Bilirubin metabolism pathway
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have rich, comprehensive content from multiple authoritative sources plus excellent diagrams. Let me compile the full answer.
Bilirubin Metabolism Pathway
Bilirubin is the major end product of heme catabolism, produced at a rate of approximately 250-350 mg/day in healthy adults. Its metabolism spans four anatomical compartments: the reticuloendothelial system, the circulation, the liver, and the intestine.
1. Heme Catabolism (Production Phase)
About 70-90% of bilirubin comes from the breakdown of hemoglobin in senescent red blood cells, with the remainder from myoglobin, cytochromes, and ineffective erythropoiesis.
The two-step enzymatic reaction occurs primarily in macrophages of the spleen (and liver Kupffer cells):
Step 1 - Heme oxygenase: Opens the porphyrin ring of heme using NADPH and O₂, releasing:
- Biliverdin (green linear tetrapyrrole)
- Carbon monoxide (CO) - transported as carboxyhemoglobin
- Fe³⁺ (recycled)
Step 2 - Biliverdin reductase: Reduces biliverdin to bilirubin using NADPH
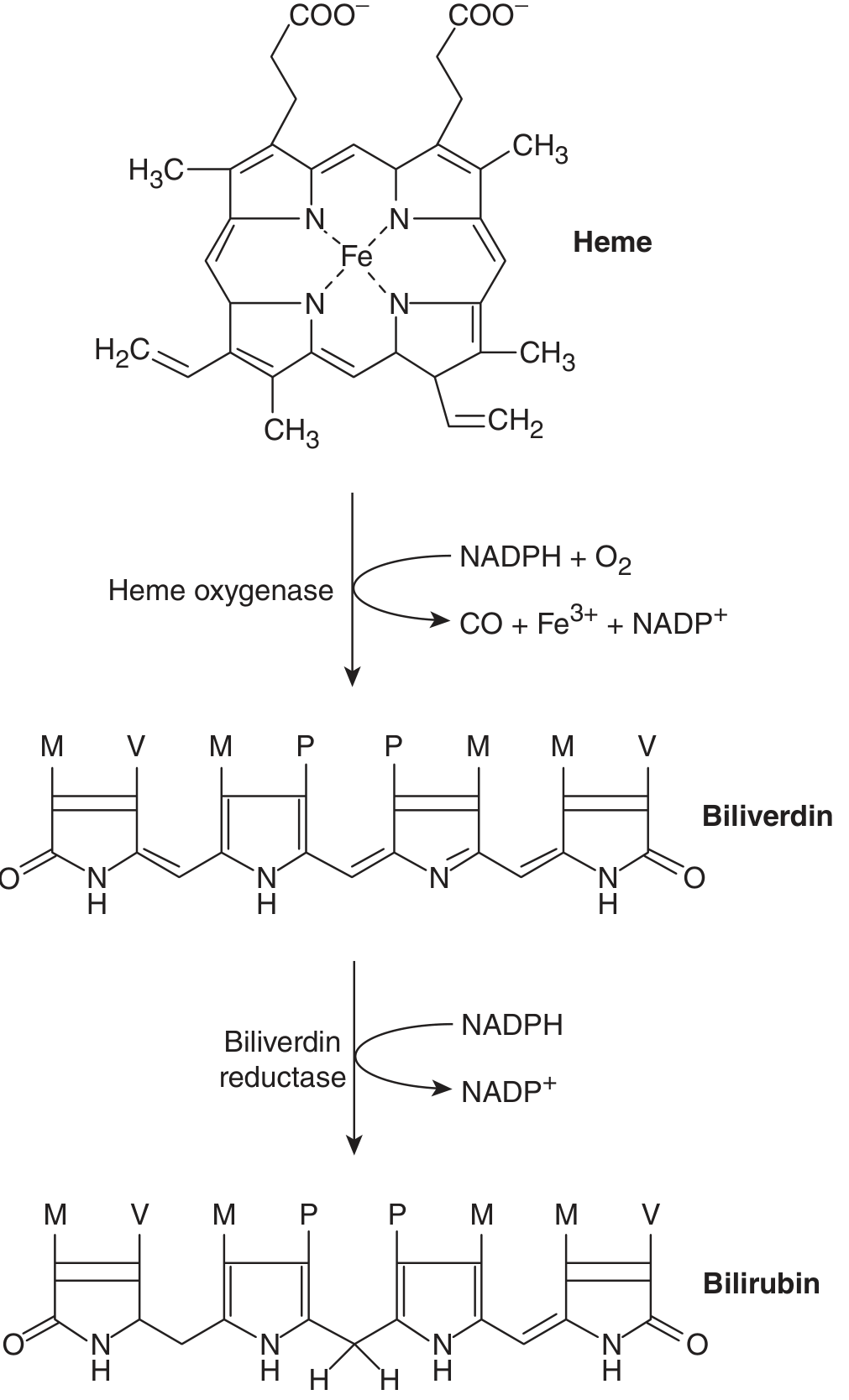
Heme → Biliverdin (heme oxygenase, NADPH+O₂) → Bilirubin (biliverdin reductase, NADPH) - Ganong's Review of Medical Physiology, 26th Ed.
The resulting bilirubin is in the unconjugated (indirect) form - highly lipid-soluble, water-insoluble, and potentially neurotoxic.
2. Transport in Plasma
Unconjugated bilirubin is insoluble in aqueous solutions and is therefore tightly bound to albumin for transport through the bloodstream to the liver. The albumin-bilirubin complex cannot be filtered by the kidney under normal conditions. The half-life of unconjugated bilirubin is only ~5 minutes, reflecting rapid hepatic uptake.
3. Hepatic Handling - Four Steps
Transfer from blood to bile involves four distinct, interrelated steps:
Step 3a - Uptake into Hepatocytes
Albumin-bound bilirubin reaches the hepatocyte surface through fenestrae in the sinusoidal endothelium and the Space of Disse. Bilirubin dissociates from albumin and enters hepatocytes via:
- OATP1B1 and OATP1B3 (organic anion transporting polypeptides) - the primary carrier-mediated transporters
- Some passive diffusion
Step 3b - Intracellular Binding
Inside the hepatocyte, free bilirubin is kept in solution by binding to cytoplasmic proteins - historically called Y and Z proteins, then ligandin, now identified as glutathione-S-transferases (GST). This prevents back-diffusion and shuttles bilirubin to the smooth endoplasmic reticulum (SER).
Step 3c - Conjugation (in SER)
In the SER, bilirubin undergoes glucuronidation catalyzed by UDP-glucuronosyltransferase (UGT1A1) encoded by the UGT1A1 gene on chromosome 2:
- Bilirubin + 2× UDPGA (uridine diphosphoglucuronic acid) → Bilirubin diglucuronide
- A smaller proportion forms bilirubin monoglucuronide
- Ratio of mono:di conjugate in bile ≈ 1:4; in plasma ≈ 1:1 (monoglucuronide refluxes more readily)
Conjugated bilirubin is now water-soluble and non-toxic.
Step 3d - Canalicular Secretion
Conjugated bilirubin is actively transported across the canalicular membrane into bile against a concentration gradient by MRP2 (multidrug resistance-associated protein 2 / ABCC2) via ATP-dependent transport.
- A small fraction of conjugated bilirubin is also transported back into portal circulation by MRP3, then reuptaken by OATP1B1/1B3 (enterohepatic-like cycling within the liver)
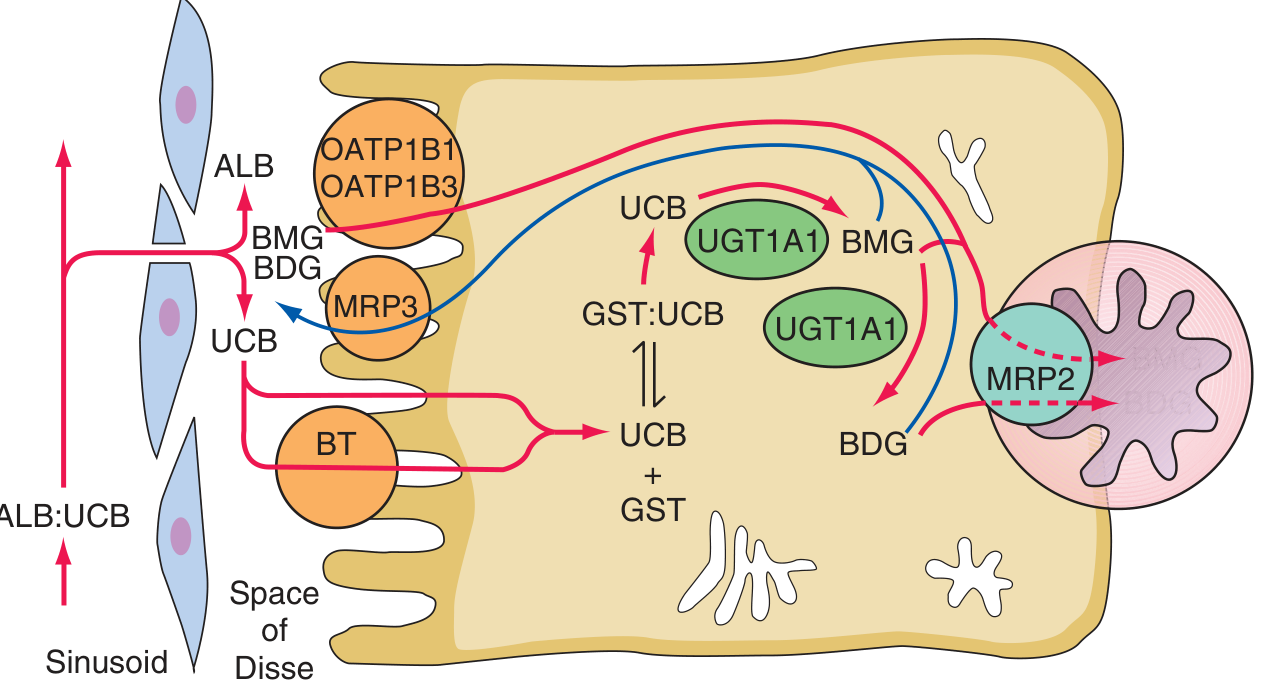
Hepatocellular bilirubin transport showing sinusoidal uptake (OATP1B1/1B3), intracellular GST binding, UGT1A1 conjugation, and MRP2-mediated canalicular secretion - Harrison's Principles of Internal Medicine, 22E
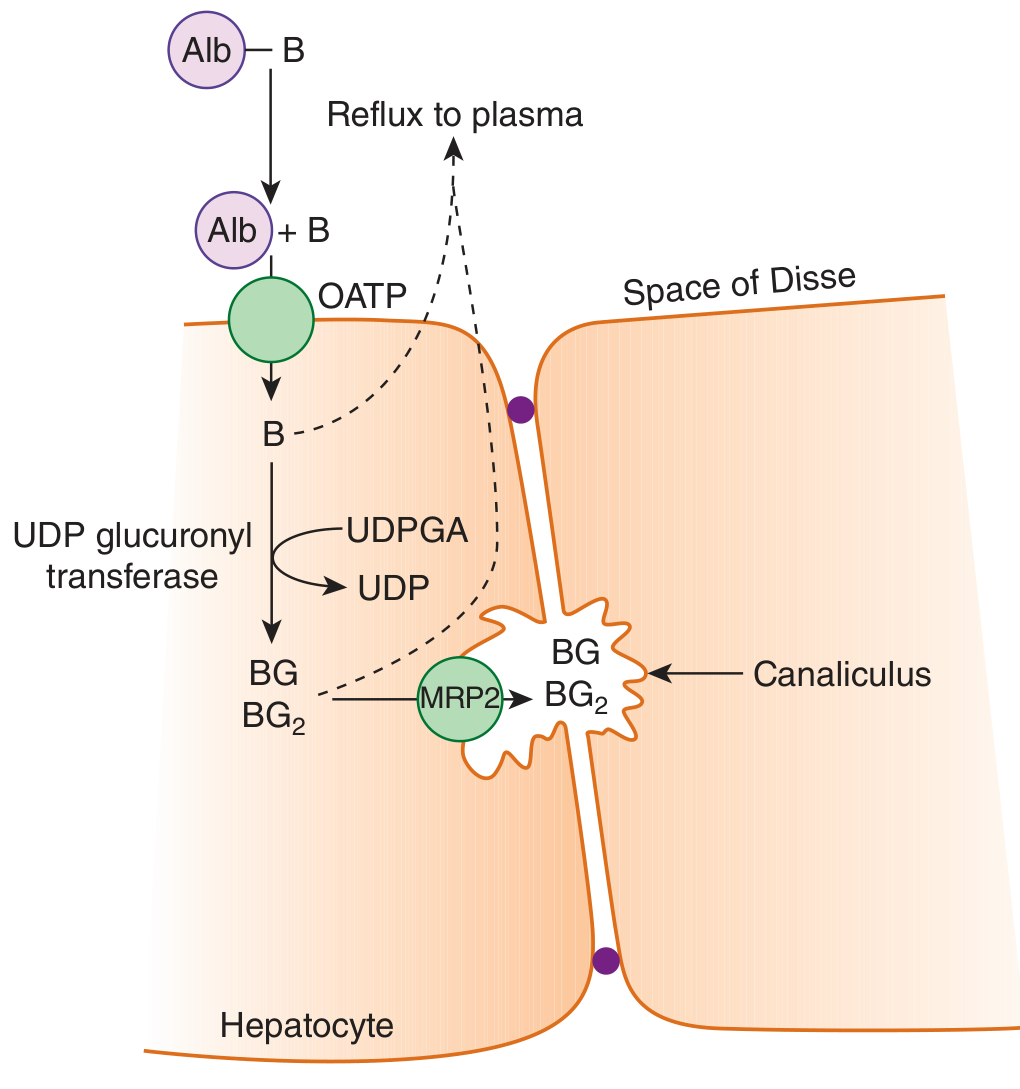
Albumin-bound bilirubin enters Space of Disse, taken up via OATP, conjugated to BG/BG₂ by UDP-glucuronyl transferase, secreted into canaliculus via MRP2 - Ganong's Review of Medical Physiology, 26th Ed.
4. Intestinal Phase and Enterohepatic Circulation
Once conjugated bilirubin enters the small intestine in bile:
- The small intestinal mucosa is relatively impermeable to conjugated bilirubin, so it passes largely unabsorbed to the colon
- In the colon, gut bacteria deconjugate bilirubin and further reduce it to a series of colorless compounds called urobilinogens (stercobilinogen, urobilinogen, mesobilinogen)
- Most urobilinogen (~80%) is oxidized to stercobilin and excreted in feces, giving stool its characteristic brown color
- A small amount (~20%) is reabsorbed into portal circulation:
- Most is re-excreted by the liver (enterohepatic circulation)
- A small fraction enters the systemic circulation and is filtered by the kidneys, excreted as urobilinogen in urine (gives urine its yellow color)
5. Delta-Bilirubin (δ-Bilirubin)
A clinically important concept: in the serum, a proportion of conjugated bilirubin covalently bonds with albumin, forming δ-bilirubin. It has the same half-life as albumin (~3 weeks), which explains why jaundice resolves slowly even after the underlying liver injury or biliary obstruction has resolved. The "direct bilirubin" assay actually measures δ-bilirubin + conjugated bilirubin + a small percentage of unconjugated bilirubin.
Summary Table
| Phase | Location | Key Molecules / Enzymes |
|---|---|---|
| Heme catabolism | Spleen/RES macrophages | Heme oxygenase, biliverdin reductase, NADPH |
| Plasma transport | Blood | Albumin (unconjugated bilirubin bound) |
| Hepatic uptake | Sinusoid → hepatocyte | OATP1B1, OATP1B3 |
| Intracellular storage | Hepatocyte cytoplasm | Glutathione-S-transferases (ligandins) |
| Conjugation | Smooth ER | UGT1A1, UDPGA |
| Canalicular secretion | Hepatocyte → bile | MRP2 (ABCC2), ATP-dependent |
| Intestinal conversion | Colon | Bacterial enzymes → urobilinogens |
| Enterohepatic cycling | Portal blood → liver | Liver re-excretion or urinary excretion |
Clinical Correlations
| Condition | Defect | Bilirubin type elevated |
|---|---|---|
| Hemolytic anemia | Excess production exceeds hepatic uptake | Unconjugated |
| Gilbert syndrome | Reduced UGT1A1 activity (~30%) + uptake defect | Unconjugated |
| Crigler-Najjar I | Complete UGT1A1 absence | Unconjugated (severe, kernicterus) |
| Crigler-Najjar II | Partial UGT1A1 deficiency | Unconjugated (milder) |
| Dubin-Johnson syndrome | MRP2 (canalicular transport) defect | Conjugated |
| Rotor syndrome | Sinusoidal reuptake defect (OATP) | Conjugated |
| Biliary obstruction | Impaired bile flow | Conjugated |
| Hepatocellular disease | Mixed (impaired conjugation + secretion) | Mixed |
- Harrison's Principles of Internal Medicine, 22E, Chapter 349
- Ganong's Review of Medical Physiology, 26th Ed., Chapter 28
- Henry's Clinical Diagnosis and Management by Laboratory Methods, Chapter 22
- Yamada's Textbook of Gastroenterology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.