Swelling due to corticosteroids
Reading File
Searching PubMed
corticosteroid edema sodium retention mechanism
Finding Sources
Finding Sources
Searching PubMed
corticosteroid adverse effects fluid retention edema
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough answer. Here it is:
Swelling Due to Corticosteroids
Swelling from corticosteroids is a well-recognized adverse effect that occurs through two distinct but related mechanisms: mineralocorticoid-mediated fluid/sodium retention and fat redistribution producing a characteristic cushingoid appearance.
1. Mechanism: Mineralocorticoid Activity and Sodium Retention
Corticosteroids vary in their relative glucocorticoid vs. mineralocorticoid potency. When mineralocorticoid activity is significant, the drug acts on renal tubular mineralocorticoid receptors - just as aldosterone does - causing:
- Na+ reabsorption in the distal nephron
- Water retention following sodium (osmotically driven)
- K+ and H+ secretion in exchange
- Expansion of extracellular fluid volume - clinically appearing as peripheral edema
This mechanism is most pronounced with:
- Hydrocortisone and cortisone (salt-retaining effect = 1 relative to hydrocortisone)
- Prednisone / prednisolone (mild salt-retaining effect = 0.8)
- Methylprednisolone (salt-retaining = 0.5)
In contrast, dexamethasone and betamethasone have essentially zero mineralocorticoid activity (salt-retaining = 0) and cause much less sodium-mediated edema.
"Excess mineralocorticoid activity causes sodium retention and hypokalemia and may precipitate congestive heart failure." - Morgan & Mikhail's Clinical Anesthesiology, 7e
The potency comparison chart below (from Lippincott Illustrated Reviews: Pharmacology) shows this clearly:
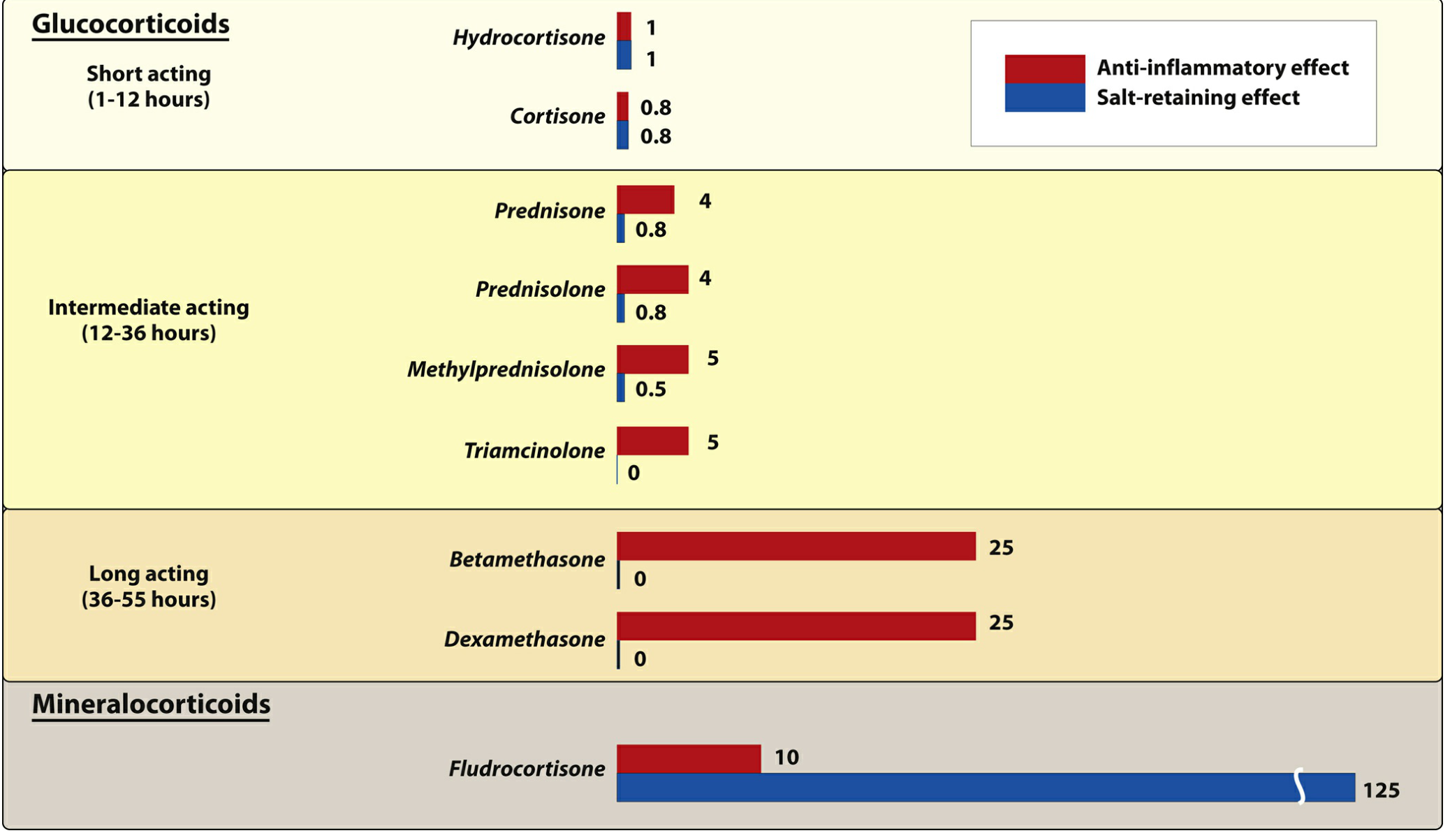
Figure: Anti-inflammatory (red) vs. salt-retaining/mineralocorticoid (blue) effects of corticosteroids relative to hydrocortisone = 1. Note fludrocortisone has a salt-retaining effect of 125.
2. The 11β-HSD2 Overflow Mechanism (High-Dose Glucocorticoids)
Normally, the enzyme 11β-hydroxysteroid dehydrogenase type 2 (11β-HSD2) in the renal tubules converts cortisol to inactive cortisone, protecting mineralocorticoid receptors from cortisol activation. However, when glucocorticoid levels are very high (as in exogenous steroid therapy or Cushing syndrome), this protective enzyme is overwhelmed, and cortisol floods and activates mineralocorticoid receptors, causing:
- Sodium retention
- Hypertension
- Hypokalemia
"When circulating cortisol concentrations are extremely high, as in Cushing syndrome, this mechanism for cortisol metabolism may be overwhelmed. As a result, the high levels of cortisol strongly activate mineralocorticoid receptors and cause sodium retention, hypertension, and hypokalemia." - Guyton and Hall Textbook of Medical Physiology
3. Fat Redistribution: Cushingoid Swelling
Beyond true fluid edema, prolonged corticosteroid therapy causes abnormal fat redistribution that creates a "swollen" or puffy appearance:
| Feature | Description |
|---|---|
| Moon face | Rounded, edematous-appearing face due to fat deposition in cheeks/temples |
| Buffalo hump | Dorsocervical fat pad between the shoulder blades |
| Truncal/central obesity | Fat deposited in thoracic and upper abdominal regions |
| Limb fat loss | Fat mobilized from the lower body, making limbs appear thin despite truncal swelling |
"A special characteristic of Cushing syndrome is mobilization of fat from the lower part of the body, with concomitant extra deposition of fat in the thoracic and upper abdominal regions, giving rise to a buffalo-like torso. The excess secretion of steroids also leads to an edematous appearance of the face... frequently described as a 'moon face'." - Guyton and Hall Textbook of Medical Physiology
The classic moon face appearance (before vs. after treatment):

Figure 78.11 - A patient with Cushing syndrome before (left) and after (right) subtotal adrenalectomy. Courtesy Dr. Leonard Posey. (Guyton and Hall Textbook of Medical Physiology)
4. Clinical Summary Table
| Type of Swelling | Cause | Typical Location | Reversible? |
|---|---|---|---|
| Peripheral edema | Na+/water retention (mineralocorticoid effect) | Ankles, feet, legs | Yes, on dose reduction |
| Moon face | Fat redistribution + edema | Face | Yes, slowly after stopping |
| Buffalo hump | Fat redistribution | Dorsocervical region | Partially, may take months |
| Truncal obesity | Central fat deposition | Abdomen, thorax | Partially |
5. Which Corticosteroids Cause More vs. Less Swelling?
More edema risk (higher mineralocorticoid activity):
- Hydrocortisone, cortisone, fludrocortisone
Moderate edema risk:
- Prednisone, prednisolone, methylprednisolone
Less edema risk (negligible mineralocorticoid activity):
- Dexamethasone, betamethasone, triamcinolone
Note that even dexamethasone can cause moon face and fat redistribution via glucocorticoid mechanisms, despite not causing sodium-mediated peripheral edema.
6. Management
-
Use the lowest effective dose for the shortest duration
-
Prefer agents with lower mineralocorticoid activity (e.g., dexamethasone) when edema is a concern
-
Dietary sodium restriction and potassium supplementation
-
Diuretics (e.g., spironolactone or thiazides) if edema is clinically significant
-
Monitor blood pressure and weight regularly
-
Guyton and Hall Textbook of Medical Physiology (Cushing syndrome section, p. 954-958)
-
Morgan & Mikhail's Clinical Anesthesiology, 7e (Corticosteroids section, p. 2034)
-
Lippincott Illustrated Reviews: Pharmacology (Corticosteroids, p. 872-874)
How do I manage edema in a patient on long-term prednisone stop after 15 days
Finding Sources
Finding Sources
Searching PubMed
corticosteroid edema management treatment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I have all the information needed. Here is the complete, evidence-based answer:
Managing Edema in a Patient Stopping Prednisone After 15 Days
The key clinical insight here is that 15 days is a short course. This fundamentally changes management - the approach is different from a patient on months of prednisone.
Step 1: Can Prednisone Be Stopped Abruptly?
Yes - 15 days is safe to stop abruptly (no taper needed).
"If glucocorticoids are no longer required for the control of the underlying disease and the treatment duration is <3-4 weeks, glucocorticoids can be stopped abruptly."
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Patients on long-term therapy (>3-4 weeks at supraphysiologic doses) are at risk of glucocorticoid-induced adrenal insufficiency (GI-AI) and require a gradual taper down to physiologic dose (3-5 mg prednisone equivalent). But at 15 days, HPA axis suppression is minimal and abrupt discontinuation is appropriate if the underlying condition no longer requires treatment.
Important caveat: If the patient is on a high dose (e.g., >40 mg/day), some clinicians still prefer a brief step-down over 3-5 days just to avoid rebound symptoms, though this is not strictly necessary for <3 weeks.
Step 2: What Happens to the Edema After Stopping?
Once prednisone is discontinued:
- The mineralocorticoid-mediated sodium and water retention resolves within days to 1-2 weeks
- Peripheral edema (ankles, feet) will gradually mobilize and resolve as urinary sodium excretion normalizes
- No specific anti-edema treatment may be needed at all - simply stopping prednisone may be sufficient
Step 3: Active Management of the Edema (While Still on Prednisone or If Edema Persists)
If the prednisone cannot be stopped yet, or if edema persists after stopping, use a stepwise approach:
Non-Pharmacologic (First-Line)
| Measure | Details |
|---|---|
| Dietary sodium restriction | <2 g/day sodium diet - reduces the mineralocorticoid-driven Na+ retention load |
| Leg elevation | Elevate legs above heart level for 30+ minutes several times daily to promote venous return |
| Compression stockings | Class I-II (15-30 mmHg) for bilateral leg edema, improves lymphatic and venous drainage |
| Fluid restriction | Modest fluid restriction if significant volume overload |
| Physical activity | Walking activates the calf muscle pump and reduces dependent edema |
Pharmacologic (Second-Line, if Non-Pharmacologic Measures Fail)
| Drug | Rationale | Dose |
|---|---|---|
| Spironolactone | Antagonizes the mineralocorticoid receptor - directly counteracts the mechanism of corticosteroid edema | 25-100 mg/day |
| Furosemide | Loop diuretic for more significant edema; pair with spironolactone at a 40 mg:100 mg ratio to maintain potassium balance | 20-40 mg/day |
| Potassium supplementation | Prednisone promotes K+ loss via mineralocorticoid effect - monitor and replace | As indicated by serum K+ |
Spironolactone is particularly elegant here because it directly antagonizes aldosterone/mineralocorticoid receptors - targeting the exact mechanism by which corticosteroids cause edema - while also being potassium-sparing (counteracting the hypokalemia risk).
Step 4: Monitor
| Parameter | Why |
|---|---|
| Blood pressure | Na+ retention raises BP |
| Serum potassium | Corticosteroids promote K+ wasting; diuretics (especially furosemide) compound this |
| Blood glucose | Prednisone causes insulin resistance; monitor especially in diabetics |
| Body weight | Track daily weight as a proxy for fluid status during diuresis |
Summary Algorithm for This Patient
15-day prednisone course ending
↓
Underlying disease controlled?
↓ YES
Stop prednisone abruptly (no taper needed)
↓
Advise patient: edema should resolve over 1-2 weeks
↓
Non-pharmacologic: low-salt diet, leg elevation, compression stockings
↓
Edema persists >2 weeks after stopping?
↓
Add spironolactone 25-50 mg/day ± furosemide
Monitor K+ and BP
Bottom line: For a 15-day course, the single most effective intervention for the edema is simply stopping the prednisone - the mineralocorticoid-driven fluid retention will self-resolve. Support this with a low-sodium diet and leg elevation. Reserve diuretics (spironolactone preferred) for cases where edema is symptomatic, the prednisone cannot be stopped, or if edema persists unexpectedly after discontinuation.
- Harrison's Principles of Internal Medicine, 22e (Glucocorticoid-Induced Adrenal Insufficiency, p. 3114)
- Frameworks for Internal Medicine (Peripheral Edema Management)
- Morgan & Mikhail's Clinical Anesthesiology, 7e (Corticosteroids)
This is a shared conversation. Sign in to Orris to start your own chat.