Vasculitis lung histopathology
Reading File
Finding Sources
Finding Sources
Searching PubMed
pulmonary vasculitis histopathology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the content needed for a comprehensive answer. Let me compile it.
Vasculitis: Lung Histopathology
Pulmonary vasculitis is defined histopathologically by cellular infiltration within vessel walls, vessel destruction, and tissue necrosis. The specific pattern varies by the type of vasculitis and the size of vessels involved.
General Principles of Lung Histopathology
Pulmonary vasculitis encompasses a spectrum of disorders "characterized histopathologically by the presence of a variety of types of cellular infiltration within vessel walls, vessel destruction, and ultimately tissue necrosis." The key general patterns are:
- Necrotizing vasculitis - fibrinoid necrosis of vessel walls
- Granulomatous inflammation - with or without giant cells
- Pulmonary capillaritis - the most common histologic expression of small vessel vasculitis in the lung
- Diffuse alveolar hemorrhage (DAH) - the clinical consequence of capillaritis
Important caveats: pathologic features overlap with necrotizing infections; prior corticosteroid treatment can abolish cellular infiltrates, leaving only arterial and airway scarring as the only histopathologic clue.
Pulmonary Capillaritis
Capillaritis is the hallmark histologic lesion of small vessel vasculitis in the lung and is nearly always present when DAH complicates ANCA-associated vasculitis (AAV).
Microscopic appearance:
- Alveolar septa disrupted by dense neutrophilic infiltrates
- Nuclear debris (karyorrhexis/leukocytoclasis) within septal walls
- Indistinct septal borders indicating wall damage
- Intra-alveolar red blood cells (DAH)
- Hemosiderin-laden macrophages in healing phase
- Plugs of organizing pneumonia may fill air spaces as lesions resolve
Figure 87.3 - Pulmonary capillaritis (Murray & Nadel):
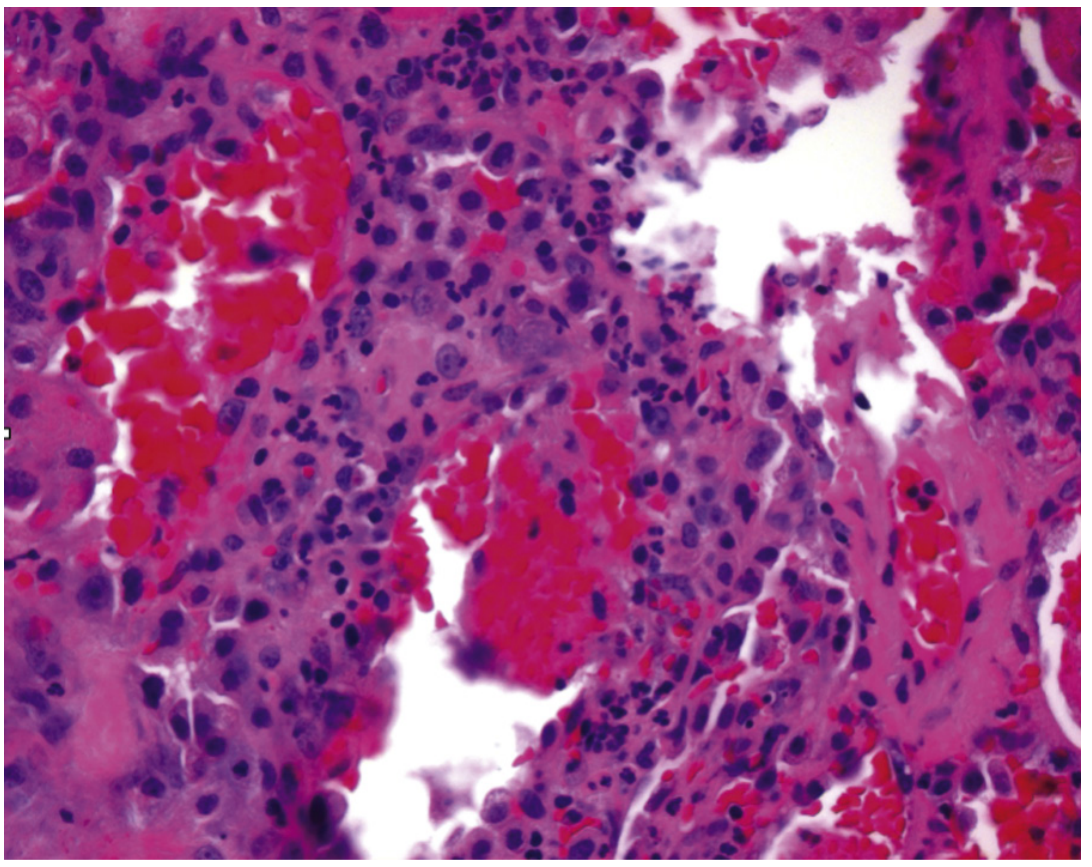
Alveolar septa are disrupted by infiltrates of neutrophils and nuclear debris. The septal borders are indistinct, indicating wall damage.
Granulomatosis with Polyangiitis (GPA / Wegener Granulomatosis)
GPA produces the most characteristic and complex lung histopathology among the vasculitides. The histopathology depends on disease stage and prior immunosuppressive treatment.
Three Major Histologic Features (all three required for classic pattern):
| Feature | Description |
|---|---|
| 1. Lung parenchymal necrosis | Geographic necrosis with irregular, serpiginous outlines, or neutrophilic microabscesses |
| 2. Vasculitis | Small-to-medium artery necrotizing vasculitis; also veins and capillaries; basophilic necrosis with surrounding chronic inflammation |
| 3. Granulomatous inflammation | Granulomas, giant cells (multinucleated), palisaded histiocytes; often with eosinophils, neutrophils, lymphocytes, and plasma cells (mixed cellular infiltrate) |
Minor Histologic Features:
- Organizing pneumonia (70% of cases)
- DAH/capillaritis (10% of cases)
- Eosinophilia
- Bronchocentric granulomatosis (1% of cases)
Immunofluorescence: Pauci-immune (no or minimal immune deposits)
Figure 87.7 - GPA lung histopathology (Murray & Nadel):

(A) Irregular "geographic" outline of parenchymal necrosis. (B) Low-power: branching necrotizing vessel (dashed outline). (C) Higher power: basophilic necrosis (arrow) with vague granulomas (inset). (D) Granulomatous adventitial inflammation with giant cells (arrows) around a pulmonary artery (PA).
From Fitzpatrick's Dermatology (open lung biopsy specimen):
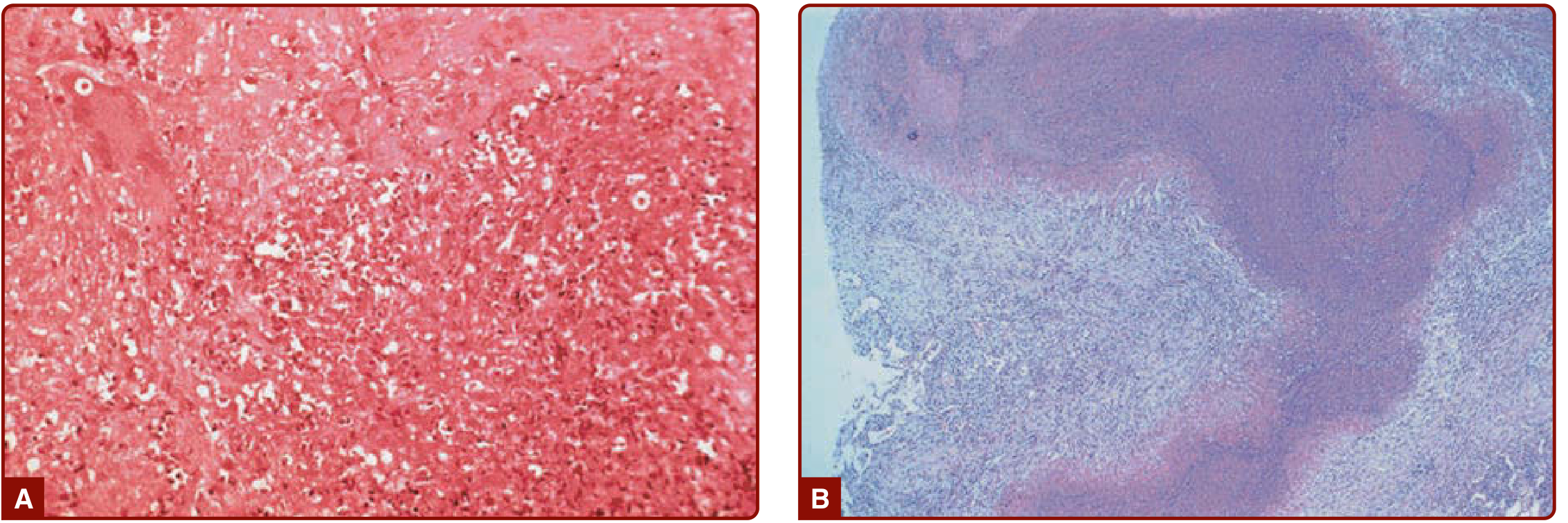
(A) Necrosis, giant cells, and mixed cellular inflammation. (B) "Geographic necrosis" on low-power view.
Eosinophilic Granulomatosis with Polyangiitis (EGPA / Churg-Strauss)
EGPA has a unique histologic triad on lung biopsy:
- Eosinophilic pneumonia - dense tissue eosinophilia filling alveolar spaces
- Necrotizing vasculitis - artery, vein, or capillary wall infiltrated by lymphocytes and eosinophils (eosinophil-predominant infiltrate, unlike the neutrophilic capillaritis of GPA/MPA)
- Granulomatous inflammation - granulomas with central necrosis containing abundant necrotic eosinophils, surrounded by palisaded histiocytes and multinucleated giant cells
Findings highly suggestive of EGPA (vs. other AAVs): eosinophilic pneumonia + parenchymal necrosis together.
Key differences from GPA: Eosinophilic (not neutrophilic) vascular wall infiltrate; eosinophilic pneumonia as background; less frequent DAH/glomerulonephritis.
Immunofluorescence: Also pauci-immune (MPO-ANCA positive in 30-70%)
Microscopic Polyangiitis (MPA)
MPA is the "simplest" histology among the AAVs:
- Focal, segmental necrotizing vasculitis affecting venules, capillaries, and arterioles
- Mixed inflammatory infiltrate - no granulomata (granuloma absence distinguishes MPA from GPA/EGPA)
- Neutrophilic capillaritis is the classic histologic finding in the lung
- DAH with intra-alveolar hemorrhage and hemosiderin-laden macrophages
- Healing produces organizing pneumonia-like patterns
Figure 87.9 - MPA lung histopathology (Murray & Nadel):
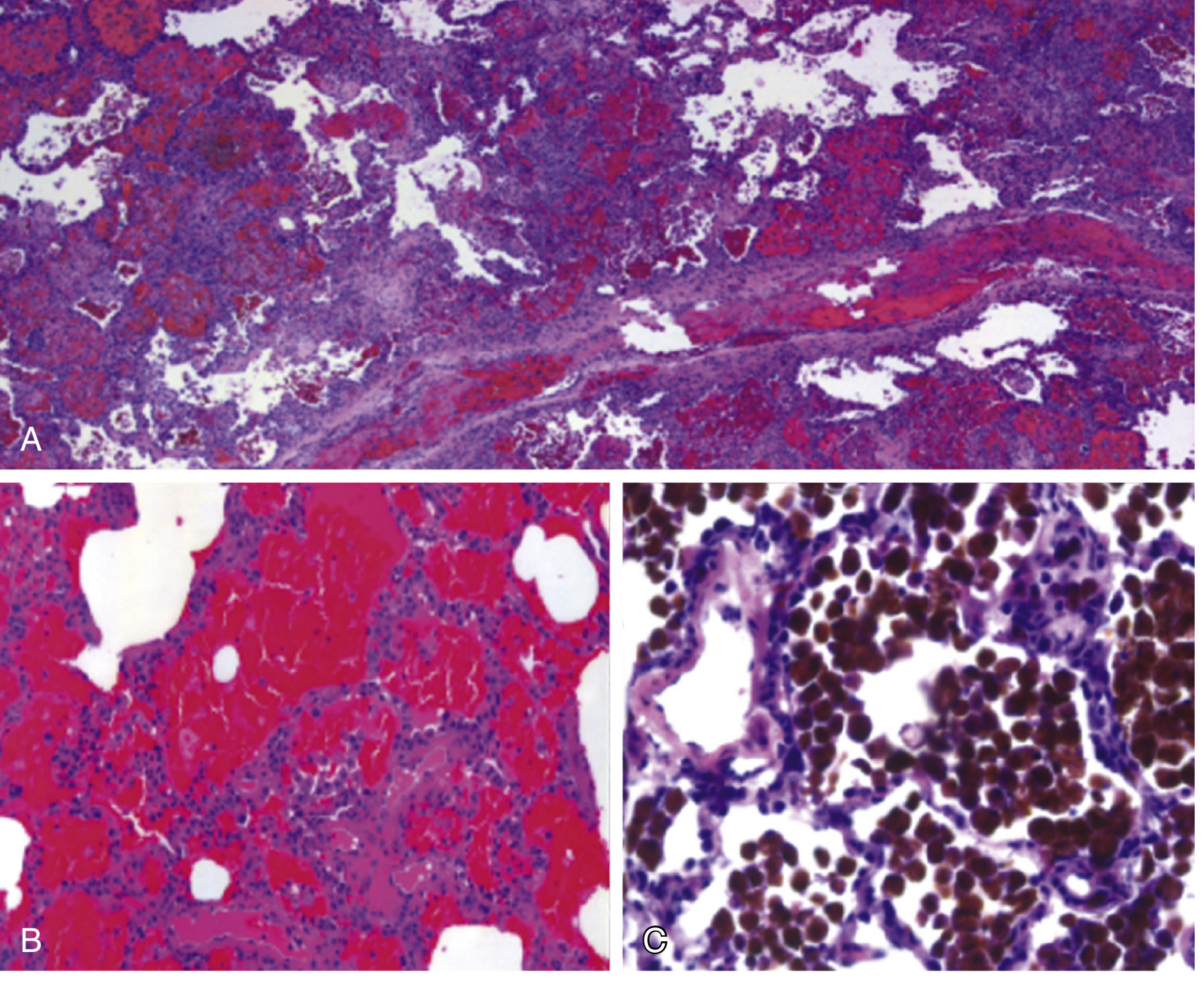
(A) Low-power: DAH with RBC-filled air spaces and inflammatory infiltrate. (B) Capillaritis and alveolar flooding. (C) Hemosiderin-laden macrophages (brown pigment) on iron stain.
Immune Complex-Mediated Vasculitides
These differ fundamentally from AAV by immunofluorescence pattern:
| Disease | IF Pattern | Key Histologic Clue |
|---|---|---|
| Anti-GBM (Goodpasture) | Linear IgG along GBM | Capillaritis + DAH |
| IgA vasculitis (HSP) | IgA deposits | Leukocytoclastic vasculitis |
| Cryoglobulinemic vasculitis | Irregular Ig + complement | Intraluminal cryoprecipitates |
| SLE/Sjögren/RA-vasculitis | Irregular IgG/IgM/complement | Background CTD changes |
| Polyarteritis nodosa | No glomerulonephritis | Medium vessel necrotizing arteritis, spares capillaries |
Comparative Summary Table
| Feature | GPA | EGPA | MPA |
|---|---|---|---|
| Vessel size | Small + medium arteries, veins, capillaries | Arteries, veins, capillaries | Venules, capillaries, arterioles |
| Infiltrate type | Neutrophilic + mixed | Eosinophilic | Neutrophilic |
| Granulomas | Yes (diagnostic) | Yes (with eosinophilic necrosis) | Absent |
| Geographic necrosis | Yes (hallmark) | Yes (with eosinophilic background) | No |
| Capillaritis/DAH | 10% | Uncommon | Classic (most common lung manifestation) |
| Immunofluorescence | Pauci-immune | Pauci-immune | Pauci-immune |
| ANCA | c-ANCA/PR3 (90-95% active) | p-ANCA/MPO (30-70%) | p-ANCA/MPO (50-75%) |
Biopsy Considerations
- Surgical (open) lung biopsy is the gold standard; transbronchial biopsy often non-diagnostic unless alveolar involvement is present
- Fresh tissue must be sent for culture (overlap with necrotizing infection), immunofluorescence (immune complex pattern), and formalin fixation (histology)
- Earlier biopsy = more likely to capture classic features; post-treatment biopsy may show only arterial/airway scarring
- Skin or kidney biopsy may establish the diagnosis and avoid lung biopsy
Sources: Murray & Nadel's Textbook of Respiratory Medicine (Chapter 87, pp. 1974-1990); Fishman's Pulmonary Diseases and Disorders (Chapter 68, pp. 1182-83); Fitzpatrick's Dermatology (Chapter 139, pp. 1689-97); Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.