antisialagogue
A drug that reduces saliva production. "Sialo" = saliva; "gogue" = producing. Important before airway procedures so the throat stays dry and the anaesthetist can see clearly.
Antimuscarinic
A drug that blocks muscarinic receptors (a type of receptor for acetylcholine). Also called anticholinergic. Produces dry mouth, raised heart rate, and reduced gut movement.
Anticholinergic
A drug that blocks the action of acetylcholine (a nerve chemical). In anaesthesia, used to dry secretions, prevent slow heart rate, and reduce gut activity.
Anticholinesterase
A drug that blocks the enzyme which breaks down acetylcholine - thus increasing acetylcholine levels. Used to reverse muscle relaxants (e.g. neostigmine). Anticholinergics are given alongside to prevent unwanted side effects.
ASA Physical Status
American Society of Anesthesiologists classification. A grading system (ASA I to VI) that describes a patient's overall health before surgery. Helps determine anaesthetic risk.
Atropine
A naturally occurring drug from the belladonna plant. A tertiary amine anticholinergic. Raises heart rate strongly, mildly reduces secretions. Crosses the blood-brain barrier.
B
Belladonna Alkaloid
A naturally occurring chemical from the "deadly nightshade" plant (belladonna). Atropine and scopolamine are examples. Historically used as both poison and medicine for thousands of years.
Benzodiazepine
A class of drug that works on GABA receptors in the brain, producing sedation, anxiolysis, muscle relaxation, and amnesia. Examples: midazolam, diazepam, lorazepam, temazepam.
Blood-Brain Barrier (BBB)
A protective layer of tightly packed cells around brain blood vessels that prevents many substances from entering the brain from the bloodstream. Tertiary amines (atropine, scopolamine) cross it; quaternary amines (glycopyrrolate) do not.
C
Cardiac Output (CO)
The amount of blood the heart pumps per minute (litres/min). Low CO = the heart is pumping weakly, as in heart failure.
Cholinesterase
An enzyme that breaks down acetylcholine. "Anticholinesterase" blocks this enzyme, preserving acetylcholine.
Competitive Inhibitor
A drug that blocks a receptor by occupying it, but the block can be overcome by more of the natural chemical. Anticholinergics competitively block muscarinic receptors.
Cycloplegia
Paralysis of the ciliary muscle of the eye, causing inability to focus (accommodation). A side effect of anticholinergics.
D
Dysarthria
Slurred or difficult speech. Used as a clinical endpoint when titrating sedation - once the patient slurs words, adequate sedation has been reached.
E
Euphoria
A feeling of intense happiness or well-being. Scopolamine causes this, which contributed to its historical use for premedication in cardiac surgery.
F
Fibreoptic Intubation
Passing a breathing tube using a flexible camera (fibreoptic scope) to guide it - used for difficult airways. Requires a dry airway, hence glycopyrrolate is given beforehand.
G
GABA Receptors
Gamma-aminobutyric acid receptors - the main "calming" receptors in the brain. Benzodiazepines enhance their effect, producing sedation and anxiolysis.
Glycopyrrolate
A synthetic anticholinergic drug. A quaternary amine - does NOT cross the blood-brain barrier. Preferred in modern anaesthesia for antisialagogue effect without CNS side effects. Longer duration than atropine.
GORD (Gastro-Oesophageal Reflux Disease)
A condition where stomach acid repeatedly flows back up the oesophagus. Patients are at higher risk of aspiration under anaesthesia.
H
H2 Blockers (H2 Antagonists)
Drugs that block histamine H2 receptors in the stomach lining, reducing acid secretion. Example: ranitidine. Given preoperatively in aspiration-risk patients to raise gastric pH.
HOCM (Hypertrophic Obstructive Cardiomyopathy)
A condition where the heart muscle is abnormally thickened, obstructing blood flow. Tachycardia (fast heart rate) is dangerous in HOCM - hence atropine must be used with extreme caution.
Hypercapnia
Excess carbon dioxide (CO2) in the blood, usually from inadequate breathing/ventilation. Occurs with oversedation.
Hypoxaemia
Low oxygen levels in the blood. A risk with oversedation depressing breathing.
I
Induction (of Anaesthesia)
The process of bringing a patient from consciousness to a state of general anaesthesia, usually using an intravenous drug or inhalational agent.
Intraoperative
During the surgery/operation.
IV (Intravenous)
Into the vein. Drugs given IV work faster than oral or IM routes.
K
Kinetosis
Motion sickness. Transdermal scopolamine is used for its prevention and treatment.
L
Lorazepam
A benzodiazepine with longer duration than midazolam. Slower onset, particularly unpredictable duration of amnesia. Used when prolonged anxiolysis is needed (e.g. cardiac surgery, 2-4 mg orally 2 hours before).
M
MAC (Minimum Alveolar Concentration)
The concentration of an inhaled anaesthetic needed to prevent movement in 50% of patients in response to a surgical stimulus. Premedication can reduce the MAC required.
Mendelson's Syndrome
Severe lung injury (chemical pneumonitis/pneumonia) caused by aspiration of acidic gastric contents during anaesthesia. Named after Curtis Mendelson who first described it in 1946 in obstetric patients.
Metoclopramide
A prokinetic drug - it accelerates gastric emptying and increases the tone of the lower oesophageal sphincter. Reduces risk of aspiration.
Midazolam
The most commonly used benzodiazepine for premedication. Rapid onset, minimal respiratory depression. Given orally, IV, or intranasally (in children). Short-acting - ideal for day surgery.
Muscarinic Receptors
A type of acetylcholine receptor found in the heart, smooth muscle, glands, and brain. Anticholinergic drugs block these receptors to produce their effects.
Mydriasis
Dilation (widening) of the pupil. A side effect of anticholinergics due to their effect on the iris muscles.
Myocardial Ischaemia
Reduced blood supply to the heart muscle, causing oxygen deprivation. Premedication in cardiac patients aims to prevent this by controlling heart rate and blood pressure.
N
Neuromuscular Blockade / Relaxants
Drugs that paralyse skeletal muscles during surgery by blocking transmission at the neuromuscular junction. They must be reversed at the end of surgery with anticholinesterases.
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
Painkillers like ibuprofen that also reduce inflammation. Can be given before surgery for pre-emptive analgesia but have risks (GI bleeding, renal impairment, altered clotting).
O
Omeprazole
A proton pump inhibitor (PPI). Reduces gastric acid production more potently than H2 blockers. Used for aspiration prophylaxis in high-risk patients.
Opioid
A class of drugs derived from or similar to opium (e.g., morphine, fentanyl). Produce analgesia, sedation, and euphoria. Cause respiratory depression in excess doses.
P
P2Y12 Receptor
A platelet receptor for ADP. Drugs like clopidogrel block this receptor to prevent clotting. Must be stopped before surgery to reduce bleeding risk.
Parasympathetic Nervous System
The "rest and digest" division of the autonomic nervous system. Controls heart slowing, secretions, and gut activity. Acetylcholine is its main neurotransmitter at muscarinic receptors.
Perioperative
The period surrounding surgery - includes before (preoperative), during (intraoperative), and after (postoperative).
Pneumonitis
Inflammation of lung tissue - in the context of anaesthesia, caused by aspirated gastric acid (chemical pneumonitis).
PONV (Post-Operative Nausea and Vomiting)
Nausea and vomiting occurring after surgery and anaesthesia. A common complication. Antiemetic premedication reduces its incidence.
Postoperative
After the surgery/operation.
Preoperative
Before the surgery/operation.
Prokinetic
A drug that speeds up movement of contents through the gastrointestinal tract. Example: metoclopramide. Reduces aspiration risk by emptying the stomach faster.
Proton Pump Inhibitor (PPI)
A type of drug (e.g., omeprazole, lansoprazole) that blocks the proton pump (H+/K+-ATPase) in the stomach lining, strongly reducing gastric acid production.
Pulmonary Aspiration
The accidental inhalation of stomach contents (food, acid) into the lungs during anaesthesia. Potentially life-threatening.
Q
Quaternary Amine
A nitrogen-containing compound carrying a permanent positive charge. Cannot cross cell membranes like the blood-brain barrier or placenta. Glycopyrrolate is a quaternary amine - this is why it lacks CNS effects.
R
Rapid Sequence Induction (RSI)
A technique for quickly inducing anaesthesia and securing the airway in patients at high aspiration risk (e.g. full stomach, emergency surgery). Sodium citrate is typically given just before.
Redistribution
After a single IV dose of an anaesthetic or drug, the plasma level rises and then falls rapidly - not because the drug is metabolised, but because it moves from the blood into other body tissues (fat, muscle). This is why emergence from a single induction dose is quick.
S
Scopolamine (Hyoscine)
A belladonna alkaloid anticholinergic. Tertiary amine - crosses the BBB causing sedation, amnesia, and euphoria. The best antisialagogue of the three. Now mainly used as a transdermal patch for PONV and motion sickness.
Sedation (Conscious Sedation)
A state where a patient is relaxed, drowsy, and comfortable but still conscious and able to respond. Deeper sedation approaches unconsciousness.
Sodium Citrate
A non-particulate (clear) antacid. Given orally immediately before anaesthesia (especially obstetric cases) to rapidly raise gastric pH, reducing the severity of lung injury if aspiration occurs.
Sympathetic Nervous System
The "fight or flight" division of the autonomic nervous system. Causes raised heart rate, raised blood pressure, and other stress responses. Premedication aims to blunt this.
Sympathicolysis
Reduction of sympathetic nervous system activity. One goal of premedication - reduces the stress response to surgery.
Sympatholysis
Same as sympathicolysis - suppression of sympathetic tone.
T
Temazepam
A short-acting oral benzodiazepine used as a premedicant. Commonly used in anxious patients in the UK, particularly for day-case surgery. Given approximately 1 hour before surgery.
Tertiary Amine
A nitrogen-containing organic compound. Uncharged and lipid-soluble - can cross the blood-brain barrier and placenta. Atropine and scopolamine are tertiary amines.
Titration
The practice of giving a drug in small, incremental doses and monitoring the effect, rather than giving a fixed bolus. Reduces the risk of overdose.
V
Vagolysis
Blocking the effects of the vagus nerve (the main parasympathetic nerve to the heart). Prevents vagal bradycardia (dangerously slow heart rate) during surgery. Anticholinergics provide vagolysis.
Vagus Nerve
The 10th cranial nerve. Carries parasympathetic signals to the heart, lungs, and gut. Activation slows the heart.
Vasodilator
A drug that widens blood vessels, lowering blood pressure.
Vasopressor
A drug that constricts blood vessels, raising blood pressure.
W
"White Coat" Hypertension
A temporary rise in blood pressure triggered by the anxiety of being in a medical environment (seeing a doctor or being in hospital). It is not a true chronic hypertension. Anxiolytic premedication can resolve it before surgery.
This glossary covers all major technical terms from the premedication topic. If any specific term needs deeper explanation or a clinical example, just ask.
Translate the main topic in Bengali
জেনারেল অ্যানেস্থেশিয়া - প্রিমেডিকেশন: সম্পূর্ণ বিষয়
সংজ্ঞা ও ঐতিহাসিক পটভূমি
প্রিমেডিকেশন হলো অ্যানেস্থেশিয়ার আগে প্রদত্ত ওষুধ যা অ্যানেস্থেশিয়া শুরু করা ও বজায় রাখা সহজ করে, রোগীর স্বস্তি বাড়ায় এবং নির্দিষ্ট ঝুঁকিগুলো কমায়।
এটি মূলত ১৯শ শতাব্দীতে প্রবর্তিত হয়েছিল - ক্লোরোফর্মের প্রয়োজনীয় মাত্রা কমাতে এবং অস্ত্রোপচারের অ্যানেস্থেশিয়া দ্রুত শুরু করতে। মরফিন ও অ্যান্টিকোলিনার্জিক অ্যাট্রোপিনের সমন্বয় ছিল মূল পদ্ধতি - যা উদ্বেগ কমাতো এবং অ্যানেস্থেশিয়াকে সহজ করতো।
আধুনিক চিকিৎসায়, দ্রুত কার্যকর অ্যানেস্থেটিক এবং ডে-সার্জারির প্রসারের কারণে সেডেটিভ প্রিমেডিকেশন এখন অনেকটাই কম ব্যবহৃত হয়। তবে বেশ কিছু বিভাগ এখনো নিরাপত্তার জন্য গুরুত্বপূর্ণ।
প্রিমেডিকেশনের লক্ষ্যসমূহ
১. অ্যাংজিওলাইসিস - অপারেশনের আগে ভয় ও উদ্বেগ কমানো
২. সেডেশন - অপারেশন থিয়েটারে নিয়ে যাওয়ার আগে রোগীকে শান্ত করা
৩. অ্যামনেশিয়া (অ্যান্টেরোগ্রেড) - অপারেশনের আগের ঘটনাগুলোর স্মৃতি মুছে দেওয়া
৪. ভ্যাগোলাইসিস / সিম্প্যাথিকোলাইসিস - স্বায়ত্তশাসিত স্নায়ুতন্ত্রের প্রতিক্রিয়া কমানো
৫. PONV হ্রাস - অপারেশন-পরবর্তী বমি বমি ভাব ও বমি কমানো
৬. ব্যথানাশক প্রভাব - অপারেশনের আগেই ব্যথা নিয়ন্ত্রণ শুরু করা
৭. অ্যান্টিসায়ালোগ প্রভাব - লালা শুকানো, বিশেষত শ্বাসনালীতে কাজ করার আগে
৮. অ্যাসপিরেশন প্রতিরোধ - ফুসফুসে পাকস্থলীর বিষয়বস্তু ঢোকার ঝুঁকি কমানো
৯. অ্যানেস্থেটিকের প্রয়োজনীয় মাত্রা কমানো (MAC কমানো)
১০. সিম্প্যাথেটিক উদ্দীপনা কমানো - হৃদরোগ ও উচ্চ রক্তচাপের রোগীদের জন্য বিশেষ গুরুত্বপূর্ণ
প্রিমেডিকেশন ওষুধের শ্রেণীবিভাগ
১. বেনজোডায়াজেপিন (সবচেয়ে বেশি ব্যবহৃত)
বেনজোডায়াজেপিন হলো প্রিমেডিকেশনে সবচেয়ে বেশি ব্যবহৃত ওষুধ। এগুলো উদ্বেগ কমায়, ঘুম আনে, স্মৃতিভ্রংশ ঘটায় এবং PONV কমায়। স্মৃতিভ্রংশ শুধুমাত্র অ্যান্টেরোগ্রেড - পুরনো স্মৃতি নষ্ট হয় না।
প্রধান ওষুধ ও মাত্রা
| ওষুধ | মুখে খাওয়ার মাত্রা (বড়দের) | বিশেষ তথ্য |
|---|---|---|
| মিডাজোলাম | ৭.৫-১৫ মি.গ্রা. | বড় ও ছোট উভয়ের জন্য সবচেয়ে বেশি ব্যবহৃত; দ্রুত কার্যকর; শ্বাসক্রিয়ায় সামান্য প্রভাব |
| ডায়াজেপাম | ৫-১০ মি.গ্রা. | দীর্ঘস্থায়ী; অপারেশনের আগের রাতের ঘুমের জন্য উপযোগী |
| টেমাজেপাম | ১০-২০ মি.গ্রা. | স্বল্পমেয়াদী; ডে-সার্জারিতে বেশি ব্যবহৃত |
| লোরাজেপাম | ২-৪ মি.গ্রা. মুখে, অপারেশনের ২ ঘণ্টা আগে | দীর্ঘ ও তীব্র উদ্বেগনাশক প্রয়োজন হলে ব্যবহার (যেমন: হৃদ অস্ত্রোপচার) |
মিডাজোলাম বড় ও ছোট উভয় রোগীর ক্ষেত্রেই প্রিমেডিকেশনে সবচেয়ে বেশি ব্যবহৃত বেনজোডায়াজেপিন। সর্বোচ্চ ২০ মি.গ্রা. পর্যন্ত শ্বাসক্রিয়া ও অক্সিজেনে তেমন প্রভাব ফেলে না।
শিশুদের ক্ষেত্রে: মিডাজোলাম ০.০২৫ মি.গ্রা./কেজি মাত্রায় ১০-২০ মিনিটের মধ্যে ঘুম ও উদ্বেগ কমায়। মুখে খাওয়া, নাকে দেওয়া এবং শিরাপথে - তিনটি উপায়েই দেওয়া যায়।
তুলনামূলক বৈশিষ্ট্য:
- মিডাজোলাম ও ডায়াজেপাম: একইরকম দ্রুত পুনরুদ্ধার (রিডিস্ট্রিবিউশনের কারণে)
- লোরাজেপাম: ধীর শুরু, দীর্ঘ ও অনিশ্চিত স্মৃতিভ্রংশ - যারা অপারেশন-পরবর্তীতে মনে রাখতে চান তাদের জন্য অনুপযুক্ত
নিরাপত্তা: ৮০ বছর বা তার বেশি বয়সী রোগীদের সহ সকল বয়সেই বেনজোডায়াজেপিন প্রিমেডিকেশন নিরাপদ এবং মৃত্যুহার বাড়ায় না।
২. অ্যান্টিকোলিনার্জিক (অ্যান্টিমাস্কারিনিক) ওষুধ
তিনটি প্রধান ওষুধ: অ্যাট্রোপিন, স্কোপোলামিন (হায়োসিন), এবং গ্লাইকোপাইরোলেট।
কার্যপদ্ধতি
প্যারাসিম্প্যাথেটিক মাস্কারিনিক রিসেপ্টরে অ্যাসিটাইলকোলিনের প্রতিযোগিতামূলক বাধাদানকারী। এদের কাজ:
- লালা, ব্রংকাস, অগ্ন্যাশয় ও পরিপাকতন্ত্রের নিঃসরণ কমানো (অ্যান্টিসায়ালোগ)
- হৃদস্পন্দন বাড়ানো
- ব্রংকোডায়ালেশন
- পরিপাকতন্ত্রের গতি কমানো
- পাকস্থলীর অ্যাসিড উৎপাদন কমানো
- পেশি শিথিলকারক ওষুধ ফেরানোর সময় পার্শ্বপ্রতিক্রিয়া রোধ করা
তুলনামূলক সারণি
| বৈশিষ্ট্য | অ্যাট্রোপিন | স্কোপোলামিন | গ্লাইকোপাইরোলেট |
|---|---|---|---|
| ওষুধের ধরন | তৃতীয় অ্যামিন (বেলাডোনা) | তৃতীয় অ্যামিন (বেলাডোনা) | চতুর্থ অ্যামিন (কৃত্রিম) |
| রক্ত-মস্তিষ্ক বাধা অতিক্রম করে? | হ্যাঁ | হ্যাঁ | না |
| গর্ভফুল অতিক্রম করে? | হ্যাঁ | হ্যাঁ | না |
| শিরাপথে কার্যকাল | ১৫-৩০ মিনিট | ৩০-৬০ মিনিট | ২-৪ ঘণ্টা |
| মাংসপেশিতে কার্যকাল | ২-৪ ঘণ্টা | ৪-৬ ঘণ্টা | ৬-৮ ঘণ্টা |
| কেন্দ্রীয় স্নায়ুতন্ত্রে প্রভাব | হালকা উদ্দীপনা (কম মাত্রায়); প্রলাপ (বেশি মাত্রায়) | ঘুম, স্মৃতিভ্রংশ, আনন্দানুভূতি | কোনো প্রভাব নেই |
| অ্যান্টিসায়ালোগ প্রভাব | + | +++ | ++ |
| হৃদস্পন্দন বৃদ্ধি | +++ | + (মাংসপেশিতে সামান্য) | + |
গুরুত্বপূর্ণ তথ্য:
- স্কোপোলামিন এখন মূলত মোশন সিকনেস ও PONV প্রতিরোধে ত্বকে লাগানো প্যাচ হিসেবে ব্যবহৃত হয়।
- গ্লাইকোপাইরোলেট এখন অ্যানেস্থেশিয়ায় পছন্দের ওষুধ কারণ: (১) রক্ত-মস্তিষ্ক বাধা অতিক্রম করে না, (২) বেশিক্ষণ কার্যকর, (৩) অ্যান্টিসায়ালোগ প্রভাব বেশি। ফাইবারঅপটিক ইন্টুবেশনের আগে বিশেষভাবে গুরুত্বপূর্ণ।
- অ্যাট্রোপিন: ব্র্যাডিকার্ডিয়া চিকিৎসায় পছন্দের ওষুধ; তবে যখন দ্রুত হৃদস্পন্দন ক্ষতিকর (করোনারি আর্টারি স্টেনোসিস, HOCM, অ্যাওর্টিক স্টেনোসিস, ফিওক্রোমোসাইটোমা) তখন সতর্কতার সাথে ব্যবহার করতে হবে।
- বৃদ্ধদের ক্ষেত্রে: কেন্দ্রীয়ভাবে সক্রিয় অ্যান্টিকোলিনার্জিক (অ্যাট্রোপিন, স্কোপোলামিন) অপারেশন-পরবর্তী মানসিক বিভ্রান্তি তৈরি করতে পারে - গ্লাইকোপাইরোলেট পছন্দনীয়।
- বিশেষ তথ্য: অ্যাট্রোপিনের অতি কম মাত্রা (<০.১ মি.গ্রা.) প্রাক-সিন্যাপটিক M1 রিসেপ্টর ব্লক করে বিপরীতভাবে হৃদস্পন্দন কমিয়ে দিতে পারে।
৩. ওপিওয়েড (মাদকজাতীয় ব্যথানাশক)
মরফিন ও এর জাতীয় ওষুধ মূল প্রিমেডিকেশনের অংশ ছিল। আধুনিক চিকিৎসায় নির্দিষ্ট ক্ষেত্রে ব্যবহৃত হয়:
- হৃদ অস্ত্রোপচারের রোগী: অপারেশনের আগে উদ্বেগ ও ব্যথা কমাতে; সাধারণত ফেন্টানাইল IV মিডাজোলামের সাথে ক্যাথেটার বসানোর আগে
- ব্যথাযুক্ত রোগী যাদের আগে থেকেই ব্যথানাশক প্রয়োজন
- ইন্টুবেশনের সময় হেমোডাইনামিক প্রতিক্রিয়া কমাতে
সতর্কতা: হার্ট ফেইলিউরে কম কার্ডিয়াক আউটপুট বা পালমোনারি হাইপারটেনশনের রোগীতে ওপিওয়েড সেডেশন সতর্কতার সাথে দিতে হবে - অতিরিক্ত সেডেশনে হার্ট দুর্বল হয়ে যেতে পারে, শ্বাসক্রিয়া বন্ধ হয়ে অক্সিজেন কমতে পারে।
৪. অ্যাসপিরেশন প্রতিরোধকারী ওষুধ
পাকস্থলীর বিষয়বস্তু ফুসফুসে ঢুকলে মারাত্মক মেন্ডেলসন সিনড্রোম (কেমিক্যাল নিউমোনাইটিস) হতে পারে। বেশি ঝুঁকিতে থাকা রোগী:
- ডায়াবেটিস মেলিটাস
- কিডনির সমস্যা
- স্থূলতা
- গ্যাস্ট্রো-ইসোফেজিয়াল রিফ্লাক্স ডিজিজ (GORD)
- গর্ভাবস্থা
- ভরা পেটে / জরুরি অস্ত্রোপচার
ব্যবহৃত ওষুধ:
| ওষুধের ধরন | উদাহরণ | কাজ |
|---|---|---|
| H2 ব্লকার | র্যানিটিডিন | পাকস্থলীর অ্যাসিড উৎপাদন কমায় |
| প্রোটন পাম্প ইনহিবিটর | ওমেপ্রাজোল | H2 ব্লকারের চেয়ে বেশি শক্তিশালীভাবে অ্যাসিড কমায় |
| গ্যাস্ট্রিক অ্যালকালাইজার | সোডিয়াম সাইট্রেট (০.৩M) | পাকস্থলীর pH দ্রুত বাড়ায়; র্যাপিড সিকোয়েন্স ইন্ডাকশনের আগে ব্যবহৃত |
| প্রোকিনেটিক | মেটোক্লোপ্রামাইড | পাকস্থলী দ্রুত খালি করে; নিচের খাদ্যনালীর স্বরবন্ধনী শক্ত করে |
উচ্চ ঝুঁকির রোগীতে (যেমন প্রসূতি রোগী - সিজারিয়ান সেকশন) প্রায়ই এই তিনটির সমন্বয় ব্যবহার করা হয়।
৫. ব্যথানাশক ওষুধ (প্রি-এম্পটিভ অ্যানালজেসিয়া)
অপারেশনের আগে মুখে প্যারাসিটামল ও NSAIDs দেওয়া যায়। এগুলো পাকস্থলী থেকে ভালোভাবে শোষিত হয় এবং সাশ্রয়ী।
প্রমাণ সংক্রান্ত তথ্য: অপারেশনের পরে দেওয়া একই ব্যথানাশকের চেয়ে আগে দিলে বেশি উপকার হয় - এর প্রমাণ দুর্বল, তবে ব্যাপকভাবে ব্যবহৃত হয়।
NSAIDs-এ সতর্কতা:
- বৃদ্ধ রোগী
- পেটের সমস্যাযুক্ত রোগী
- কিডনির সমস্যা
- কিছু অস্ত্রোপচারে রক্ত জমাট বাঁধার সমস্যা তৈরি করতে পারে
৬. অ্যান্টিইমেটিক (বমি প্রতিরোধকারী)
বেশি PONV ঝুঁকির রোগীতে অ্যান্টিইমেটিক প্রিমেডিকেশন দেওয়া হয়। ত্বকে লাগানো স্কোপোলামিন প্যাচ, অনডানসেট্রন এবং ডেক্সামেথাসোন ব্যবহার করা হয়।
৭. নিয়মিত ওষুধ চালিয়ে যাওয়া
একটি মূলনীতি হলো - রোগীরা সাধারণত অপারেশনের দিনেও তাদের নিয়মিত ওষুধ চালিয়ে যাবেন, তবে কিছু ব্যতিক্রম আছে:
| ওষুধ | অপারেশনকালীন নির্দেশনা |
|---|---|
| বিটা-ব্লকার | চালিয়ে যান - হঠাৎ বন্ধ করলে বিপজ্জনক রিবাউন্ড ইস্কেমিয়া/টাকিকার্ডিয়া হতে পারে |
| স্ট্যাটিন | চালিয়ে যান - অপারেশনকালীন উপকার আছে |
| ACE ইনহিবিটর | সতর্কতা - অপারেশনের দিন দিলে অপারেশনের সময় রক্তচাপ বিপজ্জনকভাবে কমে যেতে পারে |
| অ্যাসপিরিন | পরিকল্পিত অস্ত্রোপচারে: রক্তক্ষরণ কমাতে আগে বন্ধ করুন; তীব্র করোনারি সিনড্রোমে চালিয়ে যান |
| P2Y12 ইনহিবিটর (যেমন ক্লোপিডোগ্রেল) | করোনারি অপারেশনের আগে বন্ধ করুন; ফার্মাকোডায়নামিক্স অনুযায়ী সময় নির্ধারণ (অপরিবর্তনীয় ইনহিবিটরের জন্য কমপক্ষে ৩ দিন) |
| অ্যান্টিএনজাইনাল / নাইট্রেট | বিটা-ব্লকার চালিয়ে যান; প্রফিল্যাক্টিক IV নাইট্রেট চলমান ইস্কেমিয়া ছাড়া কোনো উপকার করে না |
বিশেষ রোগীর ক্ষেত্রে
হৃদ অস্ত্রোপচারের রোগী
- অপারেশন থিয়েটারে নিয়ে যাওয়ার আগে ওপিওয়েড ± অ্যাংজিওলাইটিক দেওয়া প্রয়োজন
- অ্যানেস্থেশিয়া শুরুর আগে রেডিয়াল আর্টারি ক্যানুলেশনের সময় সাধারণত IV মিডাজোলাম ± ফেন্টানাইল দেওয়া হয়
- হার্ট ফেইলিউরে অতিরিক্ত সেডেশন অবশ্যই এড়াতে হবে - হার্ট আরও দুর্বল হয়ে রক্তচাপ কমে যেতে পারে
- পালমোনারি হাইপারটেনশনে: অতিরিক্ত সেডেশনে শ্বাসক্রিয়া বন্ধ হয়ে CO2 বাড়তে পারে
উচ্চ রক্তচাপের রোগী
- অ্যাংজিওলাইটিক প্রিমেডিকেশন (যেমন মিডাজোলাম) "হোয়াইট কোট হাইপারটেনশন" ঠিক করে দিতে পারে
করোনারি আর্টারি ডিজিজের রোগী
- প্রিমেডিকেশনের লক্ষ্য: সিম্প্যাথেটিক উদ্দীপনা কমানো (হৃদপেশিতে অক্সিজেনের চাহিদা-সরবরাহের ভারসাম্য রক্ষা)
- অপারেশনের আগে শুধুমাত্র অল্প মাত্রায় IV মিডাজোলাম (প্রয়োজনে ছোট মাত্রায় ওপিওয়েড) দিন
- অতিরিক্ত সেডেশনও সমানভাবে ক্ষতিকর - অক্সিজেন কমে, CO2 বাড়ে, রক্তচাপ কমে
বৃদ্ধ রোগী
- কেন্দ্রীয়ভাবে সক্রিয় অ্যান্টিকোলিনার্জিক এড়িয়ে চলুন (অপারেশন-পরবর্তী মানসিক বিভ্রান্তির ঝুঁকি)
- অ্যান্টিকোলিনার্জিক প্রয়োজন হলে গ্লাইকোপাইরোলেট ব্যবহার করুন
- NSAIDs-এ সতর্কতা (কিডনির কার্যক্ষমতা ও পাকস্থলীর ঝুঁকি)
শিশু রোগী
- মুখে বা নাকে মিডাজোলাম ব্যাপকভাবে ব্যবহৃত
- অপারেশনের সময় বাবা-মায়ের উপস্থিতি শিশুর উদ্বেগ কমাতে পারে এবং অনেক ক্ষেত্রে ওষুধের বিকল্প হতে পারে
আধুনিক প্রবণতা ও ব্যবহারিক বিষয়
১. সেডেটিভ প্রিমেডিকেশন এখন আধুনিক অ্যানেস্থেশিয়ায় কম ব্যবহৃত হয় - বিশেষত ডে-সার্জারির বিস্তারের সাথে
২. অ্যান্টিইমেটিক ও অ্যান্টাসিড প্রফিল্যাক্সিস উচ্চ-ঝুঁকির রোগীতে এখনো গুরুত্বপূর্ণ
৩. মরফিন-অ্যাট্রোপিনের মূল সমন্বয় এখনো কঠিন/ফাইবারঅপটিক ইন্টুবেশনের আগে মাঝেমধ্যে ব্যবহৃত হয়
৪. রোগীকে পরিষ্কারভাবে অপারেশনের পদ্ধতি বুঝিয়ে বলা উদ্বেগ কমানোর প্রথম পদক্ষেপ - ওষুধের প্রয়োজন কমায়
৫. অপারেশনের আগে মুখে সহজ ব্যথানাশক দেওয়া সাশ্রয়ী, প্রি-এম্পটিভ উপকারের প্রমাণ দুর্বল হলেও
সারসংক্ষেপ সারণি
| ওষুধের শ্রেণী | প্রধান লক্ষ্য | মূল ওষুধ | পথ | সময় |
|---|---|---|---|---|
| বেনজোডায়াজেপিন | উদ্বেগনাশ, স্মৃতিভ্রংশ, সেডেশন | মিডাজোলাম, টেমাজেপাম, লোরাজেপাম | মুখে, শিরায় | অপারেশনের ৩০-৬০ মিনিট আগে |
| অ্যান্টিকোলিনার্জিক | অ্যান্টিসায়ালোগ, ভ্যাগোলাইসিস | গ্লাইকোপাইরোলেট, অ্যাট্রোপিন, স্কোপোলামিন | মাংসপেশিতে, শিরায় | ৩০-৬০ মিনিট আগে |
| ওপিওয়েড | ব্যথানাশ, সেডেশন | মরফিন, ফেন্টানাইল | মাংসপেশিতে, শিরায় | পরিস্থিতি অনুযায়ী |
| অ্যান্টাসিড / H2 / PPI | অ্যাসপিরেশন প্রতিরোধ | সোডিয়াম সাইট্রেট, র্যানিটিডিন, ওমেপ্রাজোল, মেটোক্লোপ্রামাইড | মুখে | ১-২ ঘণ্টা আগে |
| ব্যথানাশক | প্রি-এম্পটিভ ব্যথানাশ | প্যারাসিটামল, NSAIDs | মুখে | ১ ঘণ্টা আগে |
| অ্যান্টিইমেটিক | PONV প্রতিরোধ | স্কোপোলামিন (ত্বকে), অনডানসেট্রন | ত্বকে, শিরায় | অপারেশনের আগের রাতে / ১ ঘণ্টা আগে |
সূত্র: Miller's Anesthesia 10e | Morgan and Mikhail's Clinical Anesthesiology 7e | Barash, Cullen and Stoelting's Clinical Anesthesia 9e | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 | Bailey and Love's Short Practice of Surgery 28e
This is a shared conversation. Sign in to Orris to start your own chat.