Tell me everything about jaundice. It’s physiology, biochemistry, medicine
Reading File
Finding Sources
Searching PubMed
"jaundice" AND "bilirubin metabolism"
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer:
Jaundice: Physiology, Biochemistry, and Medicine
1. Definition and Clinical Detection
Jaundice (icterus) is the yellowish discoloration of the skin, sclera, and mucous membranes caused by deposition of the pigment bilirubin. It becomes clinically visible when total plasma bilirubin exceeds 2-3 mg/dL (34-51 µmol/L). The sclera shows the discoloration most reliably because scleral tissue has a high affinity for bilirubin due to its elastin content. Detection can be harder under fluorescent lighting, which may require higher plasma levels before jaundice is apparent.
- Tietz Textbook of Laboratory Medicine, p. 1982
- Ganong's Review of Medical Physiology, p. 514
2. Bilirubin Biochemistry: Production to Excretion
A. Bilirubin Production (Prehepatic)
About 80-85% of bilirubin comes from the breakdown of senescent red blood cells (RBCs) in the reticuloendothelial system (spleen, liver, bone marrow). The remaining 15-20% comes from other heme-containing proteins: myoglobin, cytochromes P450, catalase, and peroxidases ("ineffective erythropoiesis").
The pathway:
- Heme → Biliverdin: The enzyme heme oxygenase cleaves the heme ring, releasing iron (Fe²⁺), carbon monoxide (CO), and biliverdin (green pigment).
- Biliverdin → Bilirubin: The enzyme biliverdin reductase converts biliverdin to bilirubin (yellow pigment). This bilirubin is called unconjugated (indirect) bilirubin - it is lipid-soluble, water-insoluble, and tightly bound to albumin in plasma. It cannot be filtered by the kidneys and does not appear in urine.
B. Hepatic Uptake
Unconjugated bilirubin bound to albumin is transported to the liver. At the hepatocyte sinusoidal surface, it dissociates from albumin and is taken up by specific transport proteins (OATP1B1 and OATP1B3). Inside the hepatocyte, it is bound to intracellular proteins (especially ligandin/glutathione-S-transferase Y) to prevent efflux back into the circulation.
C. Conjugation in the Liver
Inside hepatocytes, unconjugated bilirubin is conjugated with glucuronic acid by UDP-glucuronosyltransferase (UGT1A1) in the smooth endoplasmic reticulum, forming bilirubin mono- and diglucuronide (conjugated/direct bilirubin). This renders it water-soluble, allowing excretion into bile.
D. Canalicular Excretion
Conjugated bilirubin is actively transported across the hepatocyte canalicular membrane into the bile canaliculi by the MRP2 (multidrug resistance protein 2 / ABCC2) transporter. This is the rate-limiting step in bilirubin excretion.
E. Intestinal Fate: Urobilinogen/Stercobilin
In the intestine, bacterial enzymes (beta-glucuronidases from colonic flora) deconjugate and reduce conjugated bilirubin to urobilinogen:
- Most urobilinogen is oxidized to stercobilin and excreted in stool, giving stool its brown color.
- A small fraction is reabsorbed (enterohepatic circulation), returned to the liver, and re-excreted.
- A tiny fraction escapes into the systemic circulation and is filtered by the kidneys, excreted as urobilinogen in urine.
In complete bile duct obstruction: No bilirubin reaches the gut → no urobilinogen/stercobilin → pale/acholic stools and absent urine urobilinogen. Conjugated bilirubin backs up into blood, and because it is water-soluble, it spills into urine → dark (tea-colored) urine.
- Ganong's Review of Medical Physiology, pp. 513-514
- Tietz Textbook of Laboratory Medicine, p. 1982
- Schwartz's Principles of Surgery, p. 1381
3. Classification of Jaundice
Jaundice is classified by where in the metabolic pathway the dysfunction occurs:
| Type | Location | Bilirubin Type Elevated | Urine Bilirubin | Urine Urobilinogen | Stool Color |
|---|---|---|---|---|---|
| Prehepatic | Before liver | Unconjugated (indirect) | Absent | Increased | Normal/dark |
| Intrahepatic | Within liver | Both (mixed) | Present | Variable | Variable |
| Posthepatic | After liver (obstruction) | Conjugated (direct) | Present (dark urine) | Absent | Pale/acholic |
4. Prehepatic Jaundice
Caused by excessive bilirubin production overwhelming the liver's conjugation capacity.
Inherited hemolytic disorders:
- Hereditary spherocytosis
- Sickle cell anemia
- Thalassemia
- G6PD deficiency
- Pyruvate kinase deficiency
Acquired hemolytic disorders:
- Microangiopathic hemolytic anemia (HUS, TTP)
- Paroxysmal nocturnal hemoglobinuria (PNH)
- Immune-mediated hemolysis (warm/cold autoimmune, drug-induced)
- Infections: malaria, babesiosis
- Mechanical trauma (prosthetic heart valves)
Other causes:
- Ineffective erythropoiesis: cobalamin, folate, or iron deficiency
- Resorption of large hematomas
- Massive blood transfusion
In hemolytic disorders, serum bilirubin rarely exceeds 5 mg/dL unless there is concurrent hepatic dysfunction. An important complication: chronic hemolysis predisposes to pigmented (calcium bilirubinate) gallstones, so choledocholithiasis must be considered when bilirubin rises sharply in these patients.
Drugs that impair hepatic bilirubin uptake (causing unconjugated hyperbilirubinemia): rifampin, probenecid, atazanavir, certain cephalosporins and penicillins.
- Harrison's Principles of Internal Medicine 22E, p. 366-367
5. Intrahepatic Jaundice
A. Hereditary/Genetic Disorders of Bilirubin Metabolism
Unconjugated hyperbilirubinemia (conjugation defects):
| Syndrome | Mechanism | Bilirubin Level | Clinical Features |
|---|---|---|---|
| Gilbert's syndrome | Reduced UGT1A1 promoter activity (10-35% of normal) | <6 mg/dL, fluctuating | Benign; 3-7% of population; triggered by fasting, stress, illness, alcohol; may be protective |
| Crigler-Najjar type II | UGT1A1 mutations, <10% enzyme activity | 6-25 mg/dL | Survives into adulthood; phenobarbital lowers levels |
| Crigler-Najjar type I | Complete absence of UGT1A1 | >20 mg/dL | Fatal in infancy without treatment; kernicterus; liver transplant required |
Conjugated hyperbilirubinemia (excretion defects):
| Syndrome | Defect | Features |
|---|---|---|
| Dubin-Johnson syndrome | Mutation in MRP2 (ABCC2) - blocks canalicular bilirubin excretion | Darkly pigmented liver (polymerized epinephrine metabolites), otherwise benign; hepatomegaly |
| Rotor syndrome | Deficiency of OATP1B1 and OATP1B3 (hepatic reuptake transporters) | Similar to Dubin-Johnson but no liver pigmentation; both benign |
B. Hepatocellular Disease
Any condition that damages hepatocytes impairs both conjugation and excretion. Common causes:
- Viral hepatitis (A, B, C, D, E; also EBV, CMV)
- Alcoholic hepatitis / alcoholic liver disease
- Non-alcoholic fatty liver disease (NAFLD) / steatohepatitis
- Drug-induced liver injury (DILI): acetaminophen (commonest), isoniazid, statins, herbal preparations
- Autoimmune hepatitis
- Wilson's disease (in patients <40 years)
- Hemochromatosis
- Acute liver failure (any cause)
- Ischemic hepatitis ("shock liver") from hypoperfusion
Lab pattern: ALT/AST elevated out of proportion to alkaline phosphatase (hepatocellular pattern).
C. Intrahepatic Cholestasis
Impaired bile flow within the liver without extrahepatic obstruction:
- Primary biliary cholangitis (PBC): autoimmune destruction of intrahepatic bile ducts; anti-mitochondrial antibody (AMA) positive
- Primary sclerosing cholangitis (PSC): fibro-inflammatory stricturing of bile ducts; strongly associated with IBD
- Drug-induced cholestasis: anabolic steroids, oral contraceptives, chlorpromazine
- Intrahepatic cholestasis of pregnancy
- Sepsis-associated cholestasis
Lab pattern: Alkaline phosphatase and GGT elevated out of proportion to ALT/AST (cholestatic pattern).
- Robbins & Kumar Basic Pathology, p. 2128
- Harrison's Principles of Internal Medicine 22E, pp. 367-370
6. Posthepatic (Obstructive) Jaundice
Caused by mechanical obstruction of the bile duct system (biliary tree), preventing bile flow into the duodenum.
Intrinsic Causes:
- Choledocholithiasis (most common) - stones in the common bile duct; can range from mild right upper quadrant pain to ascending cholangitis (Charcot's triad: fever/rigors, RUQ pain, jaundice; Reynolds' pentad adds hypotension and altered mental status)
- Cholangiocarcinoma (Klatskin tumor at the hilum)
- Benign biliary strictures (post-operative, post-inflammatory)
- IgG4-associated cholangitis (responsive to steroids - must differentiate from PSC)
- PSC (with extrahepatic component)
- Ampullary carcinoma (highest surgical cure rate among periampullary tumors)
- AIDS cholangiopathy (CMV, cryptosporidia)
Extrinsic Causes:
-
Pancreatic cancer (head of pancreas causing "painless jaundice" - classic presentation)
-
Gallbladder cancer
-
Chronic pancreatitis (stricture of distal CBD)
-
Pancreatic pseudocyst
-
Hilar lymphadenopathy from metastases
-
Surgical complications: clip injuries, retained stones, ischemic bile duct injury
-
Schwartz's Principles of Surgery, p. 1381
7. Morphology of Cholestasis (Pathology)
Microscopically, both obstructive and non-obstructive cholestasis show:
- Bile plugs: elongated green-brown plugs in dilated canaliculi
- Feathery degeneration: bile droplets accumulating in hepatocytes, giving a foamy appearance
- Kupffer cell activation: phagocytose extravasated bile after canalicular rupture
- Occasional apoptotic hepatocytes
In prolonged obstruction, secondary changes include: portal tract edema, neutrophilic infiltration, proliferation of bile ductules ("ductular reaction"), and eventually biliary fibrosis/cirrhosis.
- Robbins & Kumar Basic Pathology, pp. 2128-2140
8. Neonatal Jaundice
Physiologic jaundice of the newborn occurs in almost all neonates because hepatic UGT1A1 activity does not fully mature until ~2 weeks of age. This causes transient unconjugated hyperbilirubinemia, which can be worsened by breastfeeding (breast milk contains bilirubin-deconjugating enzymes).
Treatment: Phototherapy with blue light (wavelength ~460 nm) converts bilirubin to water-soluble photoisomers (lumirubin, configurational isomers) that are excreted in urine and bile without needing conjugation. Exchange transfusion is used in severe cases.
Pathological neonatal jaundice (beyond 2 weeks, or very high levels): Think Crigler-Najjar, biliary atresia, neonatal hepatitis, metabolic disorders.
Kernicterus: Unconjugated bilirubin (>20 mg/dL in neonates) crosses the immature blood-brain barrier and deposits in the basal ganglia and brainstem, causing permanent neurologic damage (cerebral palsy, hearing loss, intellectual disability).
- Robbins & Kumar Basic Pathology, p. 2118
9. Clinical Evaluation of Jaundice
Diagnostic Flowchart (Harrison's, Fig. 52-1):
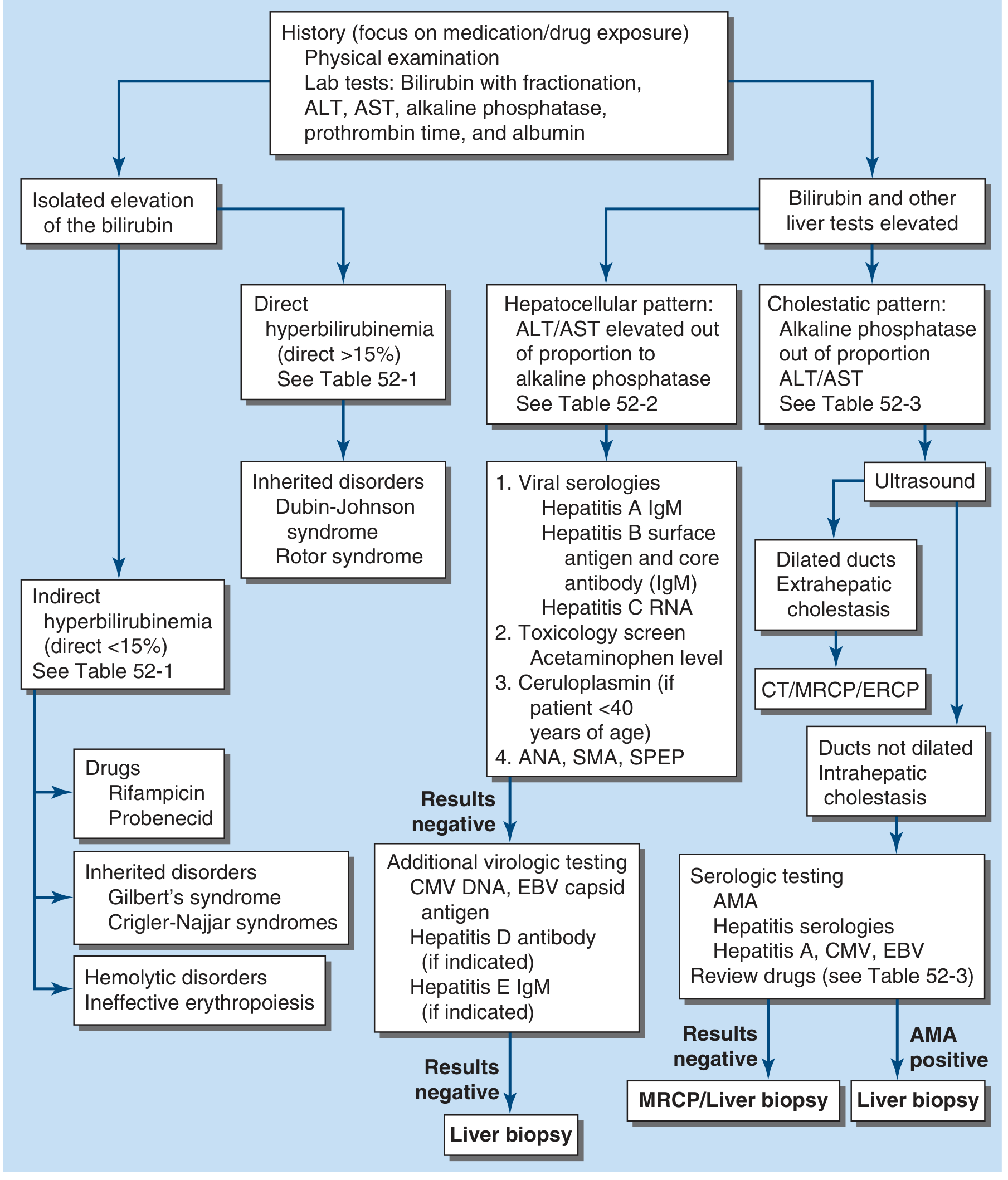
Evaluation of the patient with jaundice. The algorithm branches from lab findings into isolated bilirubin elevation vs. elevation with other liver tests, then further subdivides by direct vs. indirect and hepatocellular vs. cholestatic patterns.
History - Key Questions:
- Drug exposure: prescribed, OTC, herbal/supplements, anabolic steroids (commonest cause of DILI)
- Alcohol use history
- IV drug use, tattoos, sexual history (hepatitis B/C risk)
- Travel history (malaria, hepatitis E in endemic areas)
- Family history (hereditary conditions)
- Associated symptoms: pain (RUQ suggests choledocholithiasis; painless jaundice suggests malignancy), fever (infection, cholangitis), pruritus (cholestasis), weight loss (malignancy), dark urine + pale stools (obstructive pattern)
Physical Examination:
- Scleral icterus: earliest sign
- Hepatomegaly: hepatitis, infiltration, congestion
- Splenomegaly: portal hypertension, hemolysis
- Murphy's sign: cholecystitis
- Courvoisier's sign: palpable, non-tender gallbladder in the setting of painless jaundice suggests malignant obstruction (not gallstones, which cause a shrunken, fibrotic GB)
- Stigmata of chronic liver disease: spider nevi, palmar erythema, gynecomastia, caput medusae, asterixis
- Xanthomas/xanthelasmas: chronic cholestasis
- Lymphadenopathy: infection, lymphoma, metastases
Laboratory Tests:
| Test | Prehepatic | Hepatocellular | Cholestatic/Obstructive |
|---|---|---|---|
| Total bilirubin | Elevated | Elevated | Elevated |
| Direct (conjugated) | Normal (<15%) | Elevated | Elevated |
| Indirect (unconjugated) | Elevated | Elevated | Normal/mildly elevated |
| ALT/AST | Normal | Markedly elevated | Mildly elevated |
| Alkaline phosphatase | Normal | Mildly elevated | Markedly elevated |
| GGT | Normal | Elevated | Markedly elevated |
| Albumin | Normal | Low (chronic) | Normal (early) |
| Prothrombin time | Normal | Prolonged | Prolonged (corrects with Vit K in obstruction) |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | Elevated | Variable | Absent |
| Haptoglobin | Decreased | Normal | Normal |
| LDH | Elevated | Elevated | Normal |
Imaging:
- Ultrasound (first-line): identifies dilated bile ducts (suggesting obstruction), gallstones, liver parenchymal changes. Sensitivity ~60% for choledocholithiasis.
- CT abdomen: better for pancreatic masses, lymphadenopathy, hepatic lesions.
- MRCP (Magnetic Resonance Cholangiopancreatography): non-invasive, excellent visualization of biliary tree - preferred for suspected choledocholithiasis when US is negative.
- ERCP (Endoscopic Retrograde Cholangiopancreatography): both diagnostic and therapeutic - can remove stones, place stents, sample strictures. Reserved for when intervention is anticipated.
- EUS (Endoscopic Ultrasound): excellent for ampullary lesions, distal CBD stones, pancreatic head masses.
- Liver biopsy: definitive for intrahepatic cholestasis, autoimmune hepatitis, unexplained hepatocellular disease.
- Harrison's Principles of Internal Medicine 22E, pp. 366-371
- Schwartz's Principles of Surgery, pp. 1381-1382
10. Complications of Jaundice
Pruritus
Caused primarily by cholestasis. Bile acid accumulation in the skin was historically thought to be the cause, but current evidence points to endogenous opioids and lysophosphatidic acid as the main mediators. Treatment: cholestyramine (bile acid resin), rifampicin, naltrexone (opioid antagonist), SSRI (sertraline), antihistamines.
Coagulopathy
Bile is required for absorption of fat-soluble vitamins, including Vitamin K. Obstructive jaundice impairs Vitamin K absorption → decreased synthesis of clotting factors II, VII, IX, X. In obstruction, PT normalizes with IV Vitamin K; in hepatocellular failure, it does not (because the liver cannot synthesize the factors even with adequate Vit K).
Malabsorption
Fat-soluble vitamin deficiencies (A, D, E, K), steatorrhea.
Kernicterus (in neonates)
Unconjugated bilirubin neurotoxicity - see Section 8.
Biliary cirrhosis
Prolonged intrahepatic or extrahepatic obstruction → secondary biliary cirrhosis, portal hypertension, liver failure.
11. Global Considerations
In developed countries, the most common causes of new-onset jaundice are extrahepatic biliary obstruction (choledocholithiasis, malignancy) and drug-induced liver injury.
In developing countries, infections remain the leading cause: malaria, viral hepatitis A and E, leptospirosis, typhoid fever, viral hemorrhagic fevers, and parasitic infections (schistosomiasis, clonorchiasis, ascariasis).
Acute liver failure is signaled by jaundice + encephalopathy + coagulopathy with no prior liver disease - this is a medical emergency requiring urgent liver transplant evaluation.
- Harrison's Principles of Internal Medicine 22E, p. 370
12. Key Drug-Induced Causes (Summary)
| Drug | Mechanism |
|---|---|
| Rifampin, probenecid, atazanavir | Inhibit hepatic bilirubin uptake → unconjugated hyperbilirubinemia |
| Acetaminophen (overdose) | Hepatocellular necrosis (via NAPQI toxicity) |
| Isoniazid, pyrazinamide | Hepatocellular injury |
| Anabolic steroids, OCP | Intrahepatic cholestasis |
| Chlorpromazine | Cholestatic jaundice |
| Phenobarbital | Induces UGT1A1 (used therapeutically in Crigler-Najjar type II) |
Recent Evidence (PubMed, 2025-2026)
- A 2025 review in American Family Physician (PMID: 39823630) outlines a systematic approach to jaundice evaluation in adults, consistent with the framework above.
- A 2026 review in Pediatric Research (PMID: 40973744) covers translational perspectives on bilirubin biology, noting emerging evidence for bilirubin's cytoprotective and antioxidant roles at mild elevations.
- A 2025 review in Int J Mol Sci (PMID: 41226827) provides updated data on bilirubin photoisomers in neonatal jaundice, relevant to phototherapy optimization.
Sources consulted:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - Chapter 52
- Schwartz's Principles of Surgery, 11th Ed.
- Ganong's Review of Medical Physiology, 26th Ed.
- Robbins & Kumar Basic Pathology
- Tietz Textbook of Laboratory Medicine, 7th Ed.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.