
0ccfe031-db83-4729-8b9d-266feb514b70.jpeg
Solve
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have everything needed to give complete, well-referenced answers to all 5 questions. Here is the full solution:
Clinical Case Study - Subcapital Intracapsular Fracture of the Neck of Femur
Scenario recap: 75-year-old woman, fall in bathroom, right limb shortened + laterally rotated, X-ray = subcapital intracapsular fracture of femoral neck.
Question 1: Classify the types of fracture of the neck of the femur
Fractures of the femoral neck are classified in two main ways:
A. By Anatomical Site (location along the neck)
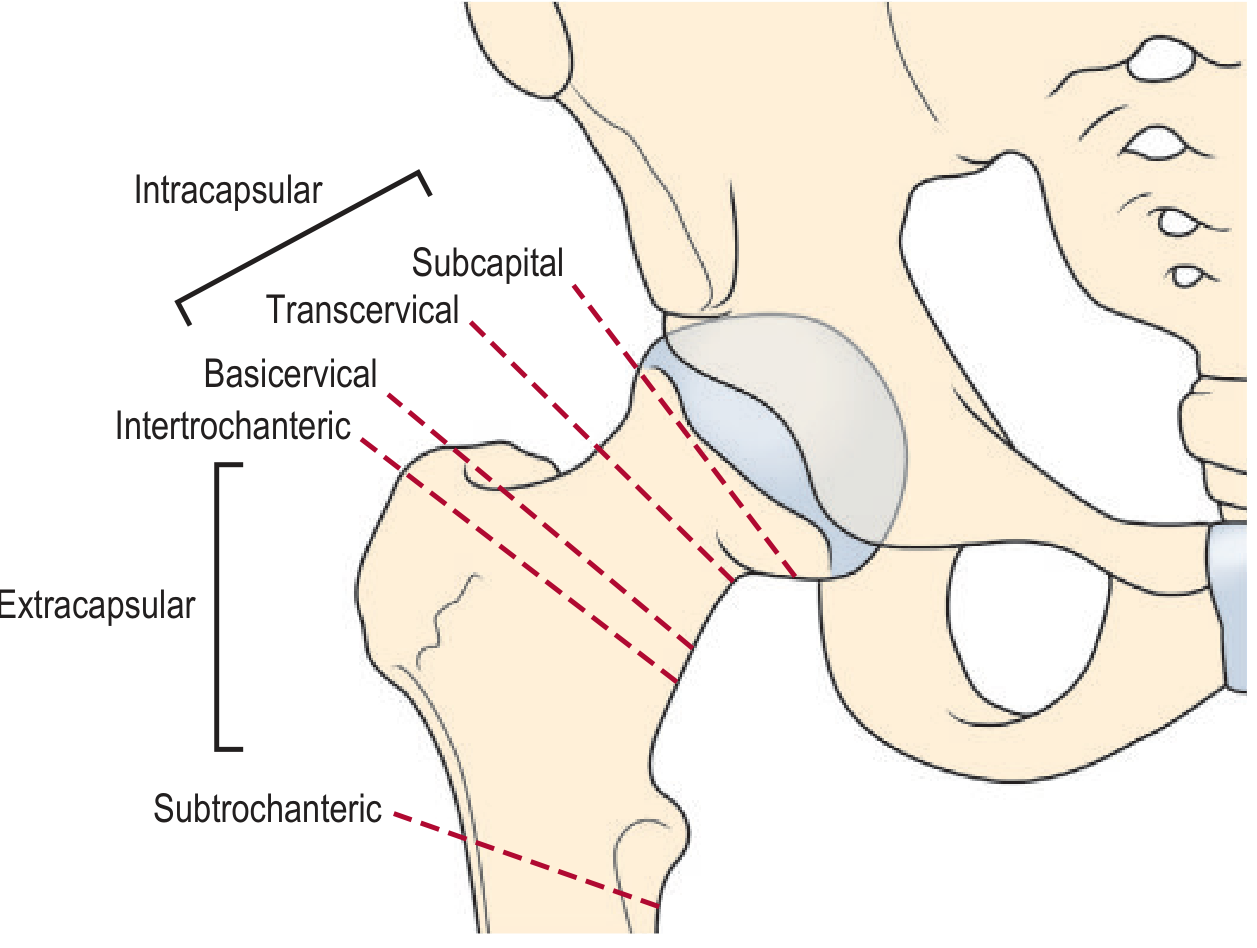
| Type | Location | Capsule relationship |
|---|---|---|
| Subcapital | Just below the femoral head | Intracapsular |
| Transcervical | Middle of the neck | Intracapsular |
| Basicervical | Base of the neck | Intracapsular (variable) |
| Intertrochanteric | Between the trochanters | Extracapsular |
| Subtrochanteric | Below the lesser trochanter | Extracapsular |
Subcapital, transcervical, and basicervical fractures are intracapsular; intertrochanteric and subtrochanteric are extracapsular.
B. By Displacement - Garden Classification (most widely used)
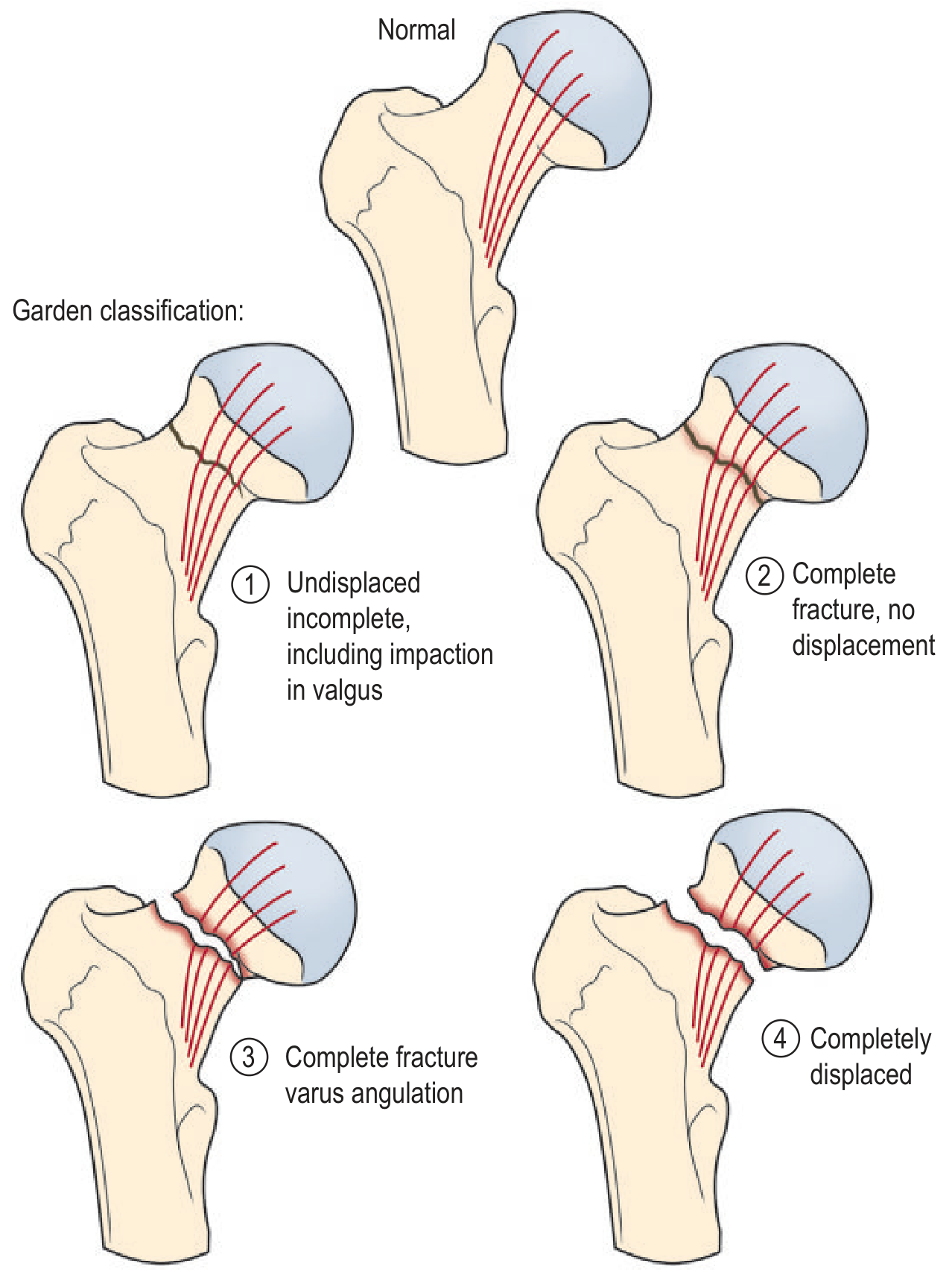
- Garden I - Undisplaced/incomplete; valgus-impacted; trabecular lines in femoral head angled relative to acetabulum
- Garden II - Complete, undisplaced; trabecular lines collinear with acetabulum
- Garden III - Complete, partially displaced with varus angulation; trabecular lines misaligned
- Garden IV - Completely displaced; head is free within acetabulum and realigns itself
C. By Angle of Fracture Line - Pauwels Classification
Based on the angle the fracture plane makes with the horizontal:
- Type I - Angle ≤ 30° (mostly horizontal, stable, good prognosis)
- Type II - Angle 30-50° (intermediate)
- Type III - Angle > 50° (nearly vertical, greatest shear forces, poor prognosis, high risk of nonunion)
This patient's fracture is a subcapital intracapsular fracture - the most common type in elderly women with osteoporosis.
(Rockwood and Green's Fractures in Adults, 10th ed.; Grainger & Allison's Diagnostic Radiology; S Das Manual of Clinical Surgery, 13th ed.)
Question 2: Anatomical basis of lateral rotation and shortening
The deformity (lateral/external rotation + shortening) is explained by muscle forces acting on the disconnected fragments:
Why external (lateral) rotation occurs:
- The iliopsoas, gluteus maximus, obturators, piriformis, and short external rotators all insert on or near the greater trochanter and the proximal femur.
- After the fracture, these muscles pull the distal fragment (shaft + lower limb) into external rotation unopposed, because the femoral head remains locked in the acetabulum.
- The foot therefore falls into external rotation - classically lying flat against the bed.
Why shortening occurs:
- The iliopsoas inserts on the lesser trochanter and pulls the shaft proximally.
- The adductors (adductor magnus, longus, brevis, gracilis, pectineus) pull the shaft medially and proximally.
- With loss of bony continuity at the neck, there is no resistance to upward displacement of the shaft, so the greater trochanter rides up and the limb shortens.
- Shortening can be confirmed clinically by Bryant's triangle and Nelaton's line - both show elevation of the greater trochanter.
In subcapital fractures specifically: the proximal fragment (femoral head) is held within the acetabulum, while the entire limb below the fracture rotates and shortens.
(S Das Manual of Clinical Surgery, 13th ed., p. 205)
Question 3: How is the length of the lower limb measured?
Two types of measurements are used:
True (Absolute) Limb Length
- Measured from the anterior superior iliac spine (ASIS) to the medial malleolus of the same side using a tape measure.
- This measures the actual bony length of the limb.
- Both limbs must be placed in identical positions (parallel to each other) before measurement.
Apparent (Relative) Limb Length
- Measured from the umbilicus (or xiphisternum) to the medial malleolus.
- This detects apparent shortening caused by pelvic tilt, adduction/abduction deformity, or scoliosis - not just bony shortening.
- In fracture neck of femur, both true and apparent shortening are present.
Clinical tip: Before measuring, any adduction or abduction deformity must be compensated for by positioning both limbs symmetrically. Shortening is expected in all hip fractures and dislocations, with the sole exception of the obturator type of anterior dislocation (which may show slight lengthening).
(S Das Manual of Clinical Surgery, 13th ed., p. 204)
Question 4: Possible complication of subcapital intracapsular fracture
The most important and feared complication is:
Avascular Necrosis (AVN) of the Femoral Head
- The blood supply to the femoral head travels via retinacular vessels closely applied to the femoral neck (branches of the medial and lateral circumflex femoral arteries).
- In a subcapital intracapsular fracture - especially displaced fractures (Garden III and IV) - these retinacular vessels are torn, cutting off the blood supply to the femoral head.
- AVN occurs in 15-35% of patients with displaced intracapsular fractures.
- The risk is greatest in Garden type 3 and 4 fractures.
Other complications include:
- Non-union - failure of the fracture to heal (common because the femoral head has poor blood supply even before AVN)
- Malunion - heals in a bad position
- Late osteoarthritis - due to joint damage and altered mechanics
- Deep vein thrombosis / pulmonary embolism - due to immobility in this elderly population (high mortality)
- Haemorrhage/shock - significant blood loss at fracture site
- Implant failure - if managed surgically
(Grainger & Allison's Diagnostic Radiology; S Das Manual of Clinical Surgery, 13th ed., p. 205)
Question 5: Clinical implications of the neck-shaft angle
The neck-shaft angle (also called the angle of inclination) is the angle between the long axis of the femoral neck and the long axis of the femoral shaft. The normal value is 125-140 degrees (commonly stated as ~130 degrees in adults).
Clinical significance:
| Condition | Angle | Implication |
|---|---|---|
| Normal | 125-140° | Normal abductor mechanics, limb alignment |
| Coxa valga | > 140° | Increased angle - may predispose to hip dislocation, increased shear at the neck |
| Coxa vara | < 125° | Decreased angle - causes a Trendelenburg gait, limb shortening, reduced abductor efficiency |
Relevance to fractures:
- The neck-shaft angle determines the biomechanical forces acting across a fracture. A more vertical fracture line (higher Pauwels angle combined with a varus neck-shaft angle) leads to greater shear forces at the fracture site, making fixation unstable and increasing risk of non-union.
- After fracture or surgical repair, the goal is to restore the normal neck-shaft angle to ensure proper abductor function and avoid Trendelenburg gait.
- Coxa vara (reduced neck-shaft angle) causes: relative shortening of the limb, inefficient hip abductors, Trendelenburg limp, and increased stress on the femoral neck.
(Rockwood and Green's Fractures in Adults, 10th ed., 2025; Rheumatology 2-Volume Set, Elsevier)
Summary for this patient: She has a classic presentation of a displaced subcapital intracapsular fracture of the neck of femur - an elderly osteoporotic woman, trivial fall, external rotation and shortening. The most urgent concern is disrupted blood supply to the femoral head, making AVN the most clinically significant complication. Management typically involves hemiarthroplasty or total hip replacement in an elderly independently mobile patient, or internal fixation for undisplaced fractures in younger patients.
This is a shared conversation. Sign in to Orris to start your own chat.