Pyriform fossa growth in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
"pyriform sinus" OR "pyriform fossa" carcinoma treatment
Finding Sources
Searching PubMed
"pyriform sinus carcinoma" OR "hypopharyngeal carcinoma" treatment outcomes
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
GROWTH OF THE PYRIFORM FOSSA (PYRIFORM SINUS CARCINOMA)
RGUHS 50-Mark Model Answer
INTRODUCTION
Carcinoma of the pyriform fossa (pyriform sinus) is the most common malignancy of the hypopharynx, accounting for approximately 65-75% of all hypopharyngeal cancers. It carries a poor prognosis due to late presentation, rich lymphatic drainage, proximity to the larynx, and a high rate of locoregional and distant metastases. Understanding its anatomy, pathology, clinical features, staging, and treatment is essential for ENT practice.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 317
- K.J. Lee's Essential Otolaryngology, p. 667
DIAGRAM 1: ANATOMY OF THE HYPOPHARYNX AND PYRIFORM FOSSA
CROSS-SECTION VIEW OF HYPOPHARYNX
(Axial plane at the level of the pyriform sinus)
ANTERIOR
|
[Thyroid cartilage]
/ \
Lateral wall Lateral wall
(Pyriform sinus) (Pyriform sinus)
| |
[Thyro-hyoid membrane] [Thyro-hyoid membrane]
\ /
[Medial wall]
(Aryepiglottic fold)
|
[Paraglottic space]
|
[Cricoid cartilage]
|
POSTERIOR
SAGITTAL/LATERAL BOUNDARY DIAGRAM OF PYRIFORM SINUS:
SUPERIOR LIMIT: Pharyngoepiglottic fold (level of hyoid)
INFERIOR LIMIT: Pyriform apex (level of cricoid cartilage)
LATERAL WALL: Contiguous with thyroid cartilage & thyrohyoid membrane
MEDIAL WALL: Aryepiglottic fold → postcricoid mucosa
POSTERIOR WALL: Opens posteriorly into pharyngeal lumen
Shape: FUNNEL-SHAPED channel bilaterally alongside the larynx
Key anatomical relationships:
| Structure | Relationship |
|---|---|
| Thyroid cartilage | Lateral to pyriform sinus - invaded by lateral wall tumours |
| Thyrohyoid membrane | Allows extralaryngeal spread without cartilage destruction |
| Aryepiglottic fold | Forms medial wall |
| Paraglottic space | Tumours at apex spread superiorly here, causing cord fixity |
| Cricoid cartilage | Medial and inferior to apex - apex tumours mandate cricoid removal |
| Cricothyroid membrane | Route of early escape of apex tumours |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, pp. 317-318
HISTOLOGY AND WALL LAYERS
The wall of the hypopharynx consists of four layers:
- Lining - non-keratinized stratified squamous epithelium
- Pharyngobasilar fascia
- Muscular layer - lower fibres of middle constrictor + inferior constrictor
- Buccopharyngeal fascia
Histological type: >95% Squamous Cell Carcinoma (SCC). May be keratinizing or non-keratinizing. Rare variants: adenocarcinoma, sarcoma, lymphoma.
AETIOLOGY AND RISK FACTORS
Primary Risk Factors:
- Tobacco smoking - current smokers have 8.53x higher incidence vs. never-smokers; dose-response relationship; bidi smoking: OR 6.8 for hypopharyngeal cancer
- Alcohol - heavy drinkers (>4 drinks/day): relative risk 9.03; synergistic effect with tobacco; acts as solvent for carcinogens and increases mucosal permeability
Other Risk Factors:
-
HPV - seen in 10.9% of hypopharyngeal cancers; pyriform fossa has the highest HPV association within hypopharynx
-
Nutritional deficiency - low BMI (≤18.5) particularly in smokers; deficiency of vitamins and dietary fibre
-
Occupational exposure - construction workers, potters, butchers, barbers; coal dust, steel dust, iron compounds, formalin fumes
-
Paterson-Brown-Kelly / Plummer-Vinson Syndrome - sideropenic dysphagia (more relevant to postcricoid carcinoma)
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 318
MOLECULAR BASIS
Hypopharyngeal cancers show:
-
Amplification of oncogenes CCND1, FGF3, FGF4 (region 11q12)
-
TP53 mutations (most common head and neck alteration)
-
EGFR overexpression - relevant for targeted therapy (cetuximab)
-
HPV-positive tumors: better prognosis vs. HPV-negative
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 318
CLINICAL FEATURES
Symptoms (in order of frequency):
- Dysphagia (most common presenting symptom) - initially to solids, then progressive
- Odynophagia - pain on swallowing
- Referred otalgia (via Arnold's nerve / Jacobson's nerve - CN X & IX) - a hallmark
- Hoarseness - due to involvement of the recurrent laryngeal nerve or paraglottic space
- Neck lump - enlarged cervical lymph nodes (often the presenting complaint, ~20-30%)
- Weight loss, anorexia
- Blood-stained sputum/hemoptysis
- Stridor - late sign, airway compromise
Signs:
- Pooling of saliva in pyriform fossa on laryngoscopy (pathognomonic)
- Mucosal irregularity/ulceration on laryngoscopy
- Fixed or reduced vocal cord mobility
- Palpable neck nodes (levels II, III, IV)
PATTERNS OF SPREAD
DIAGRAM 2: LOCAL SPREAD FROM PYRIFORM SINUS
PYRIFORM SINUS TUMOUR
|
┌──────────┼──────────────┐
│ │ │
MEDIAL WALL LATERAL WALL APEX TUMOUR
│ │ │
↓ ↓ ↓
Aryepiglottic Thyroid cart. Paraglottic space
fold involved invasion (→ vocal cord fixity)
│ │ │
Paraglottic Extralaryngeal Cricoid involvement
space spread via (precludes conservation
thyrohyoid surgery)
membrane │
Cricothyroid membrane
(early extralaryngeal escape)
Local Extension (Scott-Brown, p. 319):
- Lateral wall tumours - invade thyroid cartilage (ossified cartilages more prone); may spread extralaryngeally via thyrohyoid membrane
- Medial wall tumours - extend anteromedially into paraglottic space causing vocal cord fixity
- Apex tumours - invade paraglottic space superiorly + cricoid cartilage medially; escape via cricothyroid membrane; conservation surgery not feasible
LYMPHATIC DRAINAGE
DIAGRAM 3: Lymphatic Drainage of the Hypopharynx
(From Scott-Brown's Otorhinolaryngology, Fig. 16.1):
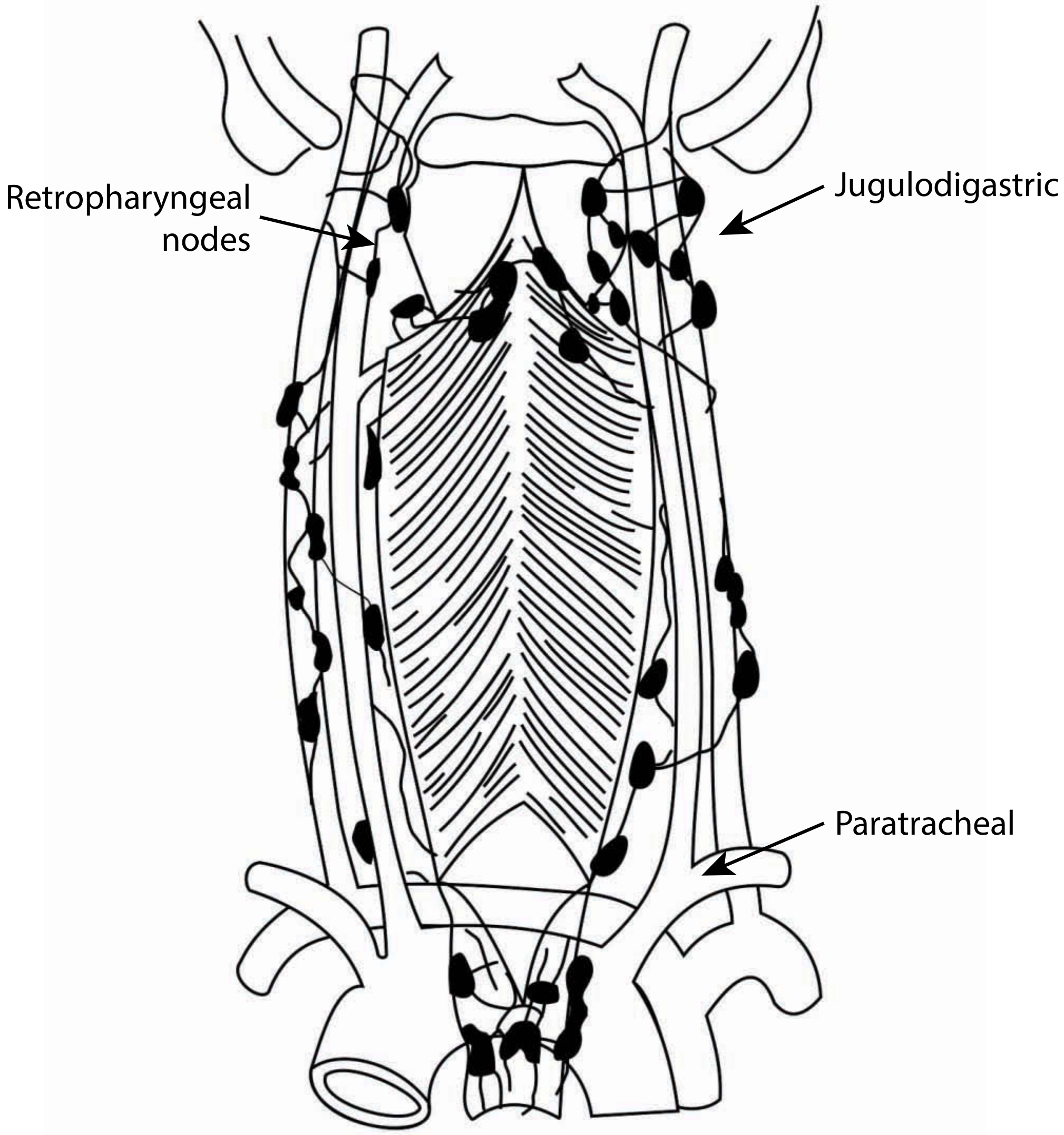
Summary:
| Subsite | Primary nodal drainage |
|---|---|
| Pyriform sinus (upper) | Deep cervical chain - jugulodigastric + jugulo-omohyoid (Levels II, III) |
| Pyriform apex + postcricoid | Paratracheal nodes (Level VI) |
| Posterior pharyngeal wall | Retropharyngeal nodes |
| All sites | Bilateral in advanced disease; N0 neck has 30-40% occult metastases |
Nodal disease is present in 60-75% of patients at diagnosis. Contralateral and bilateral nodal spread is common due to rich anastomotic lymphatic network.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 318
INVESTIGATIONS
FLOWCHART 1: Investigative Workup
SUSPECTED PYRIFORM SINUS CARCINOMA
│
┌─────────┴─────────┐
│ │
CLINICAL IMAGING
│ │
Indirect/Flexible CE-CT Neck & Chest
Laryngoscopy (First-line)
(pooling of saliva, │
mucosal lesion, ├── MRI - if cartilage
cord mobility) │ invasion suspected
│ │ (sensitivity 96%)
│ │
├── Direct ├── FDG PET-CT:
│ Laryngoscopy │ - Borderline resectable
│ + BIOPSY │ - Post-radiation
│ under GA │ - Occult disease
│
├── Flexible transnasal
│ oesophagoscopy
│ (map lower limit,
│ synchronous lesions)
│
├── FNAC of neck nodes
│ (NO open biopsy)
│
└── Chest X-ray / CT chest
(distant metastases)
│
HPV testing (p16 IHC)
Liver function tests
Haematological workup
Endoscopy checklist (Table 16.1, Scott-Brown):
- Pyriform apex: free or involved? (determines conservation surgery feasibility)
- Cricoarytenoid joint mobility
- Cricopharyngeal involvement (indicates need for reconstruction)
- Vocal cord mobility (mobile vs. fixed)
CT findings: Asymmetric soft tissue thickening, obliteration of pyriform fat, cartilage erosion.
CT image showing right hypopharyngeal cancer with thyroid invasion:

- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, pp. 319-321
TNM STAGING (AJCC 8th Edition)
Primary Tumour (T):
| T Stage | Description |
|---|---|
| T1 | Tumour limited to ONE subsite of hypopharynx AND ≤2 cm in greatest dimension |
| T2 | Invades >1 subsite OR adjacent site, OR >2 cm but ≤4 cm, WITHOUT hemilarynx fixation |
| T3 | >4 cm OR fixation of hemilarynx OR extension to oesophagus |
| T4a | Moderately advanced: invades thyroid/cricoid cartilage, hyoid bone, thyroid gland, or central compartment soft tissue |
| T4b | Very advanced: invades prevertebral fascia, encases carotid artery, or involves mediastinal structures |
Regional Lymph Nodes (N):
| N Stage | Description |
|---|---|
| N0 | No regional nodal metastasis |
| N1 | Single ipsilateral node ≤3 cm, no extranodal extension (ENE) |
| N2a | Single ipsilateral node >3-6 cm, no ENE |
| N2b | Multiple ipsilateral nodes, none >6 cm, no ENE |
| N2c | Bilateral or contralateral nodes, none >6 cm, no ENE |
| N3a | Any node >6 cm, no ENE |
| N3b | Any node with clinical ENE |
Stage Grouping:
| Stage | T | N | M |
|---|---|---|---|
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0; T1-T3 |
| IVA | T1-T3 N2 M0; T4a N0-N2 M0 | ||
| IVB | T4b any N; Any T N3 | ||
| IVC | Any T, Any N, M1 |
Note (AJCC 8th edition change): T4a = "moderately advanced"; T4b = "very advanced" (renamed from resectable/unresectable)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 321
TREATMENT
FLOWCHART 2: Management Algorithm for Pyriform Sinus Carcinoma
PYRIFORM SINUS CARCINOMA
CONFIRMED (biopsy + imaging)
│
┌─────────┴──────────┐
│ │
EARLY DISEASE ADVANCED DISEASE
(T1-T2 N0-N1) (T3-T4 / N2-N3)
│ │
├── TRANSORAL ├── Operable?
│ APPROACHES │
│ - TLM ├─YES── OPEN SURGERY
│ - TORS │ + POST-OP CHEMORADIATION
│ │ │
├── RADIOTHERAPY │ ┌───┴───────────────────┐
│ (definitive, │ │ │
│ T1-T2) │ CONSERVATION TOTAL
│ │ SURGERY LARYNGOPHARYNGECTOMY
└── NECK: │ (Partial + RECONSTRUCTION
- N0: Elective │ Laryngopharyngectomy) │
bilateral │ - If apex free ├─Pectoralis major
irradiation │ - Cords mobile ├─Free jejunum
- N+: ND │ └─Gastric pull-up
+ adjuvant RT │
├─NO── ORGAN PRESERVATION
│ PROTOCOLS
│ │
│ ┌──┴─────────────────┐
│ │ │
│ Induction Definitive
│ chemotherapy Concurrent
│ (EORTC protocol) Chemoradiation
│ │ (Cisplatin-based)
│ ↓
│ RESPONSE?
│ ├─YES── RT + concurrent chemo
│ └─NO─── Surgery
1. TRANSORAL LASER MICROSURGERY (TLM)
- Best for T1-T2 and selected T3 pyriform sinus cancers
- CO2 laser via microsuspension laryngoscopy
- Oncological outcomes: local control 84% T1, 70% T2, 75% T3, 57% T4a
- 5-year recurrence-free survival: 73% stage I/II, 59% stage III, 47% stage IVa
- Functional advantage: most patients on oral feeds from day 1 if arytenoid preserved
- Aspiration pneumonia <12%; tracheostomy required in 5%
- Scott-Brown's Otorhinolaryngology, p. 325
2. TRANSORAL ROBOTIC SURGERY (TORS)
- Increasing role in T1-T2 hypopharyngeal cancer
- 3D visualization, wristed instruments, reduced morbidity vs. open surgery
- Systematic review (PMID 35464886) - comparable oncological outcomes to TLM; better functional preservation than open surgery
3. OPEN SURGICAL APPROACHES
A. Partial Laryngopharyngectomy (Conservation surgery)
- For lateral wall pyriform sinus cancers with mobile cords and free apex
- Removes ipsilateral pyriform sinus + part of larynx
- Contraindications: apex involvement, cord fixity, bilateral disease, poor pulmonary reserve
- Functional results: oral feeding achieved in 86.2%, decannulated in 88% within 44 days
- 5-year OS: 78%, disease-specific survival 77.6% (Chung et al.)
B. Total Laryngopharyngectomy
- T3-T4 with cord fixity, bilateral disease, apex involvement
- Reconstruction options:
- Pectoralis major myocutaneous flap (partial pharyngeal defects)
- Free radial forearm flap
- Free jejunal autograft (circumferential defects)
- Gastric pull-up (when cervical oesophagus also involved)
4. RADIOTHERAPY
- Definitive RT: for T1-T2 or unfit patients
- Adjuvant RT: post-operative in all T3-T4 or node-positive disease
- Standard dose: 60-66 Gy in 30-33 fractions
- IMRT (Intensity-Modulated Radiotherapy) preferred to reduce dose to salivary glands and spinal cord
5. ORGAN PRESERVATION PROTOCOLS
- EORTC Landmark Trial (Lefebvre 1996): Induction cisplatin + 5-FU x3 cycles; responders receive RT alone; non-responders proceed to surgery. Demonstrated larynx preservation in 42% at 5 years with no compromise in OS.
- Concurrent Chemoradiation (CCRT): Cisplatin 100 mg/m² every 3 weeks + standard RT - now the preferred organ-preservation approach for T3-T4 disease
- Cummings Otolaryngology Head and Neck Surgery (EORTC trial references)
6. NECK MANAGEMENT
- N0 neck: Elective bilateral neck irradiation (or selective neck dissection levels II-IV)
- N+ neck: Modified radical or selective neck dissection + adjuvant RT/CRT
- Bilateral treatment often required due to risk of contralateral metastasis
OUTCOMES (K.J. Lee's Essential Otolaryngology, p. 858)
| Subsite | Local/Regional Control | 5-Year Overall Survival |
|---|---|---|
| Pyriform sinus | 58-71% | 20-50% |
| Pharyngeal wall | T1: 91%, T2: 73%, T3: 61%, T4: 37% | ~21% |
| Postcricoid | <60% | ~35% |
- Distant metastases occur in ~20% of patients, more common with two or three wall involvement
- Poor prognostic factors: apex involvement, close margins (<5mm), N3b disease, advanced nodal stage
FLOWCHART 3: Reconstruction Algorithm After Surgery
PHARYNGEAL DEFECT AFTER
LARYNGOPHARYNGECTOMY
│
┌─────┴──────┐
│ │
PARTIAL CIRCUMFERENTIAL
DEFECT DEFECT
│ │
│ ┌─────┴──────────┐
│ │ │
│ WITHOUT WITH
│ OESOPHAGECTOMY OESOPHAGECTOMY
│ │ │
│ Free jejunum Gastric pull-up
│ Tubed RFFF
│ Tubed ALT flap
│
├── Small defect: Primary closure
├── Medium: PMMC flap
└── Large: Free RFFF or ALT flap
RFFF = Radial forearm free flap
ALT = Anterolateral thigh flap
PMMC = Pectoralis major myocutaneous flap
RECENT ADVANCES (2021-2026)
1. Transoral Robotic Surgery (TORS)
- Lai et al. (2022), Systematic Review, PMID 35464886 - TORS achieves comparable oncological outcomes to open surgery with better functional results and shorter hospital stay for T1-T2 hypopharyngeal cancers. Endoscopic laryngopharyngeal surgery (ELPS) is an emerging alternative.
2. Immunotherapy / Checkpoint Inhibitors
- PD-1/PD-L1 inhibitors (pembrolizumab, nivolumab) - approved for recurrent/metastatic H&N SCC; emerging role in locally advanced disease
- Camrelizumab (PD-1 inhibitor) + induction chemoimmunotherapy - Phase II trial (PMID 38898018): promising response rates in locally advanced hypopharyngeal carcinoma; 2-year OS improved; may allow organ preservation in otherwise unresectable cases
- FDA-approved: pembrolizumab for PD-L1 positive recurrent/metastatic HNSCC (KEYNOTE-048)
3. Induction Chemoimmunotherapy
- Replacing traditional TPF (taxane-platinum-5FU) induction with PD-1 inhibitor combinations; higher complete response rates, paving the way for organ preservation approaches
4. Transoral Laser Surgery for Early Disease
- Casanueva et al. (2023), PMID 36056169 - Confirms TLM offers excellent oncological and functional outcomes for T1-T2 disease with 5-year OS of 60-71%.
5. Response-Adapted Treatment
- Luo et al. (2022), JAMA Network Open, PMID 35191967 - Response-adapted treatment following radiotherapy in locally advanced hypopharyngeal carcinoma; patients with good response can avoid surgery, preserving organ function without compromising survival.
6. Molecular Targeted Therapy
- Cetuximab (anti-EGFR monoclonal antibody) - used with RT in cisplatin-ineligible patients (EXTREME protocol)
- EGFR amplification in ~80% of hypopharyngeal SCCs makes this a viable target
7. Developments in Early Detection
- Cheng et al. (2025), Medicine, PMID 41204550 - review on advances in diagnosis and treatment of early hypopharyngeal carcinoma and precancerous lesions; narrow band imaging (NBI) and blue laser imaging allow detection of early mucosal changes before macroscopic lesion formation.
8. Intensity-Modulated Proton Therapy (IMPT)
- Spares more normal tissue vs. photon IMRT; reduces xerostomia, dysphagia, hypothyroidism
- Particularly beneficial in bilateral neck treatment scenarios
9. Peripheral Lymphocyte Count as Biomarker
- Lin et al. (2024), PMID 38596906 - peripheral lymphocyte count pre-treatment predicts radiotherapy effectiveness; low baseline lymphocytes correlate with poor local control, suggesting role of immune status in treatment response
SUMMARY TABLE: TEXTBOOK REFERENCES
| Topic | Scott-Brown | Cummings | K.J. Lee | Others |
|---|---|---|---|---|
| Anatomy | Ch.16, pp.317-318 | Ch.92 | p.667 | Dhingra: Ch. Hypopharynx |
| Aetiology | p.318 | - | p.855 | Hazarika |
| Staging | p.321 (AJCC 8th) | Ch.92 | p.856 | Zakir Hussain |
| TLM | p.325 | Ch.93 | p.858 | Stell & Maran |
| Organ Preservation | p.326 | EORTC | p.858 | Bozec 2023 |
| Reconstruction | p.328 | Ch.94 | p.858 | - |
KEY POINTS FOR RGUHS EXAMINATION
- Pyriform sinus = most common subsite of hypopharyngeal cancer (65-75%)
- Most common histology = squamous cell carcinoma
- Apex involvement = precludes conservation surgery (cricoid cannot be preserved)
- Pooling of saliva in pyriform fossa on laryngoscopy is pathognomonic
- Referred otalgia via Arnold's nerve (auricular branch of vagus CN X)
- Lymphatic drainage = jugulodigastric and jugulo-omohyoid nodes (Levels II-III); apex drains to paratracheal (Level VI)
- Occult nodal metastases in 30-40% of N0 necks - mandate elective treatment
- EORTC organ preservation trial by Lefebvre et al. - landmark trial establishing induction chemo + RT as alternative to surgery
- AJCC 8th edition - T4a = moderately advanced; T4b = very advanced
- 5-year survival = 20-50% (stage-dependent); poor overall prognosis due to late presentation
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (8th Ed.) - Chapter 16: Malignant Tumours of the Hypopharynx, pp. 317-334
- Cummings Otolaryngology Head and Neck Surgery (7th Ed.) - Chapter 92-94
- K.J. Lee's Essential Otolaryngology (11th Ed.) - Hypopharyngeal Cancer, pp. 855-858
- Lefebvre JL, Chevalier D, Luboinski B, et al. Larynx preservation in pyriform sinus cancer: preliminary results of a European Organization for Research and Treatment of Cancer phase III trial. J Natl Cancer Inst. 1996;88(13):890-899.
- Lai KWK, Lai R, Lorincz BB. Oncological and Functional Outcomes of TORS and ELPS for Hypopharyngeal Cancer: A Systematic Review. Front Surg. 2022. PMID: 35464886.
- Bozec A, Poissonnet G, Dassonville O. Current Therapeutic Strategies for Hypopharyngeal Carcinoma. J Clin Med. 2023. PMID: 36769885.
- Cheng J, Liu Y, Tang X. Developments in diagnosis and treatment of early hypopharyngeal carcinoma. Medicine (Baltimore). 2025. PMID: 41204550.
- Gong H, Tian S, Ding H, et al. Camrelizumab-based induction chemoimmunotherapy in locally advanced hypopharyngeal carcinoma: phase II trial. Nat Commun. 2024. PMID: 38898018.
- Luo X, Huang X, Liu S, et al. Response-Adapted Treatment in Resectable Locally Advanced Hypopharyngeal Carcinoma. JAMA Netw Open. 2022. PMID: 35191967.
- Dhingra PL & Dhingra S. Diseases of Ear Nose and Throat (7th Ed.) - Carcinoma Pyriform Fossa
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear Nose Throat and Head & Neck Surgery - Hypopharyngeal Malignancies
- Zakir Hussain. ENT for Entrance Examinations - Hypopharynx chapter
Recent Evidence Note: A 2023 review by Bozec et al. (PMID 36769885) confirms the trend toward organ preservation for resectable locally advanced hypopharyngeal carcinoma using concurrent chemoradiation rather than upfront total laryngopharyngectomy, with non-inferior survival outcomes. Immunotherapy integration (particularly PD-1 inhibitors) in the induction setting represents the most significant recent advance, potentially improving organ preservation rates further.
This is a shared conversation. Sign in to Orris to start your own chat.