COPD
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"COPD" AND "pathophysiology"
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Chronic Obstructive Pulmonary Disease (COPD): Overview & Pathophysiology
Definition
The WHO defines COPD as "a common, preventable and treatable disease characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities caused by exposure to noxious particles or gases." The airflow limitation is largely irreversible, distinguishing it from asthma.
The GOLD (Global Initiative for Chronic Obstructive Lung Disease) criteria confirm diagnosis with spirometry: a post-bronchodilator FEV1/FVC ratio < 0.70.
COPD is an umbrella term that encompasses two major overlapping patterns of lung injury:
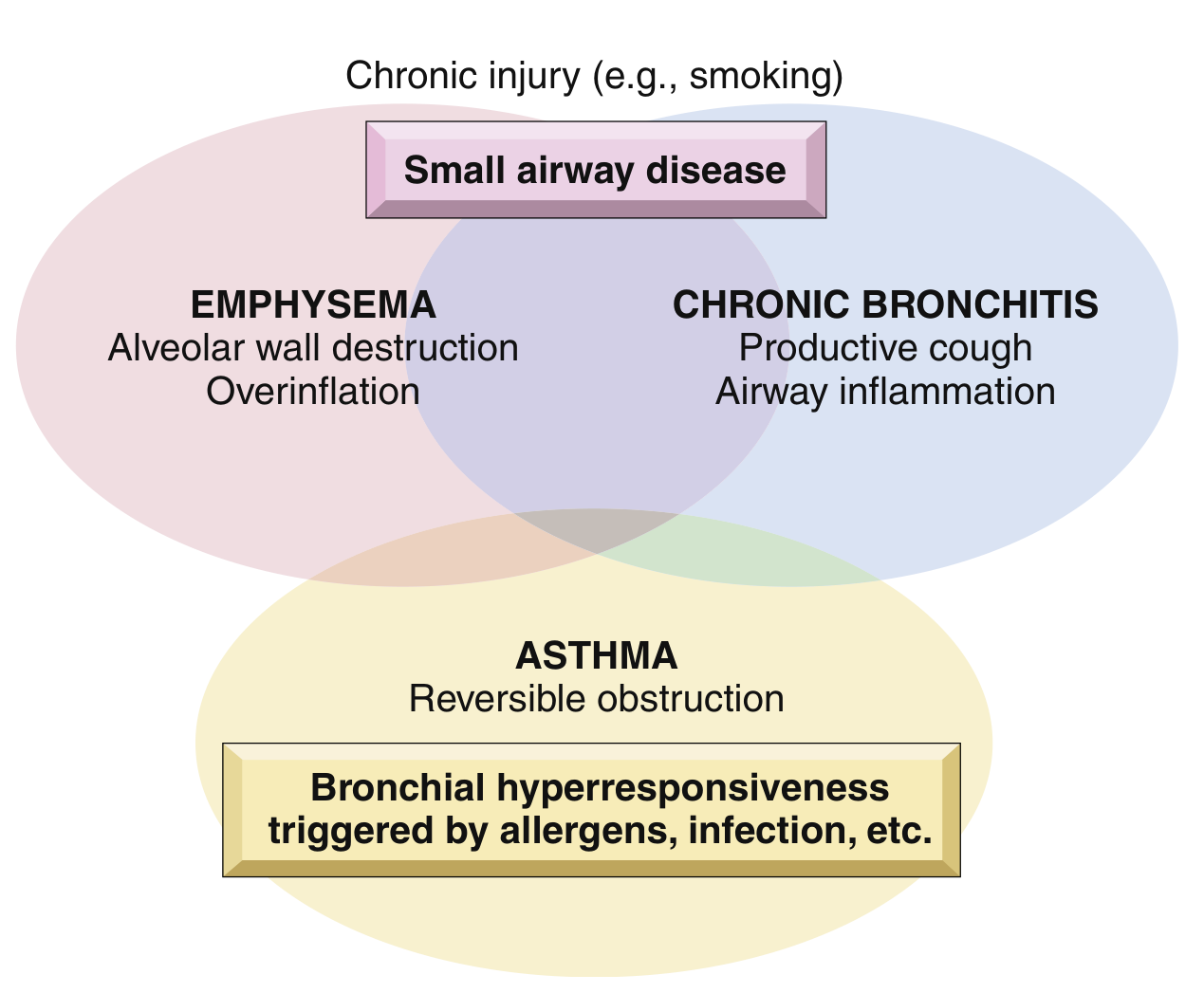
Fig. 11.4 - Schematic showing overlap between emphysema, chronic bronchitis, and asthma. (Robbins & Kumar Basic Pathology)
Epidemiology & Risk Factors
-
Affects >10% of U.S. adults over age 40; the 3rd leading cause of death worldwide
-
Smoking accounts for ~80% of all cases; 35-50% of heavy smokers develop COPD
-
Women appear more susceptible than men
-
Other risk factors:
- Poor lung development in early life
- Environmental/occupational pollutants (sulfur dioxide, nitrogen dioxide, dust)
- Airway hyperresponsiveness
- Genetic: α1-antitrypsin (AAT) deficiency (~1% of emphysema cases)
- Respiratory infections in childhood
-
Robbins & Kumar Basic Pathology, p. 447
Component Diseases
1. Emphysema
Emphysema is defined anatomically as permanent enlargement of air spaces distal to the terminal bronchioles, with destruction of alveolar walls but without significant fibrosis.
Four Patterns:
| Pattern | Location | Association |
|---|---|---|
| Centriacinar (centrilobular) | Central/proximal acinus; upper lobes | Cigarette smoking (most common, ~20x more frequent than panacinar) |
| Panacinar (panlobular) | Entire acinus uniformly; lower lobes | α1-antitrypsin deficiency |
| Distal acinar (paraseptal) | Distal acinus, near pleura | Young adults; spontaneous pneumothorax |
| Irregular | Irregular involvement | Scarring; usually clinically insignificant |
Morphology: Pale, voluminous lungs; histology shows destroyed alveolar walls without fibrosis and enlarged air spaces. Alveolar capillaries are diminished. Terminal and respiratory bronchioles deform due to loss of anchoring septa.
- Robbins & Kumar Basic Pathology, pp. 447-449
2. Chronic Bronchitis
Defined clinically (not anatomically) as a productive cough for at least 3 consecutive months in at least 2 consecutive years, in the absence of other explanations.
Key pathological feature: Hypersecretion of mucus from enlarged submucosal glands.
Reid Index: Ratio of mucous gland thickness to bronchial wall thickness. Normal ≤0.4. Raised (>0.4) in chronic bronchitis.
Morphology:
-
Hypertrophy of mucous glands in trachea and large bronchi
-
Goblet cell metaplasia in smaller bronchi and bronchioles
-
Inflammatory infiltrate: macrophages, neutrophils, lymphocytes (notably no eosinophils, unlike asthma)
-
Small airway disease (chronic bronchiolitis): mucous plugging, inflammation, submucosal fibrosis → luminal narrowing → airflow obstruction
-
Robbins & Kumar Basic Pathology, p. 449
Pathogenesis
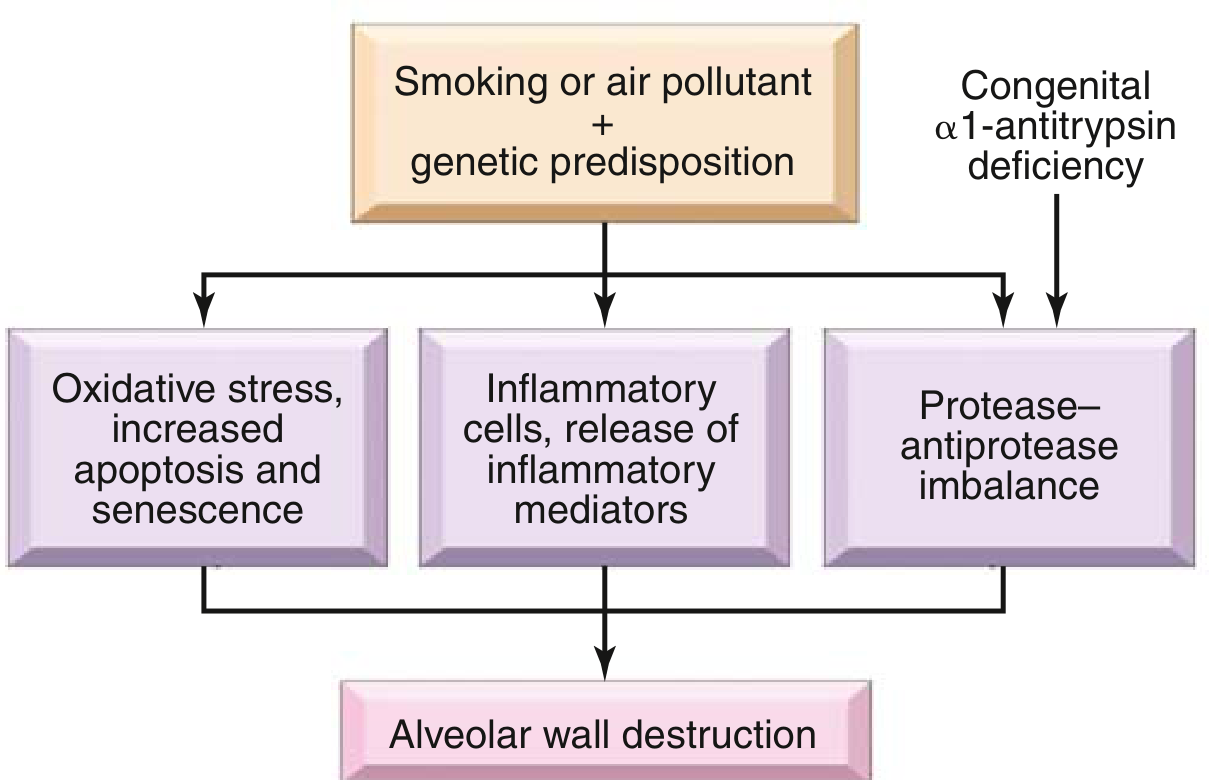
Fig. 11.6 - Pathogenesis of emphysema. (Robbins & Kumar Basic Pathology)
Three central mechanisms drive alveolar destruction:
1. Inflammatory Cells & Mediators
Cigarette smoke and noxious particles trigger innate and adaptive immune responses. Key mediators include:
- Leukotriene B4 and IL-8 (chemotactic for neutrophils)
- TNF-α and other proinflammatory cytokines
- Recruited cells: neutrophils, macrophages, CD4+ and CD8+ T cells
- Lymphoid follicles are increasingly recognized as central to COPD pathogenesis; lymphatic vessel density increases around alveolar spaces and correlates with disease severity
2. Protease-Antiprotease Imbalance
This is the cornerstone mechanism:
- Inflammatory cells release elastase and other proteases (matrix metalloproteinases) that degrade elastin and other extracellular matrix proteins
- Normally countered by α1-antitrypsin (AAT) - encoded at the Pi locus on chromosome 14
- Pi ZZ genotype (homozygous Z allele, ~0.01% of U.S. population): markedly reduced AAT → panacinar emphysema at an earlier age, worsened by smoking
- Loss of alveolar elastic tissue reduces radial traction on respiratory bronchioles → dynamic airway collapse during expiration → functional airflow obstruction even without mechanical blockage
3. Oxidative Stress
- Reactive oxygen species (ROS) in cigarette smoke cause direct tissue damage
- ROS also stimulate macrophages and neutrophils to release more ROS (amplification loop)
- Oxidative stress drives increased apoptosis and cellular senescence of structural lung cells
Airway Infection
-
Not involved in disease initiation
-
Bacterial/viral infections trigger acute exacerbations by sustaining inflammation
-
Robbins & Kumar Basic Pathology, pp. 447-449
Mechanisms of Airflow Obstruction
COPD causes obstruction through two main mechanisms:
| Mechanism | Component |
|---|---|
| Loss of alveolar elastic recoil (radial traction) → dynamic collapse of small airways on expiration | Emphysema |
| Airway narrowing due to mucous plugging, goblet cell metaplasia, inflammation, and submucosal fibrosis | Chronic bronchitis / small airway disease |
Functional Consequences
- Spirometry: Reduced FEV1, normal or near-normal FVC → reduced FEV1/FVC ratio (< 0.70)
- Air trapping → hyperinflation → barrel chest, flattened diaphragm on imaging
- Ventilation-perfusion (V/Q) mismatch → hypoxemia
- In advanced disease: hypercapnia (hypoventilation)
- Chronic hypoxemia → pulmonary vasoconstriction → pulmonary hypertension → cor pulmonale
- Mild PH is common in stable COPD; severe PH (mPAP ≥ 40 mmHg) is rare (~1-3%)
Classic Clinical Phenotypes
| Feature | "Pink Puffer" (Emphysema dominant) | "Blue Bloater" (Chronic bronchitis dominant) |
|---|---|---|
| Build | Thin, cachectic | Overweight |
| Cough | Minimal | Productive, chronic |
| Dyspnea | Prominent | Less prominent early |
| Gas exchange | Relatively preserved until late | Hypoxemia + hypercapnia |
| Cyanosis | Absent | Present |
| Cor pulmonale | Late | Earlier |
| OSA risk | Lower (lower BMI, hyperinflation) | Higher (higher BMI, lower respiratory drive) |
- Murray & Nadel's Textbook of Respiratory Medicine, p. 2747
Key Comorbidities & Systemic Effects
- OSA-COPD Overlap Syndrome: ~1% of general population; at higher risk for hypercapnia, PH, and COPD exacerbations. CPAP improves survival and reduces hospitalizations in overlap patients.
- Weight loss / cachexia: Common; can mimic occult malignancy
- Pulmonary hypertension: Primarily due to hypoxic vasoconstriction
- Right heart failure (Cor pulmonale)
- Sleep-related hypoventilation: REM sleep causes accessory muscle paralysis, worsening hypoxemia and hypercapnia in advanced COPD
Sources:
- Robbins & Kumar Basic Pathology, pp. 447-450
- Murray & Nadel's Textbook of Respiratory Medicine (2-Volume), pp. 179, 2747
- Fishman's Pulmonary Diseases and Disorders (2-Volume Set)
This is a shared conversation. Sign in to Orris to start your own chat.