Middle ear mucosal folds. MS ent university exam format for 20 marks as per standard textbooks.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple standard textbooks. Let me compile the complete 20-mark MS ENT university exam answer.
Middle Ear Mucosal Folds
MS ENT University Examination - 20 Marks
Introduction
The middle ear mucosa is essentially a mucus-secreting respiratory epithelium bearing cilia on its surface. This mucous membrane lines the bony walls of the tympanic cavity and extends to cover the ossicles and their supporting ligaments - analogous to the way the peritoneum covers the visceral organs in the abdomen. As the membrane drapes over the ossicular chain, tendons of the middle ear muscles, and ligamentous structures, it forms a series of mucosal folds that serve critical anatomical and functional roles.
These folds, when thickened, form true ligaments. Together they form the tympanic diaphragm (epitympanic diaphragm), which divides the middle ear into the superior epitympanum and the inferior mesotympanum/hypotympanum, and thereby govern middle ear ventilation, drainage, and by extension, the pathogenesis of several otological diseases.
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2; Cummings Otolaryngology, 7th ed.)
Classification of Middle Ear Mucosal Folds
Mucosal folds are classically described under two groups based on the ossicle they relate to.
A. Malleal Folds (5 folds)
-
Anterior malleal fold - runs from the neck of the malleus to the anterosuperior margin of the tympanic sulcus. It forms the anterior boundary of Prussak's space.
-
Posterior malleal fold - runs from the neck of the malleus to the posterosuperior margin of the tympanic sulcus. It forms the posterior boundary of Prussak's space and the posterior wall of the posterior pouch of von Troeltsch.
-
Lateral malleal fold (Shrapnell fold) - runs neck to neck in an arch form and attaches to the Shrapnell (pars flaccida) membrane. It forms the superior boundary of Prussak's space and is the key component of the tympanic diaphragm.
-
Anterior pouch of von Troeltsch - the recess between the anterior malleal fold and the portion of the tympanic membrane anterior to the handle of the malleus.
-
Posterior pouch of von Troeltsch - the recess between the posterior malleal fold and the portion of the tympanic membrane posterior to the handle of the malleus. This is the independent ventilation route for Prussak's space.
(K J Lee's Essential Otolaryngology, 12th ed.)
B. Incudal Folds (4 folds)
-
Lateral incudomalleal fold - arises from the posterior end of the short process of the incus, extends anteriorly between the incus body and the proximal long process, joins the head of the malleus, and projects inferiorly to align with the posterior and lateral malleal folds. It divides the lateral posterior epitympanum into the superior lateral attic (communicates with mastoid) and the inferior lateral attic (communicates directly with mesotympanum and has reliable ventilation).
-
Superior incudal fold - connects the superior surface of the incus body to the tegmen.
-
Posterior incudal ligament - attaches the short process of the incus to the fossa incudis posteriorly; it is an important component of the tympanic diaphragm.
-
Medial incudal fold - runs along the medial surface of the incus.
(Cummings Otolaryngology; from Proctor B: J Laryngol Otol 78:631-648, 1964)
C. Tensor Fold
The tensor fold is a membranous fold arising from the tensor tympani canal and cochleariform process. It is a particularly important fold because it separates the anterior epitympanic space (AES) from the supratubal recess (a superior and anterior extension of the mesotympanum near the Eustachian tube). Its significance is outlined below.
The Tympanic Diaphragm
The tympanic (epitympanic) diaphragm is composed of:
| Component | Description |
|---|---|
| Posterior incudal ligament | Anchors short process of incus |
| Lateral incudomalleal fold | Separates superior and inferior lateral attic |
| Lateral malleal fold | Key fold; superior boundary of Prussak's space |
| Lateral malleal ligament | |
| Anterior malleal fold | |
| Anterior malleal ligament | |
| Tensor fold (or posterior malleal fold) | Separates AES from supratubal recess |
| Tensor tympani tendon |
This diaphragm divides the middle ear into a superior epitympanum (above) and an inferior mesotympanum/hypotympanum (below). The only route for air exchange between the mesotympanum and epitympanum passes through the tympanic isthmus.
(K J Lee's Essential Otolaryngology; Cummings Otolaryngology)
The Tympanic Isthmus
The tympanic isthmus is a 2.5 mm opening in the tympanic diaphragm - the main and often sole conduit for ventilation of the epitympanum from the Eustachian tube.
It has two components:
-
Anterior tympanic isthmus (isthmus tympani anticus) - between the incudostapedial joint and the tensor tympani muscle tendon. This is the largest and most important ventilation route to the attic.
-
Posterior tympanic isthmus (isthmus tympani posticus) - posterior to the incudostapedial joint, between the stapedial muscle tendon, pyramidal eminence, and short process of the incus.
(K J Lee's Essential Otolaryngology; Cummings Otolaryngology, Fig. 126.10 - Proctor's partitioning diagram)
Diagrammatic depiction of the partitioning of the middle ear by ossicular chain and mucosal folds (Proctor, 1964 - reproduced in Cummings):
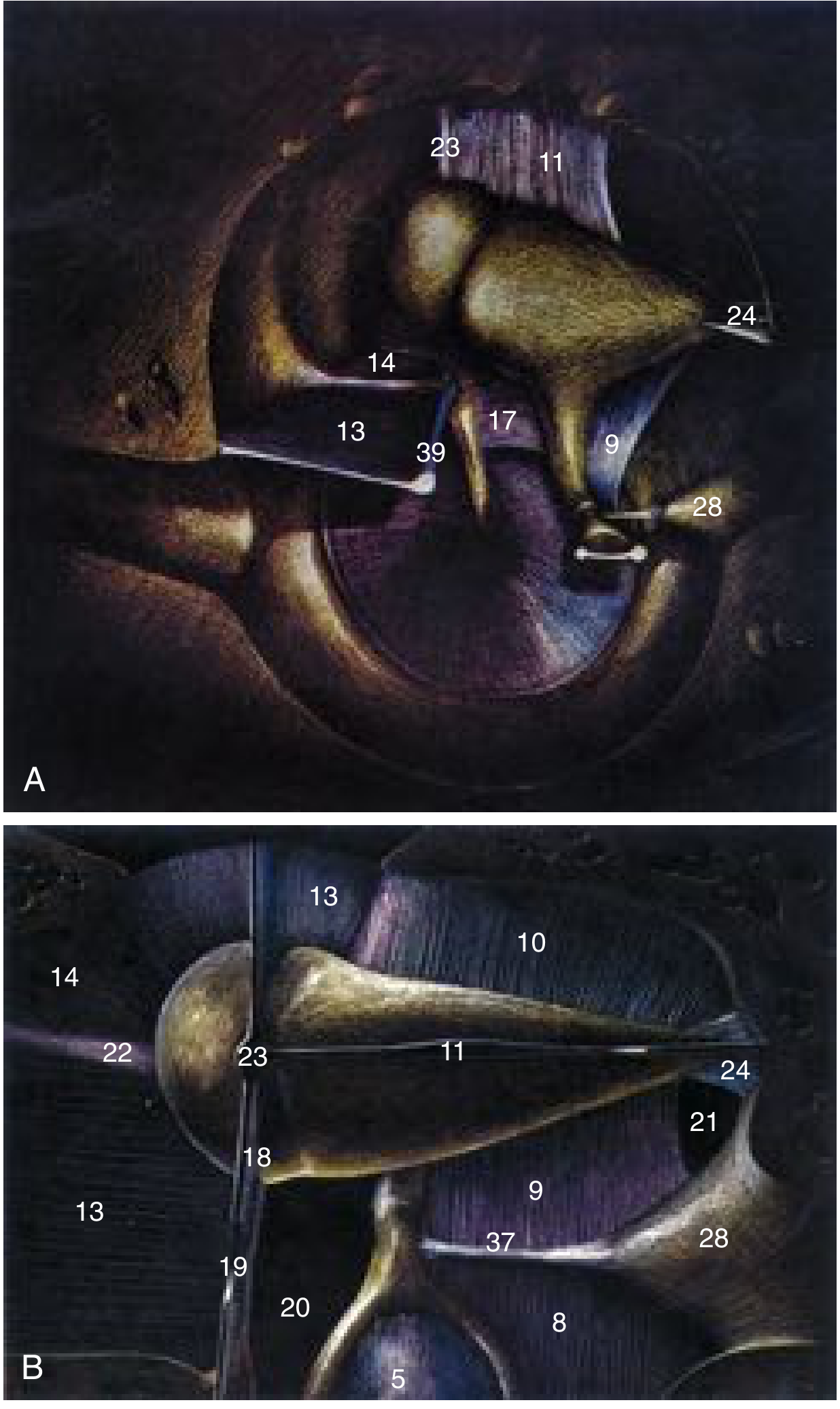
Numbers: (13) tensor fold, (17) interosseous fold, (9) medial incudal fold; (20) isthmus tympani anticus, (21) isthmus tympani posticus; (14) anterior malleolar fold, (18) superior malleolar fold; (22) anterior malleolar ligament, (23) superior malleolar ligament, (24) posterior incudal ligament.
Prussak's Space
Prussak's space is the most lateral compartment of the posterior epitympanum, and is of paramount clinical importance in the pathogenesis of attic cholesteatoma.
Boundaries
| Boundary | Structure |
|---|---|
| Superior | Lateral malleal fold (tympanic diaphragm) |
| Inferior | Lateral process (neck) of malleus |
| Medial | Head/neck of malleus |
| Lateral | Pars flaccida (Shrapnell's membrane) of TM |
| Anterior | Anterior malleal fold |
| Posterior | Posterior malleal fold |
Ventilation
Prussak's space has an independent, rough, narrow ventilation pathway through the posterior pouch of von Troeltsch. Thick and viscous secretions can block this pathway, causing sectorial dysventilation and retraction of the pars flaccida - the earliest event in development of attic cholesteatoma.
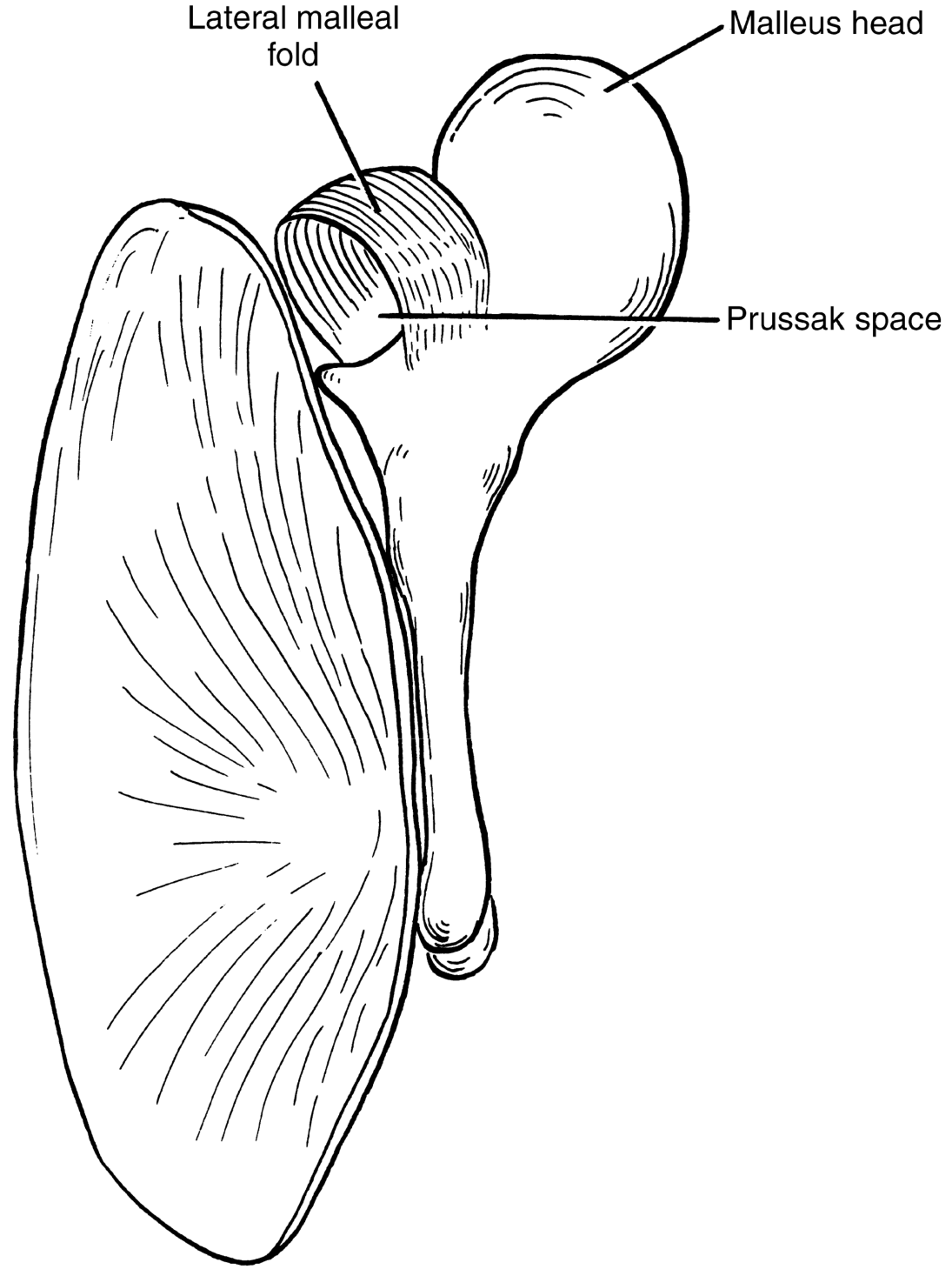
(K J Lee's Essential Otolaryngology, Fig. 13-7; Cummings Otolaryngology)
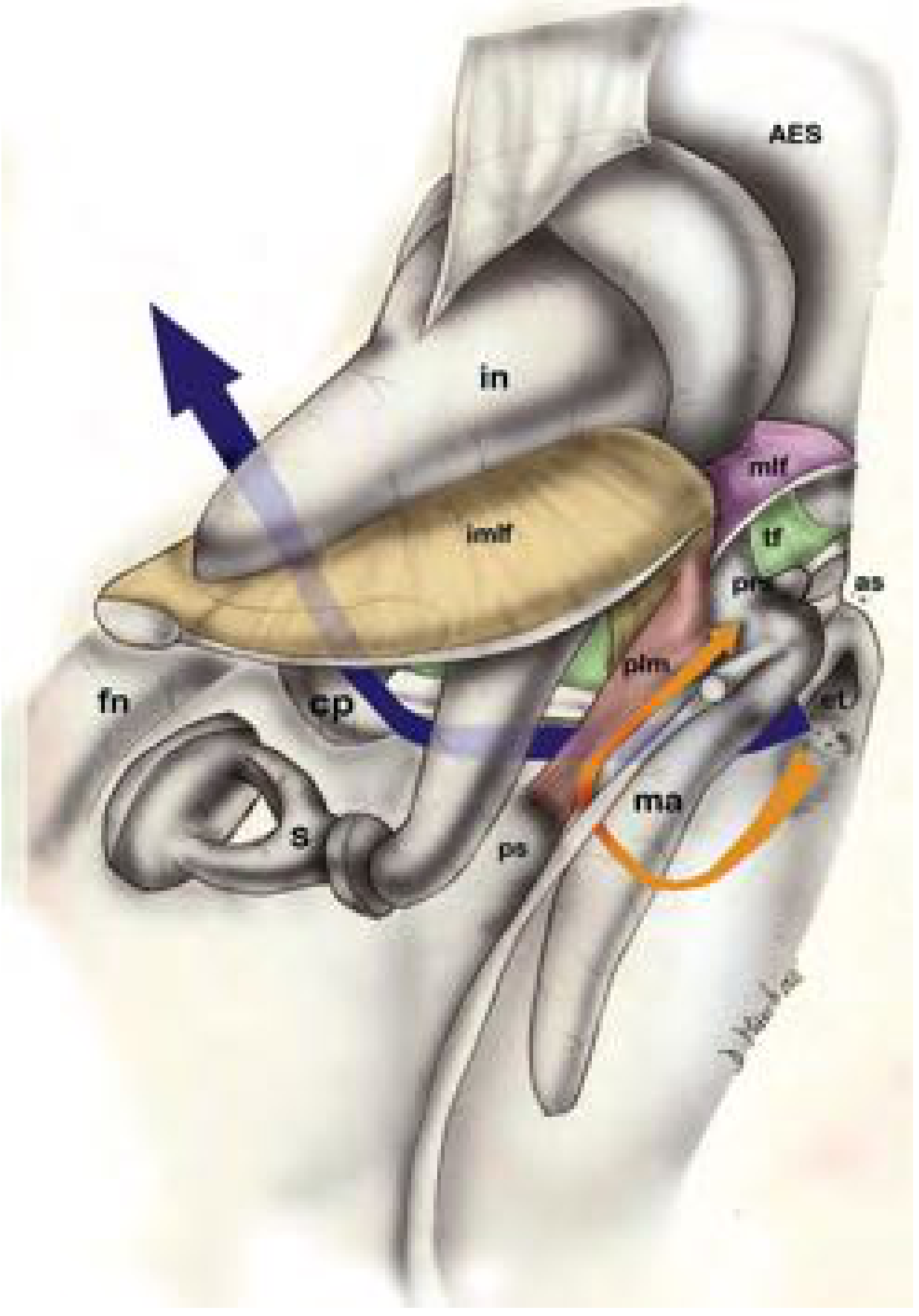
Epitympanic Diaphragm and Ventilation Pathways
The colored diagram below (Cummings, Fig. 144.3) shows the epitympanic diaphragm with key components:
- tf (yellow-green): tensor fold separating AES from supratubal recess
- imlf (tan): lateral incudomalleal fold
- mlf (purple): lateral malleal fold
- Blue arrow: main ventilation via tympanic isthmus into posterior epitympanum
- Orange arrow: ventilation of Prussak's space
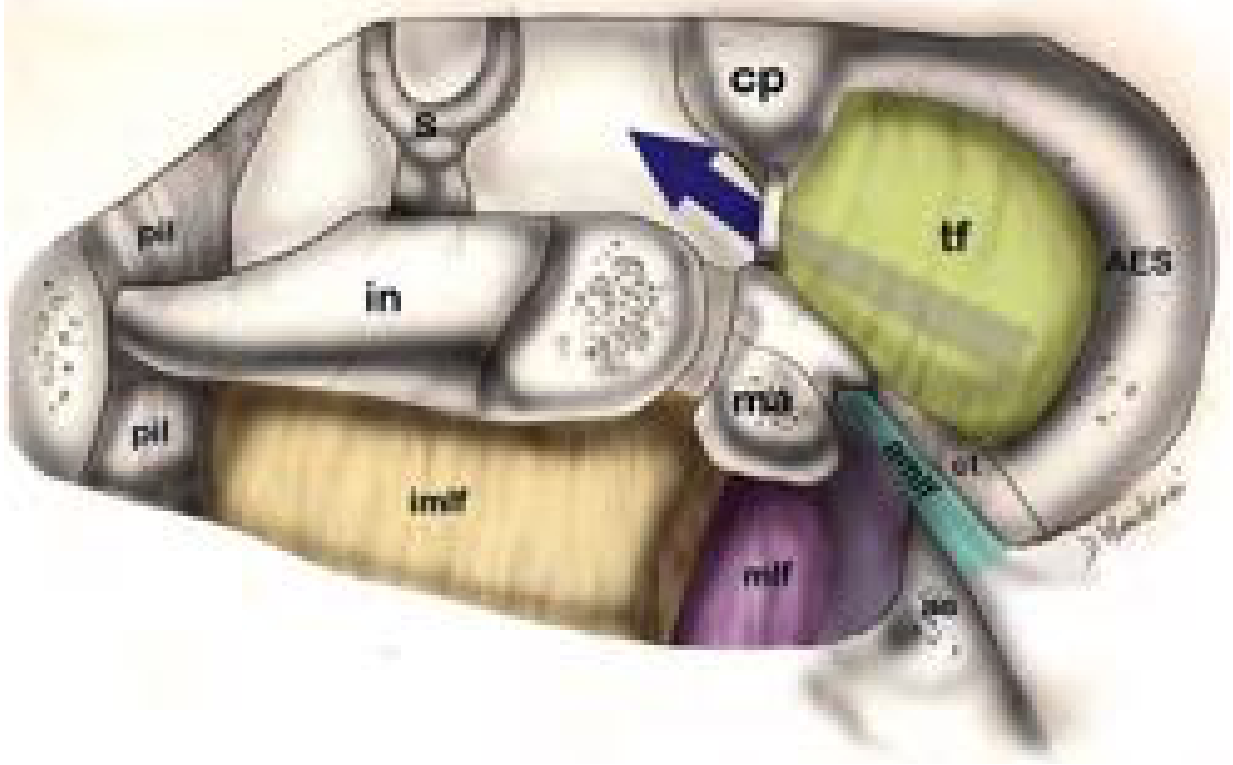
Two major ventilation pathways of the epitympanic compartments:
- Posterior pathway (blue arrow): ET → mesotympanum → tympanic isthmus → posterior epitympanum → mastoid
- Lateral pathway (orange arrow): into Prussak's space via posterior pouch of von Troeltsch
The Tensor Fold - Special Significance
The tensor fold is present as a complete fold in 73% of temporal bones (Palva et al.) and absent or incomplete in 27%. This variability has enormous clinical consequences:
- When tensor fold is complete (73%): The tympanic isthmus is the sole pathway for attic ventilation. Any obstruction of the isthmus completely cuts off ventilation to the anterior epitympanum.
- When tensor fold is incomplete/absent (27%): An alternate direct pathway exists from the mesotympanum to the anterior epitympanum, providing "fail-safe" ventilation.
- When tensor fold is oriented vertically: The supratubal recess is large and wide.
- When tensor fold is oriented horizontally: The supratubal recess is narrow and inferiorly displaced.
(Cummings Otolaryngology, 7th ed., Chapter 144)
Mucociliary Function of the Middle Ear Mucosa
Three distinct mucociliary pathways can be identified in the normal middle ear:
- Epitympanic pathway
- Promontorial pathway
- Hypotympanic pathway (the largest)
All three pathways coalesce at the tympanic orifice of the Eustachian tube. The mucosal folds also carry the blood supply to and from the ossicles and middle ear contents.
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, Chapter 46)
Clinical Significance
1. Cholesteatoma Pathogenesis
- Blockage of Prussak's space ventilation → negative pressure → retraction of pars flaccida → attic cholesteatoma
- Blockage of the tympanic isthmus (by inflammatory tissue, granulations, or disease) in the presence of a complete tensor fold → dysventilation of the anterior epitympanum and mastoid → cholesteatoma
2. Cholesteatoma Distribution
The mucosal folds create compartments in which cholesteatoma can be contained or hidden. The bony recesses (sinus tympani, facial recess, supratubal recess) harbored by these folds are frequent sites of residual cholesteatoma after surgery.
3. Surgical Implications
- During chronic ear surgery, it is recommended to:
- Widen the tympanic isthmus by removing inflammatory tissue, restoring ventilation
- Open a complete tensor fold to provide an alternate pathway for attic ventilation (anterior epitympanoplasty)
- The cog (bony septum dividing anterior and posterior epitympanum) is an important surgical landmark - anterior to the malleus head, used to orient dissection
4. Congenital and Inflammatory Defects
Congenital defects in the folds, or folds affected by inflammatory processes (mucosal disease or cholesteatoma), can block the narrow isthmus. This leads to loss of air from the epitympanum and provokes further inflammation in a self-perpetuating cycle.
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2; Cummings Otolaryngology, 7th ed.)
Summary Table
| Fold | Origin | Attachment | Key Role |
|---|---|---|---|
| Anterior malleal fold | Neck of malleus | Anterosuperior tympanic sulcus | Anterior boundary of Prussak's space |
| Posterior malleal fold | Neck of malleus | Posterosuperior tympanic sulcus | Posterior boundary of Prussak's space |
| Lateral malleal fold | Neck of malleus (arch) | Shrapnell membrane | Superior boundary of Prussak's space; key component of tympanic diaphragm |
| Tensor fold | Tensor tympani canal/cochleariform process | Lateral tympanic wall | Separates AES from supratubal recess; regulates attic ventilation |
| Lateral incudomalleal fold | Short process of incus | Malleus head/posterior malleal fold | Divides lateral posterior epitympanum into superior and inferior attic |
| Posterior incudal ligament | Short process of incus | Fossa incudis | Anchors incus; part of tympanic diaphragm |
Sources
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2 - "The Middle Ear Mucosal Folds," "The Mucosa of the Tympanic Cavity"
- Cummings Otolaryngology Head and Neck Surgery, 7th ed. - "Middle Ear Spaces," "Epitympanum" (Chapter 144), Proctor's partitioning diagram
- K J Lee's Essential Otolaryngology, 12th ed. - "Middle Ear Folds of Significance," "Epitympanum (Attic)"
- Proctor B. The development of the middle ear spaces and their surgical significance. J Laryngol Otol 78(7):631-648, 1964.
This is a shared conversation. Sign in to Orris to start your own chat.