Knee replacement surgery
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"knee replacement" OR "total knee arthroplasty"
Searching the Web
total knee replacement surgery overview indications complications rehabilitation medical
Finding Sources
Reading Web Page
https://emedicine.medscape.com/article/1250275-overview
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have very comprehensive content. Let me compile the full, well-structured answer for a medical student.
Total Knee Arthroplasty (TKA) - Comprehensive Overview
Sources: Miller's Review of Orthopaedics 9th Ed (2024), Campbell's Operative Orthopaedics 15th Ed (2026), Medscape, AAOS
1. Epidemiology & Background
Total knee arthroplasty (TKA) is one of the most commonly performed elective surgical procedures worldwide. In the United States alone, over 700,000 primary TKAs are performed annually (AAOS), with 194,695 reported by the American Joint Replacement Registry in 2022. The procedure has been refined over the past 50+ years as understanding of knee biomechanics improved.
2. Indications
The primary indication is significant, disabling knee pain due to end-stage arthritis that fails conservative management.
Absolute indications:
- Debilitating pain affecting activities of daily living
- Pain not well controlled by conservative measures (physiotherapy, NSAIDs, intra-articular injections, walking aids)
- Medical fitness for surgery
- No active infection - anywhere in the body
Causes requiring TKA:
| Cause | Notes |
|---|---|
| Osteoarthritis | Most common indication - cartilage degeneration with loss of shock absorption |
| Rheumatoid arthritis | Inflammatory destruction, often multi-joint |
| Post-traumatic arthritis | Younger patients; finite implant lifespan must be discussed |
| Avascular necrosis | End-stage joint destruction |
| Severe deformity | Significant varus/valgus or flexion contracture can itself be an indication |
| Isolated patellofemoral arthritis | Rarely justifies TKA; isolated PF replacement still under investigation |
Age considerations: Although traditionally performed in older patients (lower activity demands), TKA is not excluded by age. Younger patients with significant disability may be candidates but must understand limitations on implant longevity.
3. Contraindications
Absolute:
- Active joint or systemic infection
- Absent or non-functional extensor mechanism
- Severe peripheral vascular disease compromising wound healing
- Neuropathic arthropathy (relative - higher failure rates)
Relative:
- Morbid obesity (BMI >40 - increased infection, implant failure, complications)
- Poorly controlled diabetes (elevated HbA1c or fructosamine)
- Active immunosuppression (requires perioperative medication management)
4. Types of Knee Replacement
By Extent
| Type | Description | Key Indication |
|---|---|---|
| Total (TKA) | Replaces femoral condyles + tibial plateau (+/- patella) | Tricompartmental OA |
| Unicompartmental (UKA) | Replaces one tibiofemoral compartment (usually medial) | Isolated single-compartment OA, intact ACL, correctable deformity |
| Patellofemoral arthroplasty | Replaces trochlea and patella only | Isolated patellofemoral OA |
| Revision TKA | Replaces failed primary implants | Aseptic loosening, infection, instability, wear |
By Posterior Cruciate Ligament (PCL) Management
| Design | PCL Fate | Key Feature |
|---|---|---|
| Cruciate-Retaining (CR) | Preserved | Requires intact PCL; maintains more natural kinematics; technically demanding |
| Posterior-Stabilized (PS) | Sacrificed | Femoral "cam-post" mechanism substitutes PCL function; allows more correction; risk of notching femoral condyle |
| Constrained/Hinged | Sacrificed | Used for severe deformity, ligament deficiency, or revision cases; mechanical hinge increases bone-implant stress |
By Fixation
- Cemented: Gold standard. Uses polymethylmethacrylate (PMMA) cement. Best long-term data.
- Uncemented (cementless): Bioactive surfaces (hydroxyapatite) allow bony ingrowth. Promising mid-term results; preferred in younger, more active patients.
- Hybrid: Cemented tibia + uncemented femur (or vice versa).
By Bearing Surface
- Fixed-bearing polyethylene: Standard; polyethylene is fixed to tibial tray
- Mobile-bearing (rotating platform): Polyethylene can rotate; theoretically reduces wear but no proven clinical superiority
5. Implant Materials
| Component | Material |
|---|---|
| Femoral component | Cobalt-chromium alloy or titanium alloy |
| Tibial baseplate | Titanium or cobalt-chromium |
| Tibial insert (bearing) | Ultra-high molecular weight polyethylene (UHMWPE) |
| Patellar button (if resurfaced) | UHMWPE or metal-backed polyethylene |
6. Surgical Technique Overview
Positioning & Approach
- Supine position, tourniquet applied to thigh
- Standard approach: medial parapatellar arthrotomy (most common)
- Patella is everted (or subluxed) to expose the joint
- Anesthesia: regional (spinal/epidural) preferred; equivalent outcomes to GA
Bone Cuts - "Gap Balancing"
The surgeon makes 5 cuts to shape the distal femur and proximal tibia so the prosthetic gaps are equal in flexion and extension:
- Distal femoral cut - perpendicular to the mechanical axis of femur (creates the extension gap)
- Proximal tibial cut - perpendicular to tibial mechanical axis (usually with 3-7° posterior slope)
- Anterior/posterior femoral cuts - define the flexion gap; size the femoral component
- Chamfer cuts - bevel the femur to match component geometry
- Patellar resurfacing (optional, controversial)
Alignment Philosophies
Mechanical alignment (most common): Restores neutral Mikulicz line (hip-knee-ankle). Distal femoral and proximal tibial cuts made perpendicular to mechanical axes. Requires ligament balancing.
Kinematic alignment: Maintains native limb alignment. Cuts made at native angles. Eliminates need for soft-tissue release, but may create asymmetric implant loading.
At present, no proven superiority of either technique.
Ligament Balancing - Key Principle
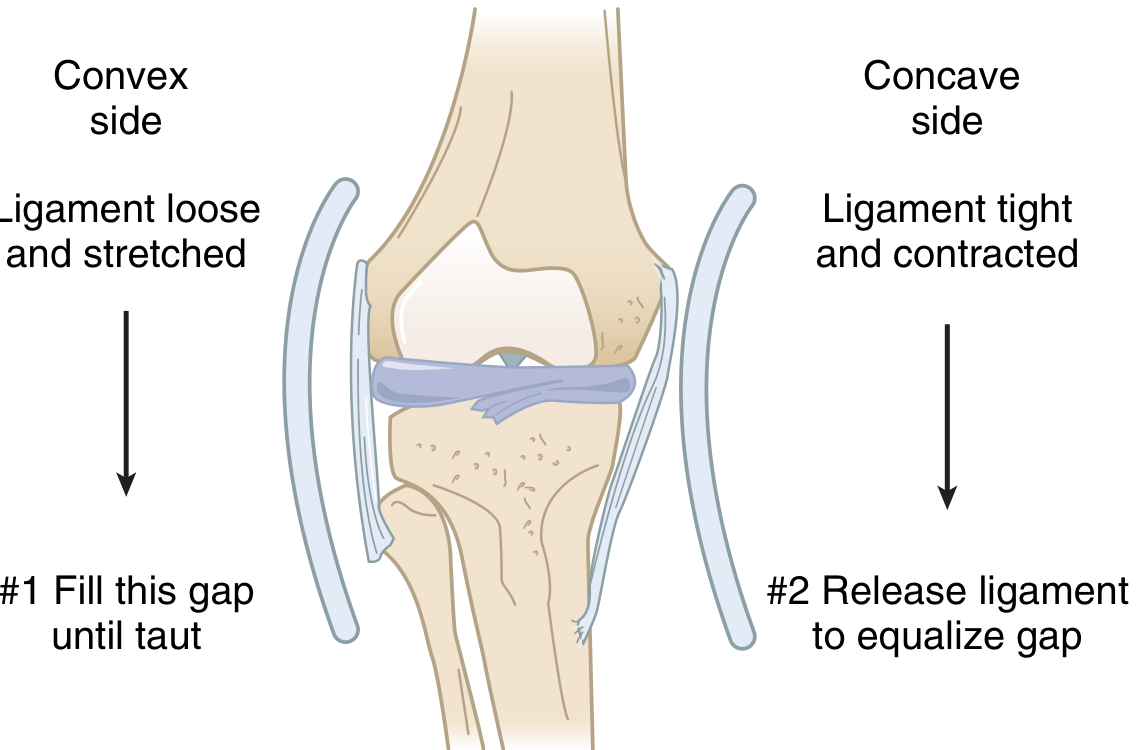
Varus deformity: Concave medial side is tight. Sequential medial release: osteophytes → medial capsule complex (1.5 cm below joint line) → posterior medial corner → superficial MCL (posterior oblique for extension tightness; anterior portion for flexion tightness).
Valgus deformity: Concave lateral side is tight. Sequential lateral release: osteophytes → lateral capsule → iliotibial band (tight in extension) → popliteus tendon.
7. Perioperative Management
Pre-operative Risk Reduction (High-Yield for Exams)
- Avoid intra-articular corticosteroid injection within 2 weeks before TKA (significantly increases infection risk)
- Optimize nutrition: check albumin and prealbumin; supplement as needed
- Glycemic control: check HbA1c or serum fructosamine
- Perioperative management of antirheumatic medications per ACR/AAHKS guidelines:
- Continue through surgery: Methotrexate, hydroxychloroquine, sulfasalazine, leflunomide
- Hold biologics (TNF inhibitors, IL-6, etc.): Hold for one dosing interval before surgery (e.g., adalimumab every 2 weeks - hold until week 3)
- JAK inhibitors (tofacitinib, baricitinib, upadacitinib): Hold 3 days prior
Anesthesia & Analgesia
- Multimodal analgesia is the standard: combines regional blocks + NSAIDs + acetaminophen +/- opioids
- NSAIDs (including IV ketorolac within 24h) reduce pain and opioid consumption
- Pregabalin reduces opioid consumption after discharge; gabapentinoids do NOT reduce postoperative pain in the perioperative period
- Nerve blocks:
- Femoral nerve block (FNB): Motor + sensory block; good analgesia but causes quadriceps weakness → fall risk → requires knee immobilizer
- Adductor canal block (ACB): Sensory-only block; preserves quad function; allows earlier ambulation; equivalent analgesia to FNB. ACB + periarticular block (PAB) provides additive benefit
- iPACK block: Targets posterior capsule; fills posterior knee coverage gap left by ACB/FNB
VTE Prophylaxis
- DVT is the most common systemic complication
- Chemoprophylaxis (LMWH, aspirin, direct oral anticoagulants) plus mechanical (sequential compression devices) started immediately
8. Complications
Intraoperative
| Complication | Notes |
|---|---|
| Femoral condyle fracture | Medial > lateral; more common with PS design (notching weakens condyle) |
| MCL injury | Convert to constrained revision prosthesis + primary MCL repair; brace 6 weeks |
| Peroneal nerve palsy | Risk with valgus + flexion contracture correction; aberrant retractor in posterolateral corner compresses nerve against proximal fibula |
| Lateral superior genicular artery transection | During lateral retinacular release; increases risk of patellar osteonecrosis |
| Extensor mechanism disruption | Usually at patellar tendon-tibial tubercle junction; requires extensor reconstruction |
Postoperative
| Complication | Notes |
|---|---|
| DVT/PE | Most common systemic complication; prophylaxis is mandatory |
| Periprosthetic joint infection (PJI) | Most dreaded; staged two-stage revision is standard for chronic infection |
| Aseptic loosening | Most common cause of late failure; tibial component loosens most often |
| Polyethylene wear | Leads to osteolysis; accelerated by malalignment, high activity |
| Instability | Due to soft tissue imbalance or component malpositioning |
| Patellar fracture | Causes: over-resection (<13 mm remaining), compromised vascularity, maltracking; treatment based on stability, lag, and fixation status |
| Arthrofibrosis | Knee stuck at 70-85° flexion; manipulation at 4-12 weeks (6-8 weeks ideal); late manipulation risks femur fracture |
| Peroneal nerve palsy | First treatment: remove compressive dressings + flex the knee; AFO support until recovery (~3 months); if no recovery by 3 months and nerve intact on EMG/NCS → surgical decompression |
| Aseptic loosening | Leading cause of revision |
9. Postoperative Rehabilitation
Immediate mobilization: Start within 24 hours of surgery. Early mobilization reduces DVT, improves outcomes, and lowers costs.
Phase-based rehab protocol:
| Phase | Timing | Goals |
|---|---|---|
| Phase I | 0-2 weeks | Quad activation, SLR, ankle pumps, ROM 0-90°, ambulate with aids |
| Phase II | 4-6 weeks | Wean walking aids, increase ROM, begin strengthening |
| Phase III | 6-8 weeks | Functional activities, stairs, improved balance |
| Phase IV | 8-12 weeks to 1 year | Return to full activities, resistance training |
Active resistance exercise (lower limb) post-TKA improves mobility, physical function, knee strength, and pain intensity (recent 2024 systematic review, PMID 39267026).
Cryotherapy has been studied for post-TKA recovery; recent systematic reviews (PMID 37706609, 39402654) show modest benefit for pain but limited impact on long-term function.
10. Outcomes & Implant Survivorship
- TKA is highly effective: 85-90%+ survivorship at 15-20 years for cemented designs
- Patient satisfaction: ~80-85% of patients are satisfied (about 15-20% report dissatisfaction, often due to persistent pain, stiffness, or unmet expectations)
- Robotic-assisted TKA is an emerging technology; recent meta-analyses (PMID 38133653, 39052153) show improved component positioning accuracy but no definitive long-term functional superiority over conventional TKA yet
Causes of Revision (Know These)
- Aseptic loosening (most common, especially tibial component)
- Infection / PJI
- Instability
- Polyethylene wear / osteolysis
- Periprosthetic fracture
- Stiffness / arthrofibrosis
- Extensor mechanism failure
Key Exam Points (High-Yield Summary)
- #1 indication: Debilitating OA pain failing conservative therapy
- Corticosteroid injection within 2 weeks of surgery = highest infection risk
- PS vs CR design: PS sacrifices PCL; PS notches femur → higher condylar fracture risk
- Varus deformity → medial release; Valgus → lateral release (ITB is key lateral structure)
- Peroneal palsy → first: flex knee + remove dressings. No surgery unless no recovery at 3 months
- Patellar fracture with minimal lag (<10°) + stable TKA → treat conservatively (cast/brace; NO therapy!)
- Arthrofibrosis → manipulation at 6-8 weeks; late manipulation risks femur fracture
- MCL injury intraoperatively → constrained revision prosthesis
- ACB preferred over FNB for early ambulation (no quad weakness)
- Hold biologics one dosing interval before surgery; JAK inhibitors 3 days before; continue MTX/HCQ
Sources: Miller's Review of Orthopaedics 9th Ed (2024), Campbell's Operative Orthopaedics 15th Ed (2026), Medscape TKA reference, AAOS OrthoInfo
This is a shared conversation. Sign in to Orris to start your own chat.