Radiological feautre in acute osteomyelitis
Reading File
Finding Sources
Finding Sources
Searching Images
acute osteomyelitis radiology X-ray MRI bone
Searching PubMed
"osteomyelitis"[MeSH Terms] AND "diagnostic imaging"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have rich content from multiple authoritative sources. Here is the comprehensive answer:
Radiological Features of Acute Osteomyelitis
Key Principle: Imaging Lag
Plain radiographs lag behind the disease process and may appear normal for up to 2 weeks after onset. This is the single most important clinical point — a normal X-ray does not exclude acute osteomyelitis. — Grainger & Allison's Diagnostic Radiology
1. Plain Radiography (X-Ray) — First-Line, Low Sensitivity Early
Despite limitations, X-ray is always obtained first. Signs develop sequentially:
| Timeframe | Radiographic Finding |
|---|---|
| Days 1–3 | Deep soft-tissue swelling (obliteration of fat planes) |
| Days 3–7 | Periosteal reaction (elevation/layering) |
| Days 7–14 | Focal osteopenia / lytic lesion at metaphysis |
| >2 weeks | Cortical irregularity / frank bone destruction |
Specific signs:
- Soft-tissue swelling — earliest and most sensitive plain film sign; displacement of fat planes around the affected bone
- Periosteal reaction — linear or lamellar new bone formation along the cortex as the periosteum is lifted by subperiosteal pus
- Lucent metaphyseal lesion — focal osteolysis reflecting bone destruction and marrow necrosis
- Cortical irregularity — represents bony destruction from advancing infection
In neonates, X-rays may show abnormalities within days (faster bone turnover), while in older children and adults the lag is the full 10–14 days.
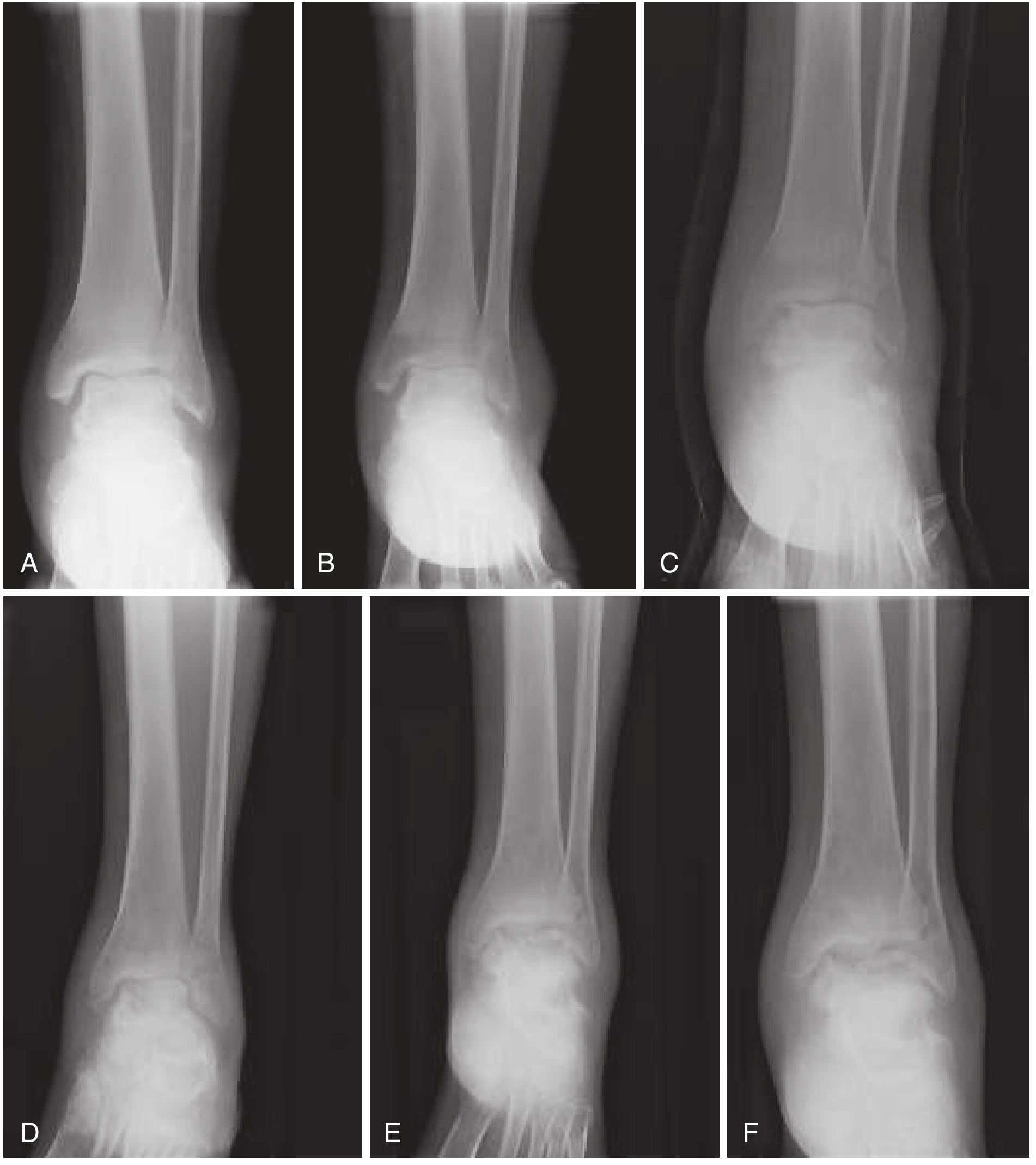
Radiographic progression of acute osteomyelitis: (A) soft tissue swelling → (B) effusion + joint space loss → (C–D) erosion and demineralization → (E–F) frank bone destruction. — Rosen's Emergency Medicine
2. Ultrasound (US) — Useful in Infants and Children
High-resolution US provides a rapid, non-invasive, radiation-free assessment:
- Detects subperiosteal fluid collections / abscesses early (even before bone changes on X-ray)
- Identifies periosteal elevation and soft-tissue edema
- Quantifies the fluid component and guides aspiration/drainage
- Most useful in infants where periosteum is loosely attached and subperiosteal abscesses are common
- Cannot assess intramedullary changes
3. MRI — Gold Standard (Highest Sensitivity and Specificity)
MRI is the investigation of choice when plain films are normal or equivocal.
Sequences and findings:
| Sequence | Finding |
|---|---|
| T1-weighted | Decreased signal in marrow (normal marrow fat replaced by edema/pus) |
| T2-weighted / STIR | Increased signal in bone marrow (edema) and surrounding soft tissues |
| Contrast-enhanced (fat-suppressed T1) | Enhancement of granulation tissue, defines abscess rim; soft-tissue abscess identified |
Characteristic MRI findings:
- Bone marrow edema — low T1, high T2/STIR signal in the metaphysis
- Subperiosteal abscess — fluid collection deep to periosteum, rim-enhancing
- Soft-tissue edema and abscess — hyperintense on T2, enhancing periphery with gadolinium
- Penumbra sign (in subacute infection) — peripheral high-signal ring of granulation tissue surrounding a low-signal abscess cavity on T1
- Sinus tracts — linear T2 high-signal tracks from medullary cavity to skin
Important caveat: On T2 sequences, reactive marrow edema can overestimate the extent of actual infection.
MRI also detects:
- Growth plate involvement (epiphyseal spread in infants)
- Multifocal disease
- Spinal complications (epidural abscess, cord compression)
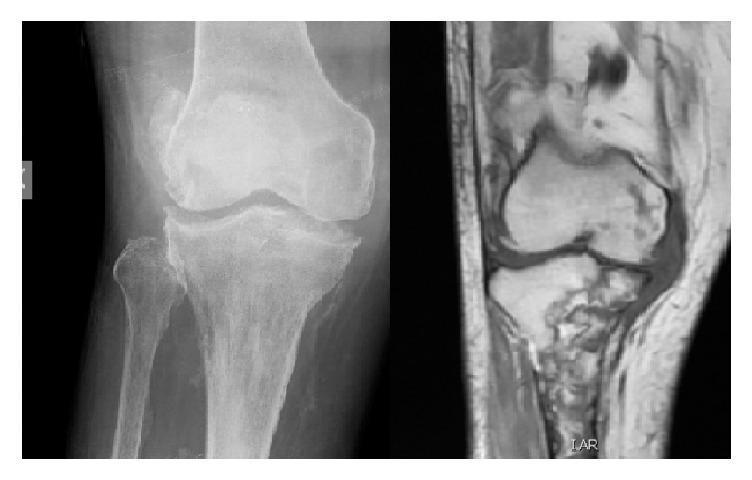
Comparison: X-ray (cortical changes, joint space loss) vs MRI (marrow edema, abscesses) in osteomyelitis.

X-ray vs STIR MRI comparison in native femoral osteomyelitis — note how MRI demonstrates far greater extent of marrow and soft-tissue involvement.
4. CT Scan
- Superior to X-ray for defining cortical destruction extent
- Detects sequestra (dense dead bone fragments) earlier than X-ray
- Useful for surgical planning and identifying gas in bone (gas-forming organisms)
- Limitation: radiation dose; inferior to MRI for soft tissue and marrow assessment
5. Bone Scintigraphy (99mTc-MDP)
- High sensitivity (>90%) — becomes positive within 24–72 hours of onset
- Three-phase technetium scan: increased uptake on all three phases (blood flow, blood pool, delayed)
- Useful when MRI is unavailable or contraindicated
- Useful for detecting multifocal disease (whole-body survey)
- Limitations: low specificity (any bone pathology gives uptake), false-negative in neonates (avascular ischemic bone may show "cold" lesion)
6. Age-Related Location and Imaging Implications
| Age Group | Vascular Anatomy | Typical Location | Imaging Implication |
|---|---|---|---|
| Neonates | Metaphyseal vessels cross growth plate | Metaphysis + epiphysis + joint | MRI if X-ray normal; multifocal in ~50% |
| Children | No epiphyseal supply | Metaphysis only | Classic metaphyseal lytic lesion |
| Adults | Growth plate closed — anastomoses reform | Metaphysis + epiphysis (subchondral) | Vertebral involvement common; MRI for discitis |
7. Imaging Algorithm Summary
Suspected Acute Osteomyelitis
│
Plain X-ray (always first)
│
┌─────┴─────┐
Normal Abnormal → treat/culture
│
MRI (investigation of choice)
├── Confirms diagnosis → treat
└── Equivocal / MRI unavailable
│
Bone scan OR US (infants)
Adapted from Rosen's Emergency Medicine diagnostic algorithm (Fig. 125.2)
Summary Table
| Modality | Sensitivity | Earliest Positive | Best For |
|---|---|---|---|
| Plain X-ray | Low early | 10–14 days | Cortical changes, periosteal reaction, screening |
| Ultrasound | Moderate | 1–2 days | Subperiosteal abscess in infants; guidance |
| MRI | Highest | 1–2 days | Early diagnosis, extent, soft tissue, abscess |
| CT | Moderate | 1–2 weeks | Cortical destruction, sequestra, surgical planning |
| Bone scan | High | 24–72 hours | Multifocal disease, MRI unavailable |
Sources: Grainger & Allison's Diagnostic Radiology; Robbins & Cotran Pathologic Basis of Disease; Rosen's Emergency Medicine; Goldman-Cecil Medicine
Recent evidence note: A 2026 systematic review (PMID 41574408) confirms plain radiography for diabetic foot osteomyelitis has significant limitations in both sensitivity and monitoring accuracy, reinforcing MRI as the preferred modality. A 2024 meta-analysis (PMID 39168784) demonstrates that diffusion-weighted and dynamic contrast MRI provide high diagnostic accuracy for osteomyelitis in diabetic foot — consistent with current textbook recommendations.
This is a shared conversation. Sign in to Orris to start your own chat.