Hypertension classification
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "classification"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compose the full, well-structured answer.
Hypertension Classification
Why Classification is Inherently Arbitrary
Blood pressure (BP) follows an approximately normal distribution in the general population, shifting left in younger people and right in older individuals and those with CKD. The relationship between BP and cardiovascular (CV) risk is continuous with no threshold - death from heart disease and stroke increases progressively from as low as 115/75 mmHg upward across all age groups. Any numerical cut-off is therefore a clinical convenience, not a biological boundary. The Global Burden of Disease study identified systolic BP (SBP) between 110 and 115 mmHg as the "theoretical minimum risk level." - Comprehensive Clinical Nephrology, 7th Edition
1. ACC/AHA 2017 Classification (USA - Current Standard)
The most influential modern classification. Lowered the hypertension threshold from 140/90 to 130/80 mmHg based on SPRINT trial data and network meta-analyses.
| Category | SBP (mmHg) | DBP (mmHg) | |
|---|---|---|---|
| Normal | < 120 | and | < 80 |
| Elevated | 120–129 | and | < 80 |
| Hypertension Stage 1 | 130–139 | or | 80–89 |
| Hypertension Stage 2 | ≥ 140 | or | ≥ 90 |
- Individuals with SBP and DBP in two different categories are assigned to the higher category.
- Diagnosis requires an average of ≥2 readings on ≥2 occasions, usually separated by ≥1 week.
- The "elevated BP" category replaced the JNC 7 term "prehypertension."
- Fuster and Hurst's The Heart, 15th Edition; Comprehensive Clinical Nephrology, 7th Edition
2. JNC 7 Classification (Historical - USA, 2003)
Still referenced widely, particularly in older literature and some international guidelines.
| Classification | SBP (mmHg) | DBP (mmHg) | |
|---|---|---|---|
| Normal | < 120 | and | < 80 |
| Prehypertension | 120–139 | or | 80–89 |
| Stage 1 Hypertension | 140–159 | or | 90–99 |
| Stage 2 Hypertension | ≥ 160 | or | ≥ 100 |
The term prehypertension was introduced here to indicate elevated CV risk and the need for lifestyle modification, even without a drug treatment threshold.
3. ESC/ESH 2018 Classification (European)
Uses a broader grading system that separates office BP classification from the diagnostic threshold for hypertension, and incorporates ambulatory and home BP thresholds.
| Office BP Classification | SBP (mmHg) | DBP (mmHg) |
|---|---|---|
| Optimal | < 120 | and < 80 |
| Normal | 120–129 | and/or 80–84 |
| High Normal | 130–139 | and/or 85–89 |
| Grade 1 Hypertension | 140–159 | and/or 90–99 |
| Grade 2 Hypertension | 160–179 | and/or 100–109 |
| Grade 3 Hypertension | ≥ 180 | and/or ≥ 110 |
| Isolated Systolic Hypertension | ≥ 140 | and < 90 |
Diagnostic thresholds for hypertension:
- Office BP: SBP ≥ 140 and/or DBP ≥ 90 mmHg
- 24-hour ambulatory BP (ABPM): ≥ 130/80 mmHg
- Daytime (awake) ABPM: ≥ 135/85 mmHg
- Nighttime (asleep) ABPM: ≥ 120/70 mmHg
- Home BP monitoring (HBPM): ≥ 135/85 mmHg
- Comprehensive Clinical Nephrology, 7th Edition (citing Williams et al., 2018 ESC/ESH guidelines)
4. ISH 2020 Classification (International Society of Hypertension)
Designed for global use, especially in low- and middle-income countries where ABPM may be unavailable.
| Category | SBP (mmHg) | DBP (mmHg) |
|---|---|---|
| Normal | < 130 | and < 85 |
| High Normal | 130–139 | and/or 85–89 |
| Grade 1 Hypertension | 140–159 | and/or 90–99 |
| Grade 2 Hypertension | ≥ 160 | and/or ≥ 100 |
- Comprehensive Clinical Nephrology, 7th Edition (citing Unger et al., 2020 ISH guidelines)
5. Classification by Cause (Etiology)
| Type | Prevalence | Notes |
|---|---|---|
| Primary (Essential) Hypertension | ~90–95% of cases | No identifiable cause; multifactorial |
| Secondary Hypertension | ~5–10% | Identifiable underlying cause (listed below) |
Common causes of secondary hypertension (in descending order of prevalence):
- Chronic kidney disease / renal parenchymal disease
- Renovascular disease (renal artery stenosis)
- Primary aldosteronism
- Obstructive sleep apnea
- Drug-induced (NSAIDs, OCPs, decongestants, stimulants, steroids)
- Pheochromocytoma
- Cushing's syndrome
- Coarctation of the aorta
- Thyroid disease (hypo- or hyperthyroidism)
- Comprehensive Clinical Nephrology, 7th Edition
6. Pediatric Classification (ACC/AHA 2017 / AAP 2017)
BP in children is classified by age-adjusted percentiles until age 12, then by fixed thresholds from age 13.
Children 1–12 years:
| Category | Threshold |
|---|---|
| Normal | < 90th percentile |
| Elevated | ≥ 90th percentile or ≥ 120/80 mmHg to < 95th percentile |
| Hypertension Stage 1 | ≥ 95th percentile to < 95th percentile + 12 mmHg, or 130/80 to 139/89 |
| Hypertension Stage 2 | ≥ 95th percentile + 12 mmHg, or ≥ 140/90 mmHg |
Children ≥ 13 years: Same thresholds as adults.
- Fuster and Hurst's The Heart, 15th Edition
7. Special Subtypes and Definitions
| Subtype | Definition |
|---|---|
| White Coat Hypertension | Elevated BP in clinical setting; normal on ABPM/HBPM. Prevalence ~15–30% of hypertensives. |
| Masked Hypertension | Normal BP in clinic; elevated on ABPM/HBPM. Higher true CV risk than white coat HTN. |
| Isolated Systolic Hypertension (ISH) | SBP ≥ 140 mmHg with DBP < 90 mmHg. Common in the elderly due to arterial stiffness. |
| Isolated Diastolic Hypertension | Elevated DBP with normal SBP. More common in younger adults. |
| Resistant Hypertension | BP remains ≥ 130/80 mmHg despite use of ≥3 antihypertensive agents (including a diuretic) at optimal doses. |
| Pseudoresistant Hypertension | Apparent resistance due to white coat effect, medication non-adherence, or inaccurate measurement. |
| Refractory Hypertension | Uncontrolled BP despite ≥5 antihypertensive agents including long-acting thiazide diuretic and mineralocorticoid receptor antagonist. |
- Fuster and Hurst's The Heart, 15th Edition; Comprehensive Clinical Nephrology, 7th Edition
8. Hypertensive Crises
When BP is severely elevated (typically > 180/120 mmHg):
| Term | Definition |
|---|---|
| Hypertensive Urgency | Severely elevated BP without evidence of acute target organ damage. Patient is typically asymptomatic. |
| Hypertensive Emergency | Severely elevated BP with acute or worsening target organ damage. |
Target organ damage in hypertensive emergencies:
- Acute myocardial ischemia or infarction
- Intracranial hemorrhage
- Pulmonary edema / heart failure
- Acute kidney injury
- Hypertensive encephalopathy
- Ischemic stroke
- Aortic dissection
Triggers: Clonidine withdrawal, pain, sympathomimetics (cocaine, amphetamines), pheochromocytoma, preeclampsia/eclampsia. Hypertensive emergencies account for about 0.6% of adult emergency department visits.
- Fuster and Hurst's The Heart, 15th Edition
9. ASH Working Group Staging (Risk-Integrated Approach)
The American Society of Hypertension proposed a staging system that integrates BP elevation, CV risk factors, biomarkers, and target organ damage rather than relying on BP numbers alone:
| Stage | BP Elevation | CV Risk Factors | Target Organ Disease |
|---|---|---|---|
| Normal | Normal/rare | None or few | None |
| Stage 1 | Occasional/intermittent | Several | None |
| Stage 2 | Sustained | Many | Early signs present |
| Stage 3 | Marked and sustained | Many | Overt, with or without CV events |
- Comprehensive Clinical Nephrology, 7th Edition (citing Giles et al., 2009)
Cardiovascular Risk Context
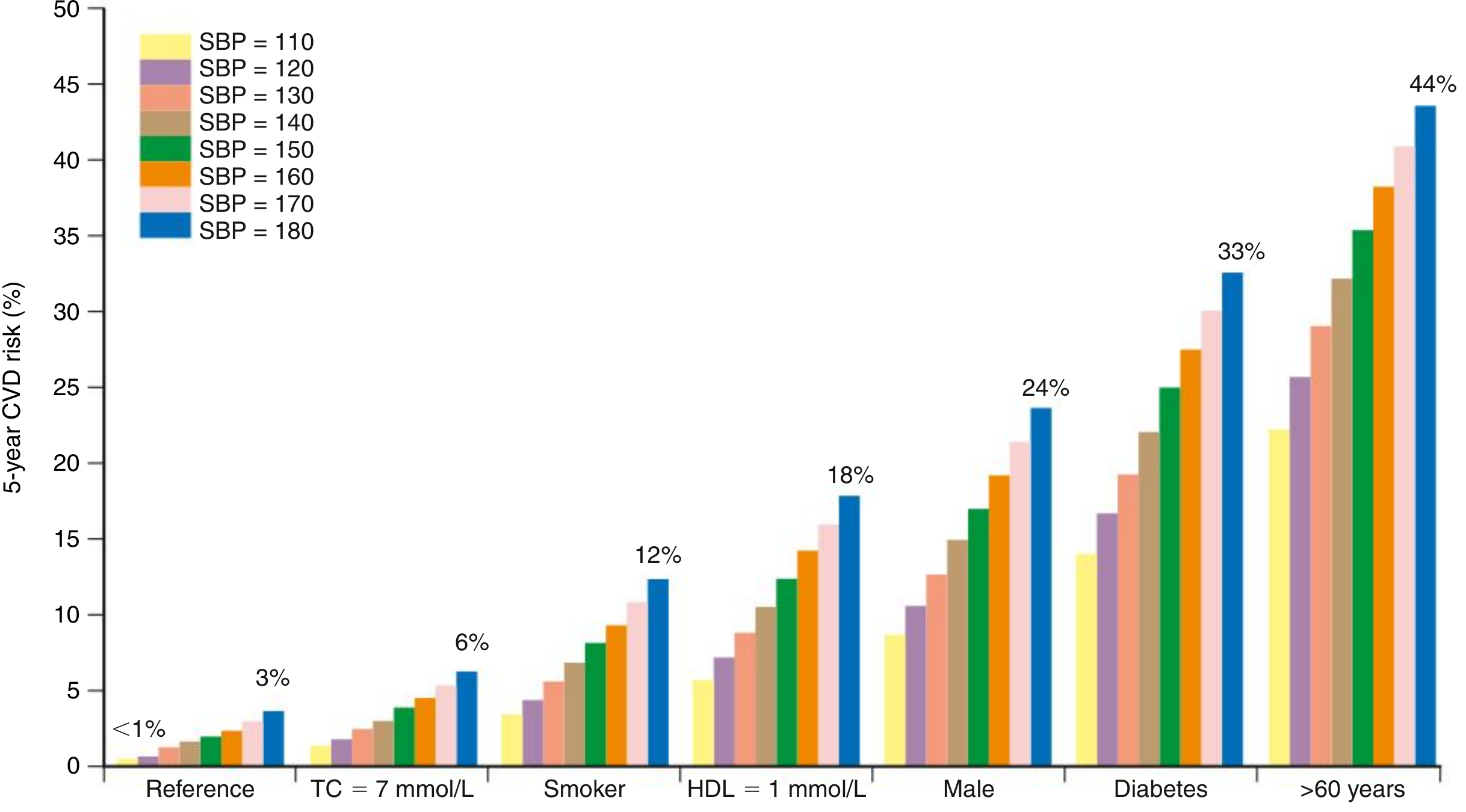
Fig: 5-year CVD risk by SBP level and associated risk factors. A person over 60 years with SBP of 180 mmHg carries a 44% 5-year CVD risk. Diabetes and age dramatically amplify the risk at any given BP level. - Comprehensive Clinical Nephrology, 7th Edition
Guideline Comparison at a Glance
| Normal | Pre/High Normal | HTN threshold | |
|---|---|---|---|
| JNC 7 | < 120/80 | 120–139/80–89 (Prehypertension) | ≥ 140/90 |
| ACC/AHA 2017 | < 120/80 | 120–129/< 80 (Elevated) | ≥ 130/80 |
| ESC/ESH 2018 | < 120/80 | 120–139/80–89 (Normal/High Normal) | ≥ 140/90 |
| ISH 2020 | < 130/85 | 130–139/85–89 (High Normal) | ≥ 140/90 |
The key divergence is the ACC/AHA 2017 lowering the hypertension threshold to 130/80 mmHg - a change that increased the prevalence of hypertension in US adults from ~32% (JNC 7) to ~46% but reduced the proportion recommended pharmacotherapy (since lifestyle modification alone is often adequate at Stage 1).
This is a shared conversation. Sign in to Orris to start your own chat.