
IMG-20251119-WA0011.jpg
Analysis and diagnosis and mark , details
Reading File
Finding Sources
Searching the Web
short PR interval ECG 116ms WPW pre-excitation diagnosis criteria
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
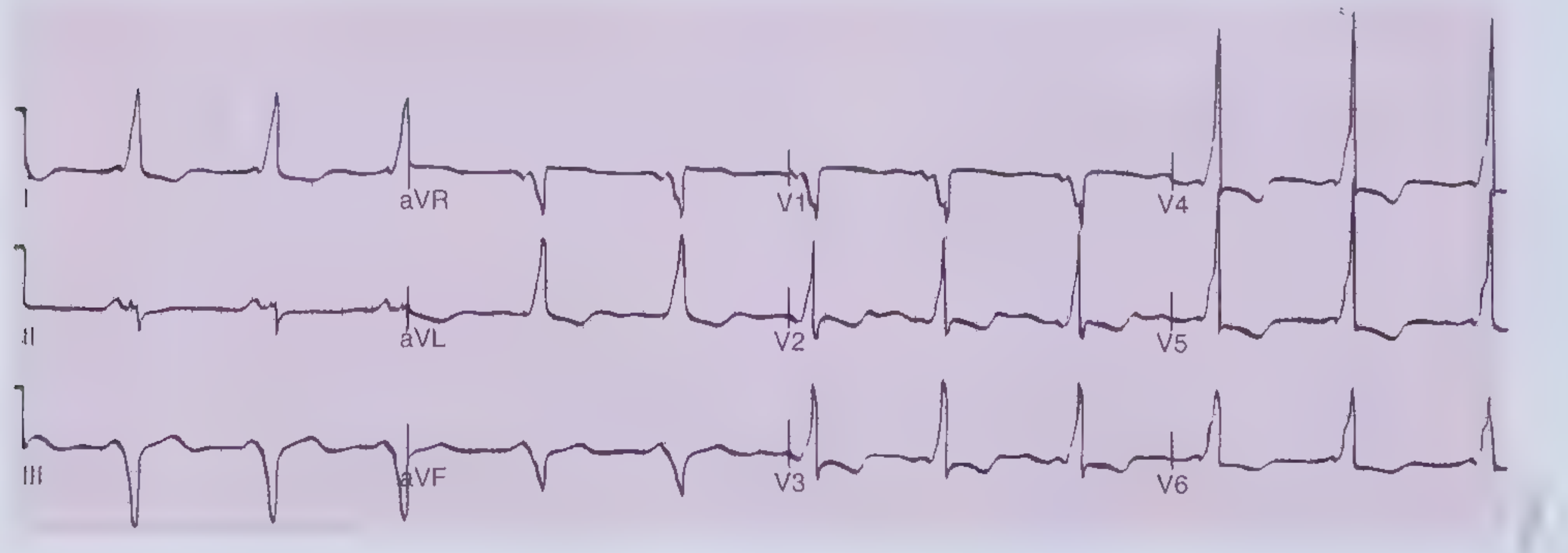
Here is the detailed ECG analysis and diagnosis:
ECG Analysis - Detailed Report
Machine Measurements (GE MAC1200 ST - Ruban Hospital)
| Parameter | Value | Normal Range |
|---|---|---|
| Heart Rate | 64 bpm | 60-100 bpm - Normal |
| QRS Duration | 74 ms | <120 ms - Normal |
| QT / QTcB | 412 / 426 ms | QTc <440 ms - Normal |
| PR Interval | 116 ms | <120 ms - SHORT |
| P wave duration | 66 ms | Normal |
| RR / PP | 934 / 940 ms | Normal |
| QRS Axis | -5° (near normal) | -30° to +90° |
| Sokolow Index | 1.8 mV | <3.5 mV - Normal |
Key Findings on Visual ECG Review
1. Short PR Interval - 116 ms
- Normal PR is 120-200 ms (3-5 small squares at 25 mm/s)
- This ECG shows PR = 116 ms, which is borderline short / below normal
- The machine itself flags: "short PR interval"
2. QRS Morphology Assessment
- QRS duration is narrow at 74 ms (normal)
- No frank delta wave with the classic broad, slurred upstroke is prominently visible in this tracing - the QRS appears relatively narrow
- This is an important distinction from classic WPW
3. Rhythm
- Regular sinus rhythm at 64 bpm
- P waves present and conducting normally
4. No ST-T Changes
- No ST elevation or depression
- No T wave inversion
Differential Diagnosis for Short PR Interval
| Condition | PR | QRS | Delta Wave | This ECG |
|---|---|---|---|---|
| WPW (manifest) | Short <120 ms | Wide >120 ms | Present | QRS is narrow (74ms) - does NOT fully fit |
| LGL Syndrome | Short <120 ms | Narrow | Absent | Fits pattern |
| Enhanced AV nodal conduction | Short | Narrow | Absent | Possible |
| Normal variant / vagal tone | Low-normal | Normal | Absent | Possible |
Most Likely Diagnosis
Lown-Ganong-Levine (LGL) Syndrome / Enhanced AV Nodal Conduction
This ECG shows:
- Short PR (116 ms) - below the 120 ms cutoff
- Narrow QRS (74 ms) - rules out classic WPW
- No visible delta wave
- Machine correctly reports: "short PR interval, probably normal ECG"
This pattern fits LGL syndrome or simply enhanced AV nodal conduction - where an accessory pathway (James fibers) bypasses the slow part of the AV node but inserts into the bundle of His, producing a short PR with a normal, narrow QRS and no delta wave.
Compare with the classic WPW reference ECG below (from Frameworks for Internal Medicine), which shows the broad slurred delta wave and wide QRS that this patient does NOT have:
Clinical Implications
- LGL/short PR with narrow QRS: associated with paroxysmal supraventricular tachycardia (PSVT) - the patient may have episodes of sudden palpitations
- Risk is considerably lower than WPW with delta wave (no risk of rapid pre-excited atrial fibrillation)
- If symptomatic (palpitations, syncope): Holter monitoring, event recorder, or electrophysiology study (EPS) are next steps
- If asymptomatic: No immediate treatment needed; reassurance and follow-up
Summary Box
ECG Diagnosis: Sinus rhythm, 64 bpm | Short PR interval (116 ms) with narrow QRS - consistent with LGL pattern / enhanced AV conduction | No delta wave | No ischemic changes | QTc normalMachine interpretation: "Short PR interval - probably normal ECG" - partially correct; the short PR should be clinically correlated with symptoms
Note: This ECG report is marked "Unconfirmed report" by the machine (standard automated disclaimer). Clinical correlation with patient symptoms is mandatory. If the patient has palpitations or syncope, further electrophysiologic workup is warranted.
- Braunwald's Heart Disease, A Textbook of Cardiovascular Medicine - WPW/pre-excitation section
- Frameworks for Internal Medicine - AVRT and accessory pathway criteria
This is a shared conversation. Sign in to Orris to start your own chat.