Approach to Arthritis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from both sources. Let me compile the full, structured response.
Approach to Arthritis
1. Definition and Epidemiology
Arthritis encompasses a broad group of conditions causing joint inflammation, pain, and dysfunction. It affects more than 20% of adults in the United States and is a leading cause of disability worldwide. Patients may present acutely or chronically with primary joint pain, systemic complications, or medication-related side effects.
2. Pathophysiology
Arthritis primarily affects synovial (diarthrotic) joints, which consist of:
- Two subchondral bone ends covered with articular cartilage
- A fibrous joint capsule lined by the synovial membrane
- Synovial fluid - a viscous lubricant allowing near-frictionless motion
Damage to any of these structures - via inflammation, infection, crystals, or degeneration - leads to the spectrum of arthritic conditions.
3. Broad Classification
Three broad categories guide the initial differential:
| Category | Examples |
|---|---|
| Degenerative / OA | Primary OA, post-traumatic arthritis |
| Infectious / Septic | Bacterial, gonococcal, tuberculous arthritis |
| Inflammatory | RA, gout, pseudogout, PsA, reactive arthritis, SLE, SpA |
4. Step 1 - History
The "seven dimensions" of history are essential (Kelley's Rheumatology):
Key Clinical Factors to Assess (Rosen's Emergency Medicine, Box 102.1)
- Age of the patient
- Number of joints involved (mono- vs oligo- vs polyarticular)
- Time course: Acute (<7 days) | Subacute (7 days - 3 weeks) | Chronic (>3 weeks)
- Trauma history
- Systemic symptoms (fever, fatigue, rash, eye changes, GI symptoms)
- Aggravating/alleviating factors
- Medication history (many drugs cause arthralgia)
Mono vs. Polyarthritis - Clinical Significance
- Monoarthritis - must urgently exclude septic arthritis; a delay causes irreversible joint destruction and death
- Polyarthritis - widens the differential toward systemic rheumatologic disease; rarely infectious
Characteristic Historical Clues
| Feature | Inflammatory Arthritis | Osteoarthritis | Septic Arthritis |
|---|---|---|---|
| Morning stiffness | >1 hour | <30 minutes (gel phenomenon) | Variable |
| Effect of movement | Pain improves | Pain worsens | Severely limited |
| Onset | Weeks to months (RA) | Slow, over years | Rapid (hours to days) |
| Systemic symptoms | Common (fever, fatigue) | Absent | Fever (often absent!) |
| Age of onset | Any age | Typically >50 | Any age |
5. Step 2 - Physical Examination
General Examination
- Vital signs - fever/tachycardia (note: most septic arthritis patients are afebrile on presentation)
- Gait and posture
- Skin: psoriasis/nail pitting (PsA), butterfly rash (SLE), tophi (gout), skin breaks (septic)
- Eyes: uveitis (SpA, reactive arthritis)
- Mucous membranes: oral ulcers (SLE, Behçet's, reactive arthritis)
- Lymph nodes, salivary glands, thyroid
- Spine: axial involvement (SpA, OA)
Joint Examination (systematic approach)
- Inspection - swelling, deformity, erythema, muscle wasting
- Palpation - warmth, tenderness, effusion
- Range of motion (active and passive)
- Neurovascular assessment
- Special tests per joint
Joint Findings Differentiating Conditions
| Finding | Suggests |
|---|---|
| Hot, red, swollen single joint | Septic arthritis or crystal arthropathy |
| Symmetric small joint swelling (MCP, PIP) | Rheumatoid Arthritis |
| Asymmetric DIP involvement + nail pitting | Psoriatic Arthritis |
| Podagra (1st MTP) | Gout |
| Cool, hard bony enlargement | Osteoarthritis (Heberden's/Bouchard's nodes) |
| Dactylitis ("sausage finger") | PsA, reactive arthritis |
| Enthesitis | Spondyloarthropathy |
| Deep proximal muscle tenderness + high ESR age >50 | Polymyalgia rheumatica |
6. RA vs. OA Comparison
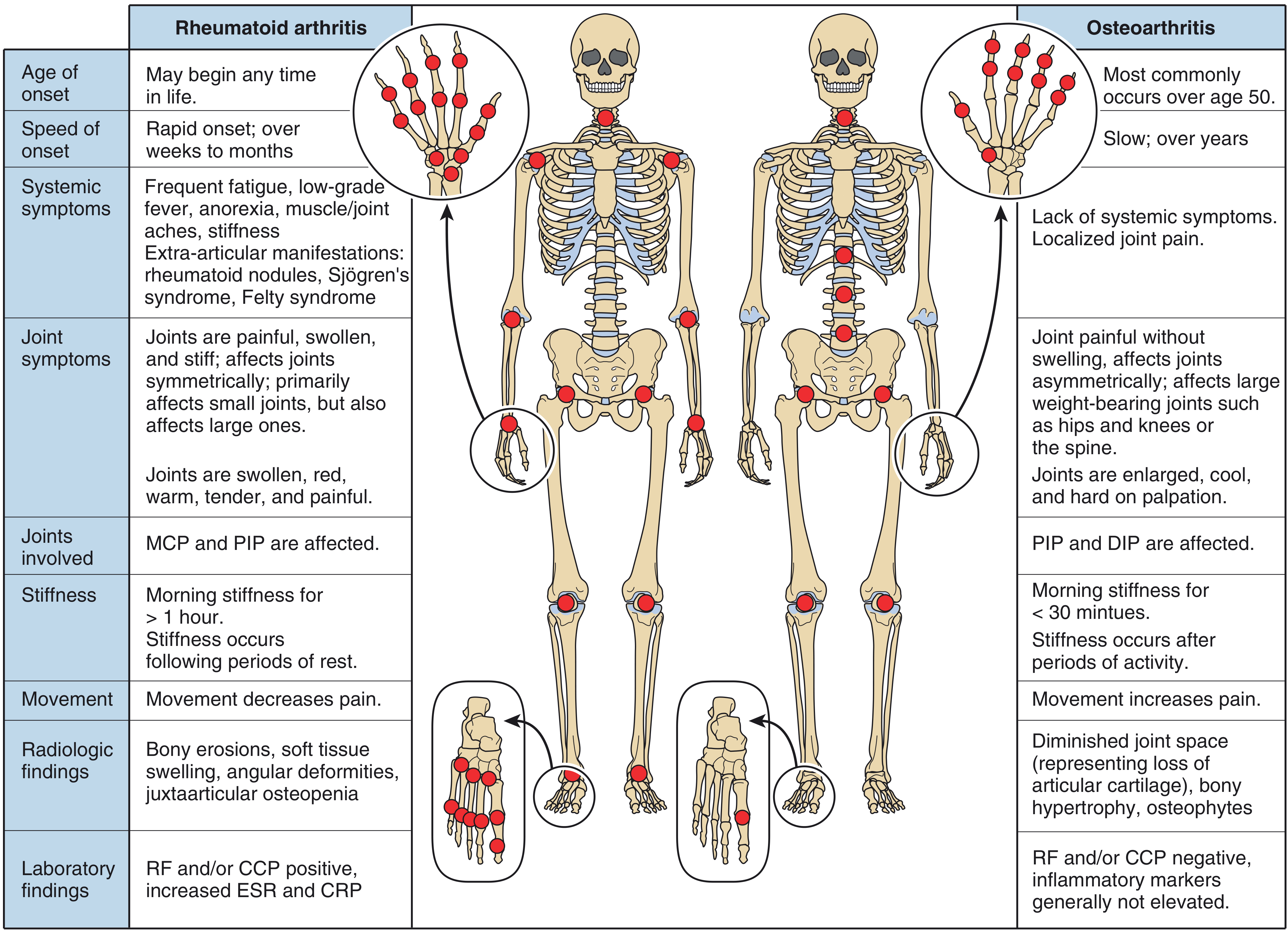
7. Joint Distribution Patterns
| Rheumatoid Arthritis | Osteoarthritis | Psoriatic Arthritis | Gout/Pseudogout | |
|---|---|---|---|---|
| Large joints | Knees, ankles, wrists (symmetric) | Hips, knees, ankles | Knees, ankles (asymmetric) | Knees, ankles |
| Small joints | MCP, PIP (hands); MTP (feet) - symmetric | DIP, PIP, 1st CMC (hands); 1st MTP (feet) | DIP + nails (asymmetric) | MTP (gout); MCP (pseudogout) |
| Spine | Cervical | Cervical + LS | LS spine + SI joints | No |
(Firestein & Kelley's Textbook of Rheumatology, Table 42.1)
8. Step 3 - Laboratory Investigation
Targeted (not "routine") - guided by differential:
| Test | When to Order | Interpretation |
|---|---|---|
| CBC | Suspected infection or systemic disease | Leukocytosis in septic/inflammatory |
| ESR / CRP | Inflammatory vs non-inflammatory | Elevated in RA, infection, PMR |
| Serum uric acid | Suspected gout | Often normal during acute attack - do NOT use to rule out gout |
| RF / anti-CCP | Suspected RA | Anti-CCP more specific (positive in ~70%) |
| ANA / dsDNA | Suspected SLE | ANA high sensitivity, low specificity |
| HLA-B27 | Suspected SpA | Supports (not diagnostic of) ankylosing spondylitis |
| Blood cultures | Suspected septic arthritis | Before antibiotics |
| Glucose, LFTs | Drug side effects, metabolic assessment | Background screening |
9. Step 4 - Synovial Fluid Analysis (Arthrocentesis)
Joint aspiration is mandatory in any acute monoarthritis to rule out septic arthritis. There is no reliable clinical finding that can safely exclude a septic joint without fluid analysis.
Synovial Fluid Classification
| Parameter | Normal | Non-inflammatory (OA) | Inflammatory (RA, gout) | Septic |
|---|---|---|---|---|
| Appearance | Clear, straw | Yellow, clear | Yellow, turbid | Turbid/purulent |
| WBC (cells/mm³) | <200 | 200-2,000 | 5,000-50,000 | >50,000 |
| PMNs | <25% | <25% | >50% | >75% |
| Glucose | Normal | Normal | Low (slight) | Very low |
| Culture | Negative | Negative | Negative | Positive |
| Crystals | None | None | Present (gout: MSU; pseudogout: CPPD) | None |
- Monosodium urate (MSU) crystals in gout: needle-shaped, negatively birefringent
- Calcium pyrophosphate (CPPD) in pseudogout: rhomboid, positively birefringent
- Hemarthrosis (bloody fluid): suggests trauma, pigmented villonodular synovitis, or coagulopathy
Arthrocentesis Sites (Rosen's Emergency Medicine)
| Joint | Needle Entry Point |
|---|---|
| Knee | Lateral to superior half of patella |
| Shoulder | Inferior to posterolateral edge of acromion |
| Elbow | "Soft spot" between lateral epicondyle and radial head |
| Ankle | Between tibialis anterior tendon and medial malleolus |
| Wrist | Ulnar to EPL tendon, distal to Lister's tubercle |
| MTP (1st) | Dorsal, medial to extensor tendon |
10. Step 5 - Imaging
Plain Radiographs - Diagnostic Clues
| Finding | Disease Suggested |
|---|---|
| Juxta-articular osteopenia | Early RA |
| Joint-space narrowing | RA, PsA, OA |
| Bony erosions | RA, PsA, chronic gout |
| Osteophytes / bony sclerosis | OA |
| Soft tissue calcification / chondrocalcinosis | CPPD (pseudogout) |
| Periosteal new bone formation | PsA |
(Firestein & Kelley's Textbook of Rheumatology, Table 42.3)
- CT scan: better for fractures, osteomyelitis, bone disease
- MRI: superior for early synovitis, cartilage, tendon/ligament pathology, sacroiliitis
- Ultrasound: bedside effusion detection, guides arthrocentesis, detects early synovitis and erosions
11. Approach Summary Algorithm
Acute Joint Pain
│
▼
Number of Joints?
┌─────┴─────────────┐
Mono/Oligo Polyarticular
│ │
▼ ▼
Arthrocentesis Symmetric?
MANDATORY ┌────┴────┐
│ Yes No
▼ │ │
Fluid analysis RA, PsA, ReA,
- WBC count Viral Gout, AS
- Crystals
- Culture
│
▼
WBC >50,000 or
positive culture?
│
Yes → Septic Arthritis (IV antibiotics + urgent washout)
No → Crystal? (gout/pseudogout) or Inflammatory (RA, etc.)
12. Key Points / Pitfalls
- Septic arthritis is the #1 must-not-miss diagnosis in acute monoarthritis - do not delay aspiration based on clinical grounds alone
- Serum uric acid is unreliable during acute gout - levels may be normal; diagnosis requires synovial fluid crystal analysis
- Most patients with septic arthritis are afebrile on presentation - do not use absence of fever to rule out infection
- Morning stiffness >1 hour is a hallmark of inflammatory arthritis (especially RA); stiffness lasting <30 minutes (gel phenomenon) suggests OA
- Acute monoarthritis can be the first presentation of systemic rheumatologic disease (e.g., RA, PsA, reactive arthritis) - always consider
- Drug-induced arthropathy is common - always take a thorough medication history
- Anti-CCP antibodies are more specific for RA than RF and may be positive years before clinical disease
Sources: Rosen's Emergency Medicine - Concepts and Clinical Practice (Ch. 102: General Approach to Arthritis); Firestein & Kelley's Textbook of Rheumatology (Ch. 42: Approach to the Patient with Arthritis)
This is a shared conversation. Sign in to Orris to start your own chat.